0855
Diagnostic Accuracy of Zero Echo Time Magnetic Resonance Imaging for Grading of Cervical Spine Neural Foraminal Stenosis1Department of Radiology and Imaging, Hospital for Special Surgery, New York, NY, United States
Synopsis
A challenge for orthopaedic radiologists is utilizing MRI to assess neuroforaminal (NF) stenosis of the cervical spine as cortical bone does not display with sufficient signal intensity. This study utilized zero echo time (ZTE) imaging to visualize the cervical spine and compare evaluation of NF stenosis to corresponding CT imaging. Substantial agreement was found between ZTE and CT (κ=0.71). ZTE tended to underestimate stenotic grade in 25% of foramina, with a majority (66%) of differences within one grading level. Further development of ZTE and image processing may minimize the need for cervical spine CT in assessing NF stenosis.
Introduction
Direct visualization of cortical bone with magnetic resonance imaging (MRI) is challenging. Generating sufficient positive image contrast is limited as the highly organized tissue ultrastructure results in very short T2 values that preclude acquisition of sufficient signal intensity. As a result, cortical bone is normally displayed as a dark structure in generated images. Proton density zero echo time (ZTE) imaging permits visualization of tissues with very short transverse relaxation times, such as cortical bone, and is capable of displaying images with CT-like contrast1,2. ZTE imaging has been used to visualize cortical bone in the cranium (1,2) and lower extremities (3), but the direct clinical utility of this novel acquisition for visualization of cortical bone has yet to be determined. A major challenge for orthopaedic radiologists is utilizing MRI to assess the degree of neural foraminal (NF) stenosis of the cervical spine. Conventional assessment is inherently flawed as it is performed using T2-weighted, 2D axial images obtained parallel to the disc space and not orthogonal to the neural foramen. Additionally, the margins of osseous uncovertebral ridges that contribute to NF stenosis are difficult to define from standard MR images. As such, computed tomography (CT) is routinely obtained by spine surgeons for pre-operative planning, as 1) CT images can be easily reformatted into an oblique sagittal plane orthogonal to the foramen and 2) CT images better define mineralized disc material and/or ridges which may need to be addressed surgically. The purpose of this study was to demonstrate the use of 3D ZTE imaging of the cervical spine to assess osseous NF stenosis. It was hypothesized that ZTE imaging would yield NF stenosis scores comparable to CT.Methods
Twenty-nine patients (18F/11M), aged 58.7 ± 12.5 years (mean ± SD), in this IRB-approved study were enrolled consecutively from a clinical cohort of patients receiving standard-of-care MRI in our radiology department. All patients had a cervical spine CT obtained or scheduled (and later completed), within 1 month of MRI without intervening surgery (median time of scan separation = 0 days). All MRI scans were performed on a clinical 3T scanner (DV750, GE Healthcare, Waukesha, WI) using either a 8 or 32 channel HNS coil with these acquisition parameters: TE/TR: 0ms/300ms, flip angle: 1°, bandwidth: ± 62.5 kHz, NEX: 2-4 , voxel size: 1 mm3, scan time: ~5 mins. ZTE and CT images were reviewed in a blinded fashion during separate interpretation sessions. The isotropic ZTE dataset was reformatted to generate double oblique images that aligned the imaging plane perpendicular to each neural foramen. A 6 point scale (none, mild, mild/moderate, moderate, moderate/severe, severe) was used to bilaterally grade NF stenosis at intervertebral levels C2-C3 through C7-T1 ( total of 12 grades/patient). Statistical Analysis: Weighted Kappa statistics were used to assess agreement between ZTE and CT grades (SAS V.9.3, Cary, NC). Significance was set at p < 0.05.Results
Substantial agreement in NF stenosis grade for 339 foramina was found between corresponding CT and ZTE scans: κ = 0.71 (95% CI: 0.66 to 0.76). Perfect agreement was found in 63% of evaluated foramina, with ZTE grading tending to underestimate stenotic grade (25% of foramina). A majority (66%) of differences between the imaging techniques were within 1 grading level.Discussion
The ability to evaluate osseous detail is necessary for radiological assessment of cervical NF stenosis, and many patients require CT and MRI for effective diagnosis and preoperative planning. Results reveal similar NF grading between ZTE and CT evaluation, with slight underestimation of severity on ZTE images. Estimation differences in NF grade are likely due to disparate spatial resolutions (1mm3 in ZTE vs. 0.2x0.2x0.3 mm3 in CT). Further assessment in larger cohorts, with inter-/intra-observer comparisons as well as evaluation of stenosis with only standard MRI, are currently underway to further support the utility of ZTE imaging of the cervical spine.Conclusion
ZTE MRI permits visualization of osseous cervical anatomy, and with continued MRI sequence and processing improvements ZTE may soon obviate the need for cervical spine CT and its associated ionizing radiation and additional cost.Acknowledgements
The authors would like to acknowledge Jung Joo, RT-MRI, for his assistance with MRI scanning. HSS has an institutional research agreement in place with GE Healthcare.References
1. Delso G, Wiesinger F, Sacolick LI, Kaushik SS, Shanbhag DD, Hullner M, Veit-Haibach P. Clinical evaluation of zero-echo-time MR imaging for the segmentation of the skull. J Nucl Med 2015;56(3):417-422.
2. Johnson EM, Vyas U, Ghanouni P, Pauly KB, Pauly JM. Improved cortical bone specificity in UTE MR Imaging. Magn Reson Med 2016.
3. Larson PE, Han M, Krug R, Jakary A, Nelson SJ, Vigneron DB, Henry RG, McKinnon G, Kelley DA. Ultrashort echo time and zero echo time MRI at 7T. MAGMA 2016;29(3):359-370.
Figures
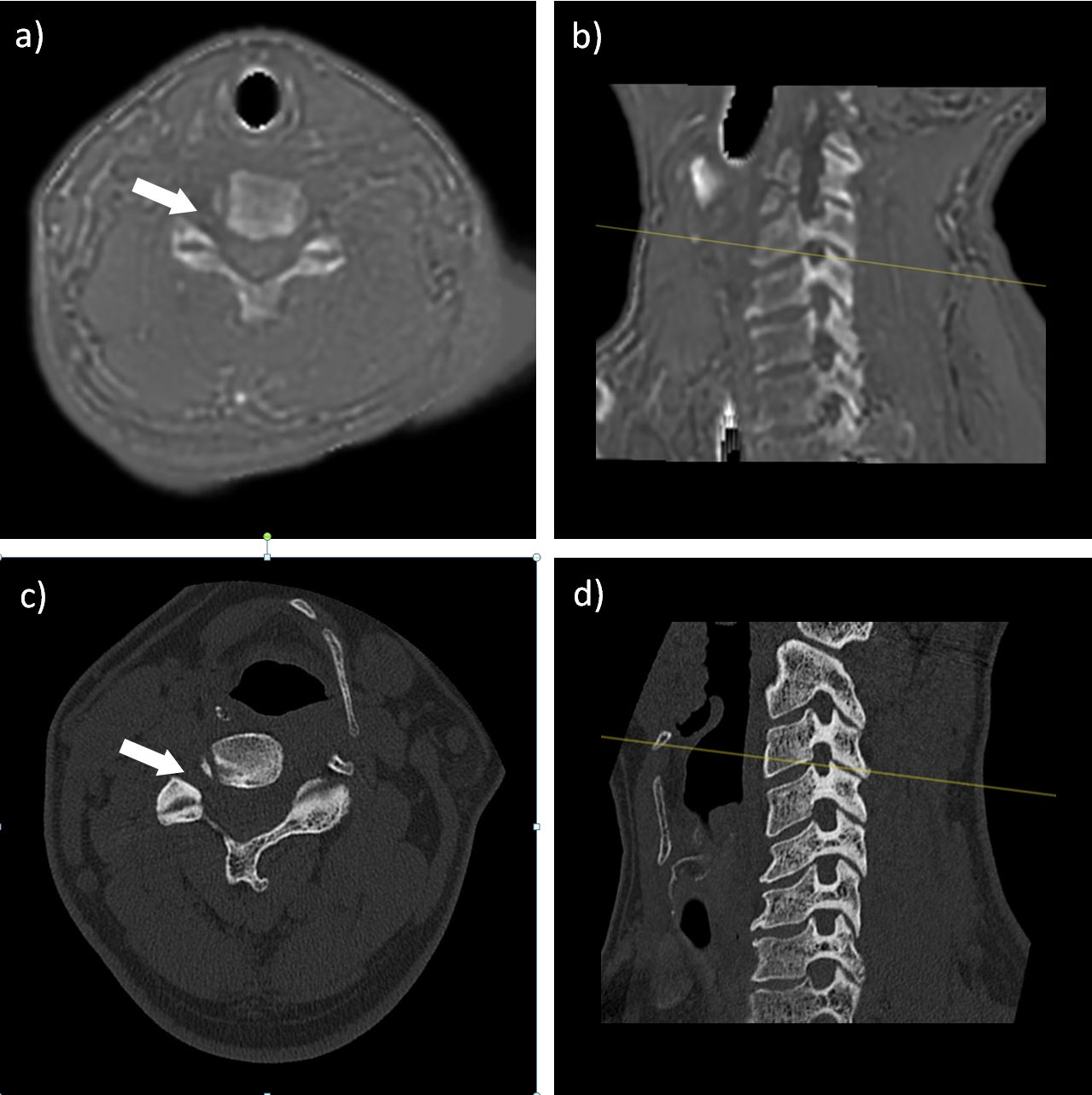
Figure 1. Axial (a) and double-oblique (b) ZTE images, and axial (c) and double-oblique (d) CT of a 38 year old male at the C4-5 level demonstrating no stenosis (white arrows).Yellow lines are cross references for corresponding axial slices.
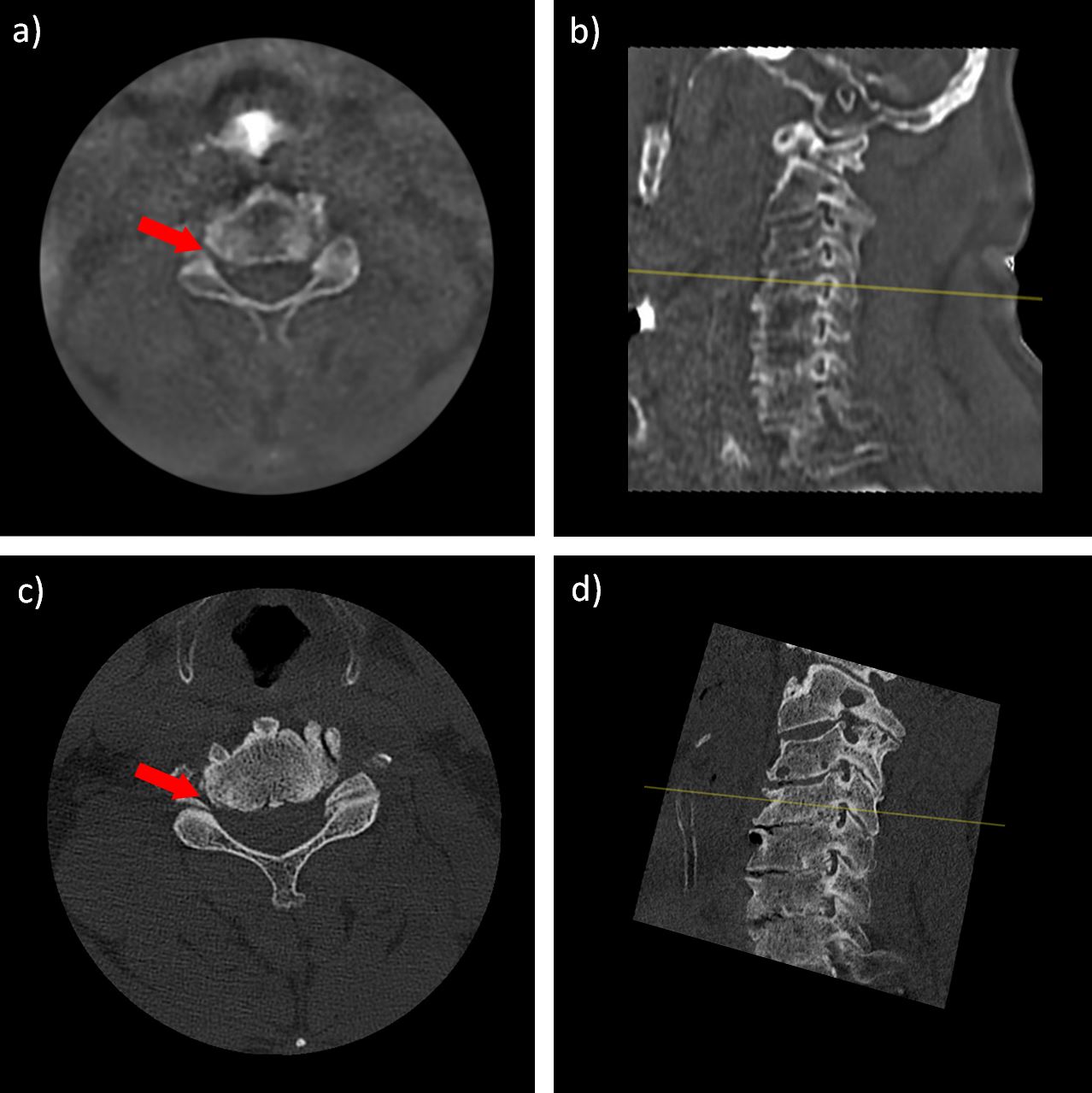
Figure 2. Axial (a) and double-oblique (b) ZTE images, and axial (c) and double-oblique (d) CT of a 71 year old male at the C4-5 level exhibiting severe stenosis (red arrows). Yellow lines are cross references for corresponding axial slices.