0853
MRI quantification of diffusion and perfusion in epiphysis of femoral heads after close reduction of children with DDH by intravoxel incoherent movement1Radiology, Tian Jin Hospital, Tian Jin, People's Republic of China, 2MR Research China, GE Healthcare, People's Republic of China, 3Pediatric Orthopedics, Tian Jin Hospital, Tian Jin, People's Republic of China
Synopsis
Developmental dysplasia of the hip (DDH) is a common disease of the development of hips. Some children with DDH need close reduction followed by immobilization in spica casting, but excessive hip abduction may lead to avascular necrosis of the epiphysis of femoral head. Therefore, this study would like to use IVIM method to help the pediatric orthopaedic doctors to know whether the blood supply of epiphysis of femoral heads is insufficiency or not in patients with DDH after close reduction.
Purpose
Developmental dysplasia of the hip (DDH) includes acetabular dysplasia, delay development or necrosis of femoral heads, subluxation or dislocation of hip joints, is a common disease of the development of hips [1]. Some children with DDH need close reduction followed by immobilization in spica casting, however, excessive hip abduction may lead to avascular necrosis of the epiphysis of femoral heads[2]. Therefore, finding a reliable method to evaluate the blood supply of the epiphysis of femoral head is paramount. Some authors utilized contrast enhanced MRI to study the blood flow of the femoral head[3]. But it involved the MRI contrast agent, which may lead many adverse effects on patients, especially on children [4, 5]. In consequence, it’s urgent to find a noninvasive method to evaluate the perfusion of the epiphysis of the femoral head. Intravoxel incoherent motion (IVIM) can separately measure the pure diffusion coefficient (ADCslow), perfusion-related incoherent microcirculation (ADCfast) and the microvascular volume fraction (f), which avoiding the exogenous contrast agents injection [6, 7]. In this study, we would like to use IVIM method to measure and compare the perfusion and diffusion situation between DDH sides and normal sides of the epiphysis of femoral heads in patients with DDH after close reduction.
Methods
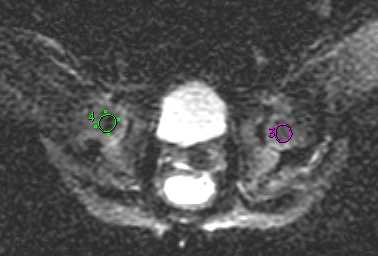
The prospective study was reviewed by the ethics committee of the hospital. All recruited patients’ legal guardians signed written informed consent. Twenty-eight patients (3 boys and 25 girls, age range: 6-24 months, average age: 16.14±7.62 months) with DDH and performed close reduction and spica casting of hip joints were recruited in this study. The DDH sides of hips were treated as lesion group, and the normal sides of hips as control group. The MRI examinations were performed on a 3-T MRI scanner (MR750, GE Healthcare) with an 8-channel cardiac coil immediately after the close reduction. The IVIM data was acquired by a multi-b single shot SE-EPI pulse sequence with the following parameters: TR/TE=2000/77.4 ms, acceleration factor 2, slice thickness 2.5 mm with 1.0 mm gap and FOV 300×300 mm2, matrix size 160×192. For each subject, eleven b-values set at (number of excitation): 0(2), 10(4), 30(4), 50(4), 80(4), 120(4), 200(4), 500(6), 800(6), 1300(8) and 2000 (8) s/mm2 were acquired. Region of interest was placed on the epiphysis of both femoral heads on the b=0 DWI image (As shown in Fig 1). The ADCslow, ADCfast, f, and ADCfast×f were measured on each ROI. Two radiologists measured the data separately. The intraclass correlation coefficient (ICC) was calculated to assess the variability of data for the two observers. Mann-Whitney U test was performed to compare the values of ADCslow, ADCfast, f, and ADCfast×f between lesion group and control group (P values<0.05). Receiver operating characteristic (ROC) curves were generated with respective cut-off values determined to accommodate best diagnostic accuracy based on the Youden index.Results
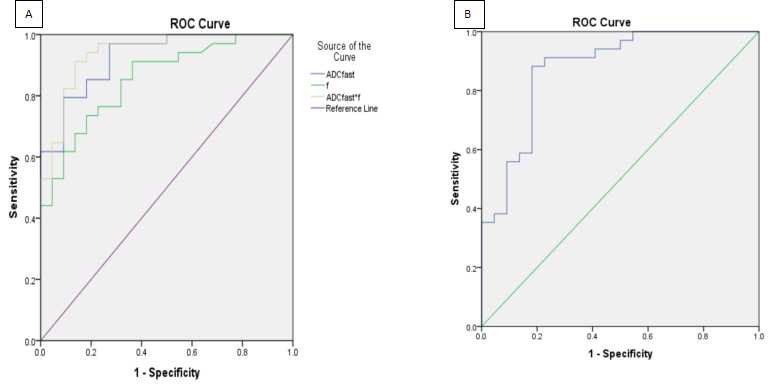
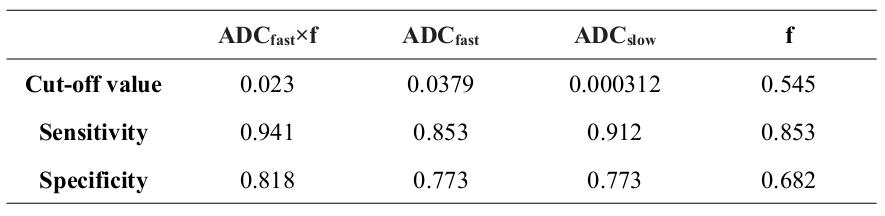
The ICC of ADCslow was 0.989 (P=0.036), ADCfast was 0.999 (P=0.000), f was 0.993 (P=0.009) and ADCfast×f was 0.996 (P=0.005), showed excellent inter-observer agreement. The values of ADCslow in lesion group were significantly higher than in control group. However, the values of the ADCfast, f and ADCfast×f in lesion group were significantly lower than in control group. As shown in Fig 2, the ADCfast×f value was the most powerful parameter, with area under the curve (AUC) of 0.940, followed by ADCfast 0.926, but ADCslow and f value were less powerful, with AUC of 0.876 and 0.855(P=0.000), respectively. The optimal cut-off values of ADCfast×f, ADCfast, ADCslow, and f were summarized in Table 1.Discussion
The ADCfast, f, and ADCfast×f were lower in DDH sides of the hip joints than in the controls. It suggests that when patients with DDH having dislocation of hip joints or close reduction, the medial circumflex artery and the small vessels in the femoral epiphysis may be compressed, resulting in occlusion of the blood supply of epiphysis of femoral heads. The insufficiency of blood supply of epiphysis of femoral heads, granulation tissue formation and inflammatory cells infiltrates in the epiphysis probably gain more space for water molecules diffusion [8], which appears as increased ADCslow.Conclusion
IVIM is a promising non-invasive method to investigate the perfusion and diffusion of epiphysis of femoral heads in patients with DDH. Lower ADCfast, f, and ADCfast×f suggest the insufficiency of blood supply of the epiphysis of the femoral head in patients with DDH after close reduction, higher ADCslow suggests bone absorption, granulation tissue formation and inflammatory cells infiltration in the epiphysis. The ADCfast×f value has the most powerful sensitivity and specificity to predict blood supply insufficiency.
Acknowledgements
NoneReferences
[1]. Bracken. J., T. Tran and M. Ditchfield, Developmental dysplasia of the hip: Controversies and current concepts. Journal of Paediatrics and Child Health, 2012. 48(11): p. 963-973.
[2]. Kruczynski.J., et al., Avascular necrosis of the proximal femur in developmental dislocation of the hip. Incidence, risk factors, sequelae and MR imaging for diagnosis and prognosis. Acta Orthop Scand Suppl, 1996. 268: p. 1-48.
[3]. Tiderius. C., et al., Post-closed reduction perfusion magnetic resonance imaging as a predictor of avascular necrosis in developmental hip dysplasia: a preliminary report. J Pediatr Orthop, 2009. 29(1): p. 14-20.
[4]. Sebag, G., et al., Dynamic gadolinium-enhanced subtraction MR imaging--a simple technique for the early diagnosis of Legg-Calve-Perthes disease: preliminary results. Pediatr Radiol, 1997. 27(3): p. 216-20.
[5]. Du J, et al., MR perfusion index as a quantitative method of evaluating epiphyseal perfusion in Legg-Calve-Perthes disease and correlation with short-term radiographic outcome: a preliminary study. J Pediatr Orthop, 2013. 33(7): p. 707-13.
[6]. Du, J., et al., Intravoxel Incoherent Motion MR Imaging. Medicine, 2015. 94(25): p. e1028.
[7]. Wurnig. M.C., et al., Systematic analysis of the intravoxel incoherent motion threshold separating perfusion and diffusion effects: Proposal of a standardized algorithm. Magnetic Resonance in Medicine, 2015. 74(5): p. 1414-1422.
[8]. Boutault. J.R., et al., Diffusion MRI of the neck of the femur in Legg-Calve-Perthes disease: A preliminary study. Diagnostic and Interventional Imaging, 2013. 94(1): p. 78-83.
Figures