0849
Zero Echo Time MRI: Osseous Shoulder Imaging1Radiology and Imaging, Hospital for Special Surgery, New York, NY, United States, 2Sports Medicine, Hospital for Special Surgery, New York, NY, United States
Synopsis
Routine MRI fails to provide direct visualization of bone due to the short tissue relaxation times and limited signal intensity. This study investigates the use of proton density zero echo time (ZTE) MRI for bone in the shoulder. Shoulder CT and ZTE images were acquired for 31 patients. Five measures of osseous defect and lesion sizes were compared between the two modalities. ‘Fair’ to ‘excellent’ intraobserver agreement was observed between CT and ZTE MRI. Zero Echo Time MRI may obviate the need for additional CT evaluation in some cases.
Introduction
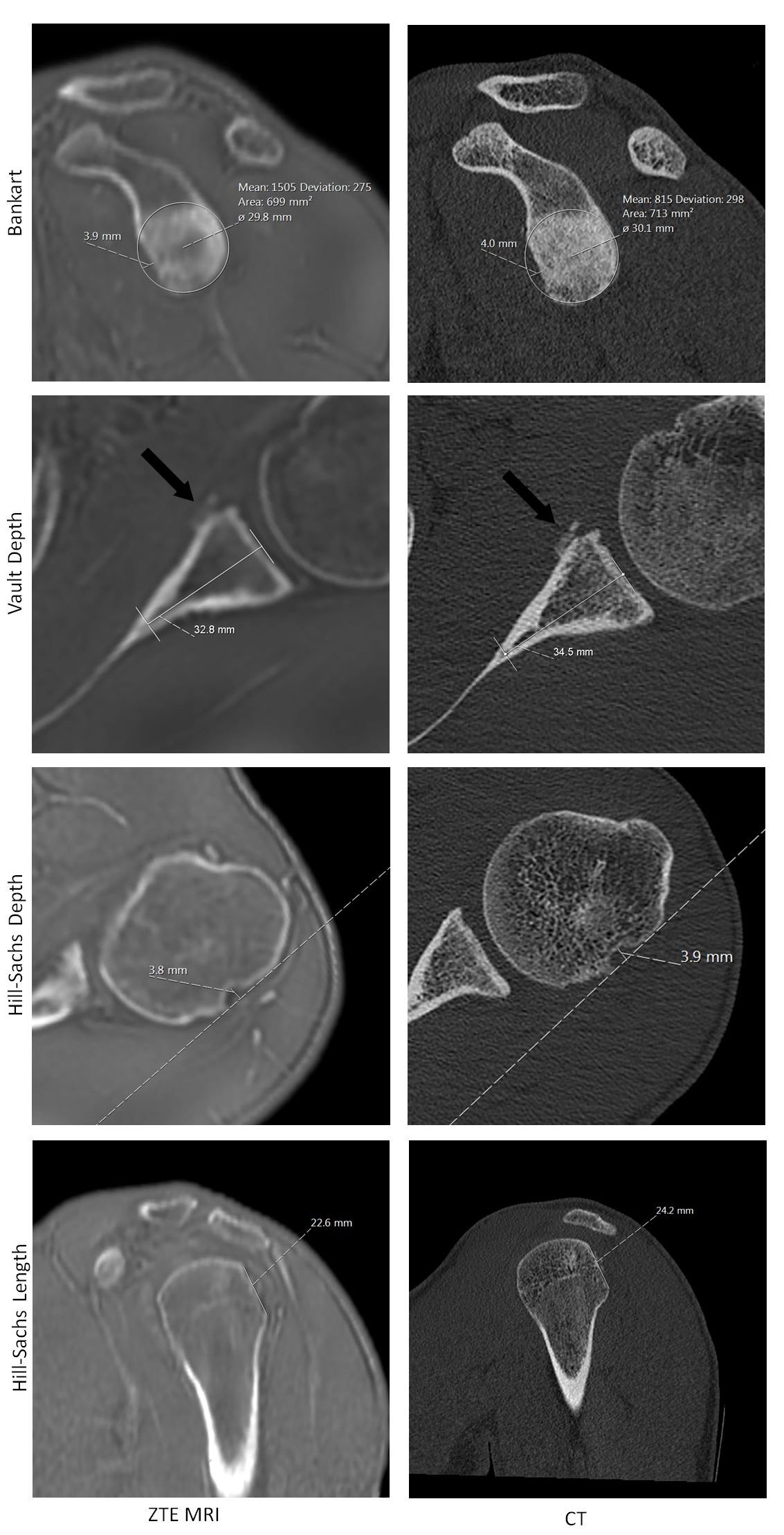
When assessing bone stock preoperatively prior to arthroplasty or following traumatic injury, accurate osseous imaging of the shoulder is necessary for clinical management. While routine MRI is commonly used to assess the soft tissue envelope, it fails to provide direct visualization of cortical bone due to the short tissue relaxation times, yielding limited signal intensity. This study investigates the utility of proton density zero echo time (ZTE) MRI for imaging cortical bone in the shoulder. With appropriate post-processing, ZTE MRI enables visualization of bone with CT-like contrast1,2 (see figure 1). ZTE imaging has been applied to the head, but has had limited application outside of the cranium.2 The objective of this study was to assess clinical utility of ZTE imaging to osseous shoulder pathologies.Methods
Under IRB approval, with informed consent, 31 patients (22M/9F, 41 ± 21 y.o.; mean±SD) were recruited consecutively and enrolled in this study. Inclusion criteria for concurrent CT consisted of a scheduled or prior shoulder CT (within 1 mo.) with no intervening surgery. CT scans were utilized as the gold standard in this study. Following an institutional standard-of-care shoulder MRI examination, the ZTE series was acquired with the following parameters: TR: 300ms, flip angle: 1°, receiver bandwidth: 62.5 kHz, matrix size: 256-320, slice thickness: 1.5 mm, scan time: ~4-6 mins, field-of-view (FOV): 20-28cm. Scans were performed on clinical 1.5T and 3T scanners (Optima MR450w and Discovery MR750, GE Healthcare, Waukesha, WI). Three-channel shoulder coils (Invivo, Gainesville, FL) and standard patient positioning were used for all imaging.
All ZTE and CT images were de-identified and randomly evaluated by a board-certified radiologist who was blinded to the other image dataset. Images were evaluated for glenoid vault depth, Bankart3 and Hill-Sachs4 lesion sizes, and the extent of any osteophytes and/or exostosis (see figure 1). Hill-Sachs lesion size was measured as length and depth of the defect relative to the intact bone surface. Bankart lesion size was determined as percent bone loss, relating the measured size of the defect and the diameter of a circle, fit to the posterior-inferior glenoid.4 When present, the extents of osseous malformations such as osteophytes and exostoses were also measured on the glenoid and humerus. Measurements were taken to the nearest millimeter. Only the portion of the cohort exhibiting each condition (on CT) was used in intermodality comparison: osseous markers for instability (Bankart and/or Hill-Sachs lesions; N = 15), and markers for osteoarthritis (ostephye/exostoses; N = 22). Glenoid vault depth was measured in 29 of the 31 patients, as artifact obscured the glenoid anatomy in 2 patients’ ZTE scans. Intermodality comparison was evaluated using intraclass correlation coefficients.
Results
Intraclass correlation coefficients (ICCs) indicate ‘good’ (ICC > 0.60) to ‘excellent’ (ICC > 0.75) inter-modality agreement between CT and ZTE for osseous measures, excluding glenoid vault depth. Specifically, Hill-Sachs depth and length agreement resulted in ICC values of 0.63 and 0.68, respectively (p = 0.006 and 0.002). Agreement in percent bone loss, as a measure of Bankart lesion size, resulted in an ICC of 0.61 and the direct measurement of the defect size yielded an ICC of 0.66 (p = 0.006 and 0.003). Glenoid vault depth exhibited ‘fair’ agreement (ICC > 0.40), with an ICC of 0.46 (p < 0.001).Discussion
Agreement was established across the five measures utilized in this study, indicating similar utility of the CT and ZTE MRI. Glenoid vault depth did not agree as strongly as other measures, likely due to the local anatomy of convergence of the interior of the scapular cortices, coupled with disparate imaging resolutions between modalities. The primary limitation of this study is that the measurements required the radiologist to locate anatomy in multi-planar reformatted (MPR) images, potentially introducing additional error in determining the best plane in which to obtain the measure.Conclusion
The ability to disclose bone detail is essential for preoperative assessment prior to arthroplasty and many of these patients also require MRI to assess the integrity of the rotator cuff and deltoid muscles and tendons. Similarly, instability patients require detection of labral, capsular and articular cartilage lesions in addition to the bone defects. ZTE MRI may obviate the need for additional CT evaluation with its attendant ionizing radiation in some cases. Further assessment in larger cohorts with complex bony deficiencies is currently underway.Acknowledgements
The authors wish to acknowledge HSS Sports Medicine & Shoulder Service for assistance with patient recruitment and HSS Radiology and Imaging staff for assistance scanning and consenting patients. HSS has an institutional research agreement in place with GE Healthcare.References
1. Delso G, Wiesinger F, Sacolick LI, et al. Clinical evaluation of zero-echo-time MR imaging for the segmentation of the skull. J Nucl Med 2015;56:417-422.
2. Wiesinger F, Sacolick LI, Menini A, et al. Zero TE MR bone imaging in the head. Magn Reson Med 2015; 75:107-114.
3. Sugaya H, Moriishi J, Dohi M, et al. Glenoid rim morphology in recurrent anterior glenohumeral instability. JBJS Am 2003; 85-A:878-84.
4. Saliken DJ, Bornes TD, Bouliane MJ, et al. Imaging methods for quantifying glenoid and Hill-Sachs bone loss in traumatic instability of the shoulder: a scoping review. BMC Musculoskelet Disord 2015; 16:164.
Figures