0833
3D Radial UTE MRI outperforms 3D Cartesian conventional echo time MRI for evaluation of cystic fibrosis lung disease1Radiology, University of Wisconsin, Madison, WI, United States, 2Translational Bioimaging, Barrow Neurological Institute, 3Medical Physics, University of Wisconsin
Synopsis
In this prospective cross-sectional study of 30 cystic fibrosis (CF) subjects, 3D radial ultrashort echo time (UTE) MRI significantly outperformed 3D Cartesian conventional echo time MRI when compared with reference standard computed tomography (CT), especially with respect to the depiction of air trapping. Short-term 1-2 week repeatability was comparable with CT. Since air trapping is considered one of the earliest signs of CF lung disease, and potentially reversible, the use of UTE MRI could significantly improve the utility of MRI as a biomarker for treatment effect in mild CF lung disease.
Introduction
Ultrashort echo time (UTE) MRI is a promising outcome measure for cystic fibrosis (CF), enabling better depiction of lung tissue than conventional echo time MRI methods. However, direct comparison using computed tomography (CT) as a reference standard has not yet been performed.Purpose
To compare the performance of 3D Radial UTE and 3D Cartesian conventional echo time MRI (with and without IV contrast) in assessing CF structural lung disease, using CT as a reference standard.Methods
In this IRB-approved, HIPAA-compliant prospective cross-sectional study, we recruited 30 subjects with CF at their baseline state of health (16:14 M:F, age: 10-55 years, FEV1: 25-122% predicted). Prior to imaging, 10 subjects were selected to undergo a second repeat study visit 1-2 weeks later.
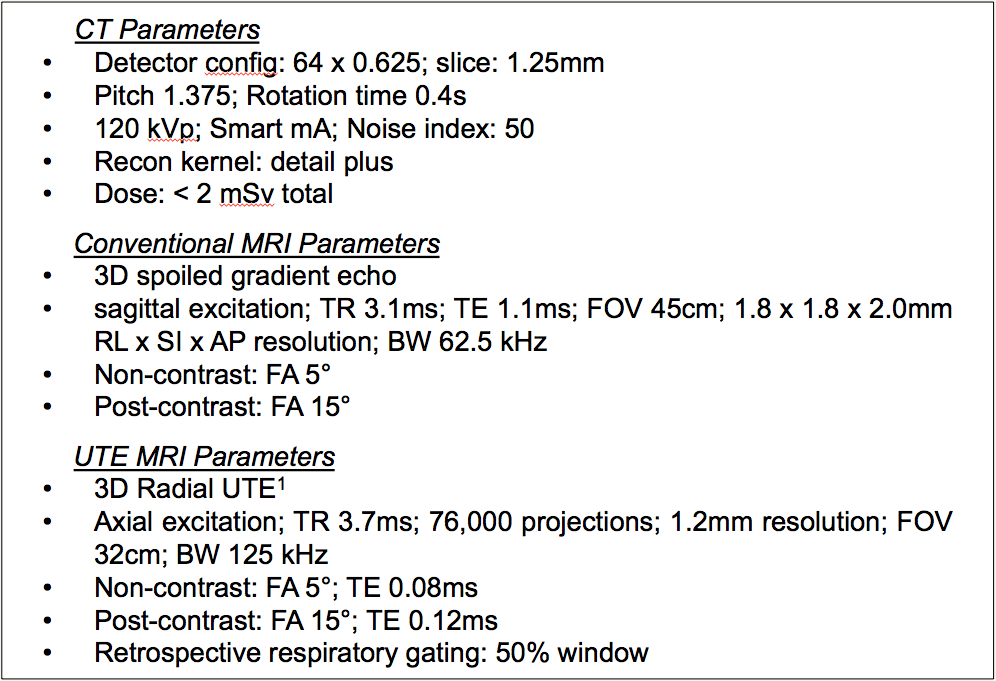
All subjects underwent CT and MRI at each study visit. Volumetric inspiratory and expiratory CT was performed on a 64-slice scanner (Lightspeed VCT, GE Healthcare). MRI was performed on a 1.5T scanner (Signa HDx, GE Healthcare), using an 8-channel cardiac coil. Both a 5-min free-breathing 3D radial UTE scan1 and a conventional 15-19s breath-hold 3D Cartesian spoiled gradient echo scan were performed. Each of these was performed twice, before and after injection of 0.1 mmol/kg gadobenate dimeglumine (MultiHance, Bracco Diagnostic). Scan parameters are listed in Figure 1.
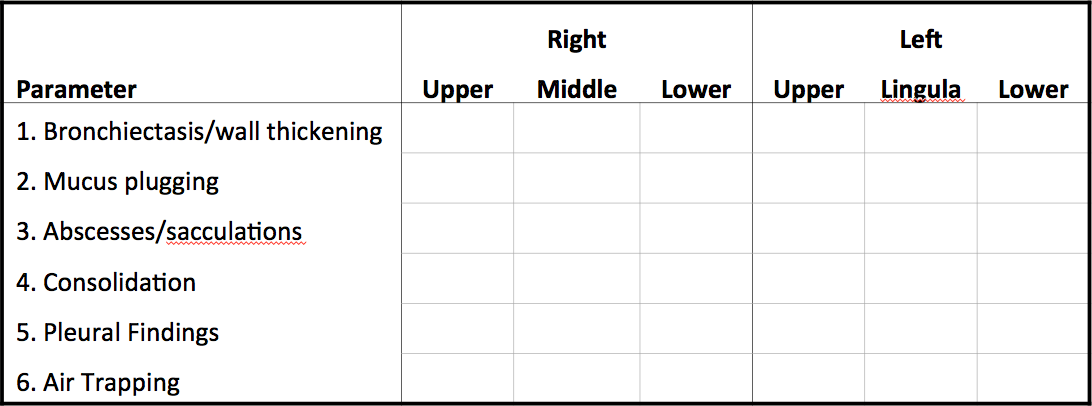
We modified the Heidelberg Structural CF score2 by adding an “air trapping” subscore and increasing the ordinal scale to 4 points (none, <1/3, 1/3-2/3, or > 2/3 of lobe affected) (Figure 2). Two cardiothoracic radiologists scored the images by consensus, blinded to the FEV1 and scores for other modalities. We block randomized each modality (non-contrast conventional, post-contrast conventional, non-contrast UTE, post-contrast UTE, and CT). Readers scored each modality in separate sessions.
We used Pearson’s correlation versus CT, Friedman’s test for differences between modalities, and Bland-Altman analysis of repeatability with p<0.05 significance threshold.
Results
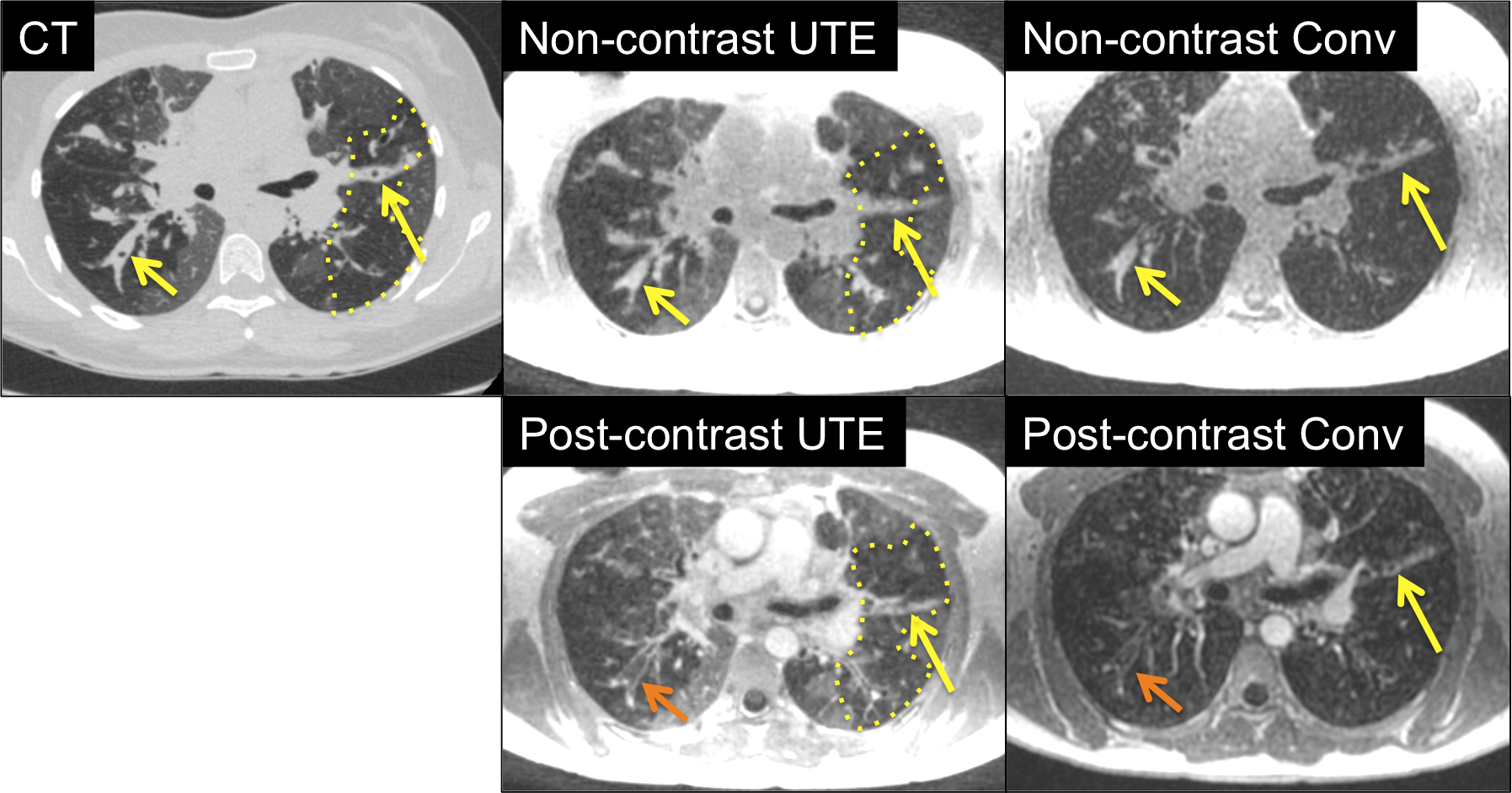
Figure 3 shows example images from one subject. Bronchiectasis and mucus plugging can be seen in all MRI modalities. Air trapping, however, can only be seen with CT and UTE MRI methods.
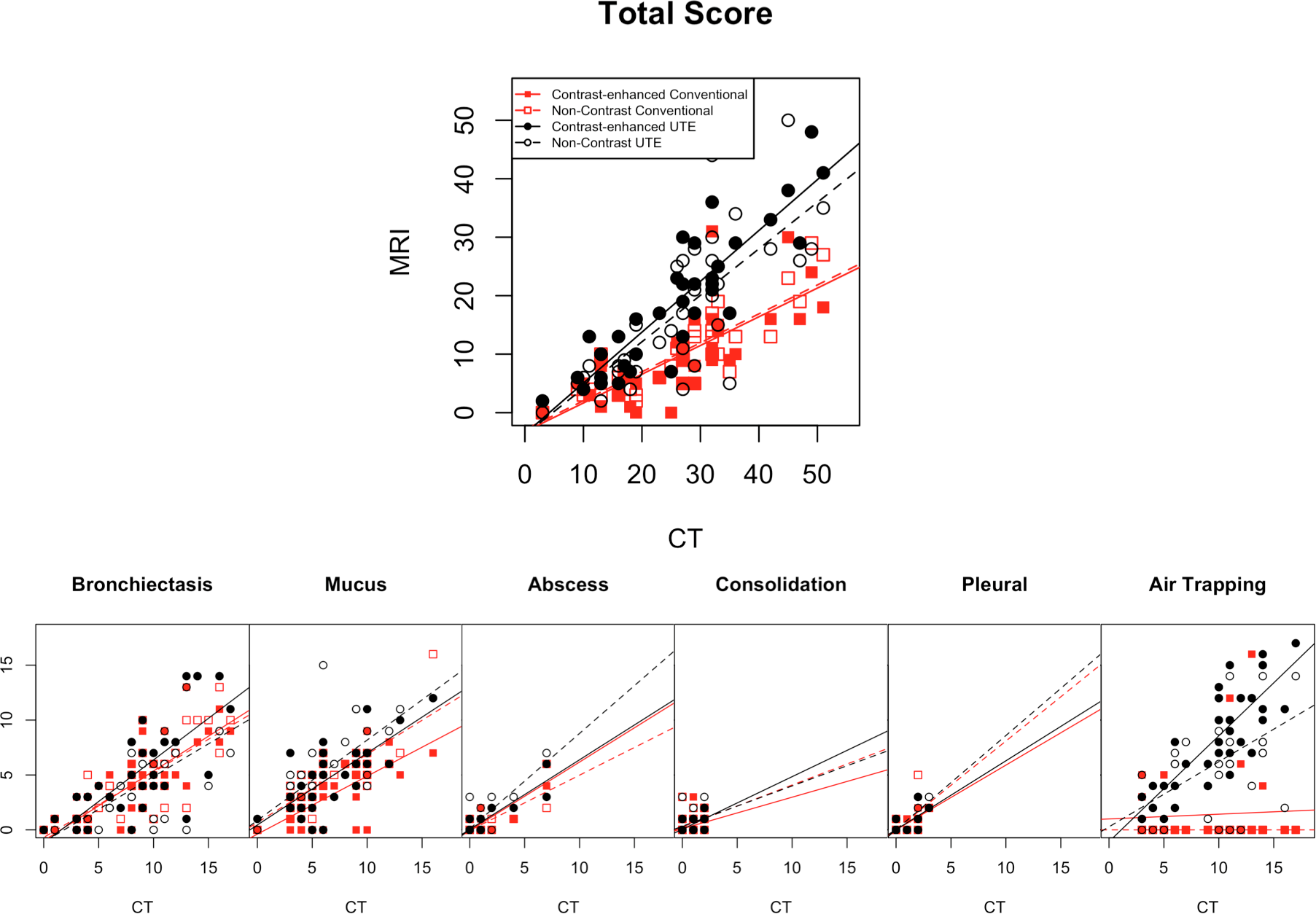
Correlation of total score with CT was very good for all MRI modalities (r=0.76-0.81, p<0.01), although the slope of the regression line for UTE (non-contrast: 0.79; contrast-enhanced: 0.87) was much closer to unity than conventional MRI (non-contrast: 0.50; contrast-enhanced: 0.49). Most of this difference arose from differences in air trapping subscore, as air trapping on conventional MRI showed no significant correlation with CT (p=0.85). All other subscores correlated with CT at p<0.01 (Figure 4).
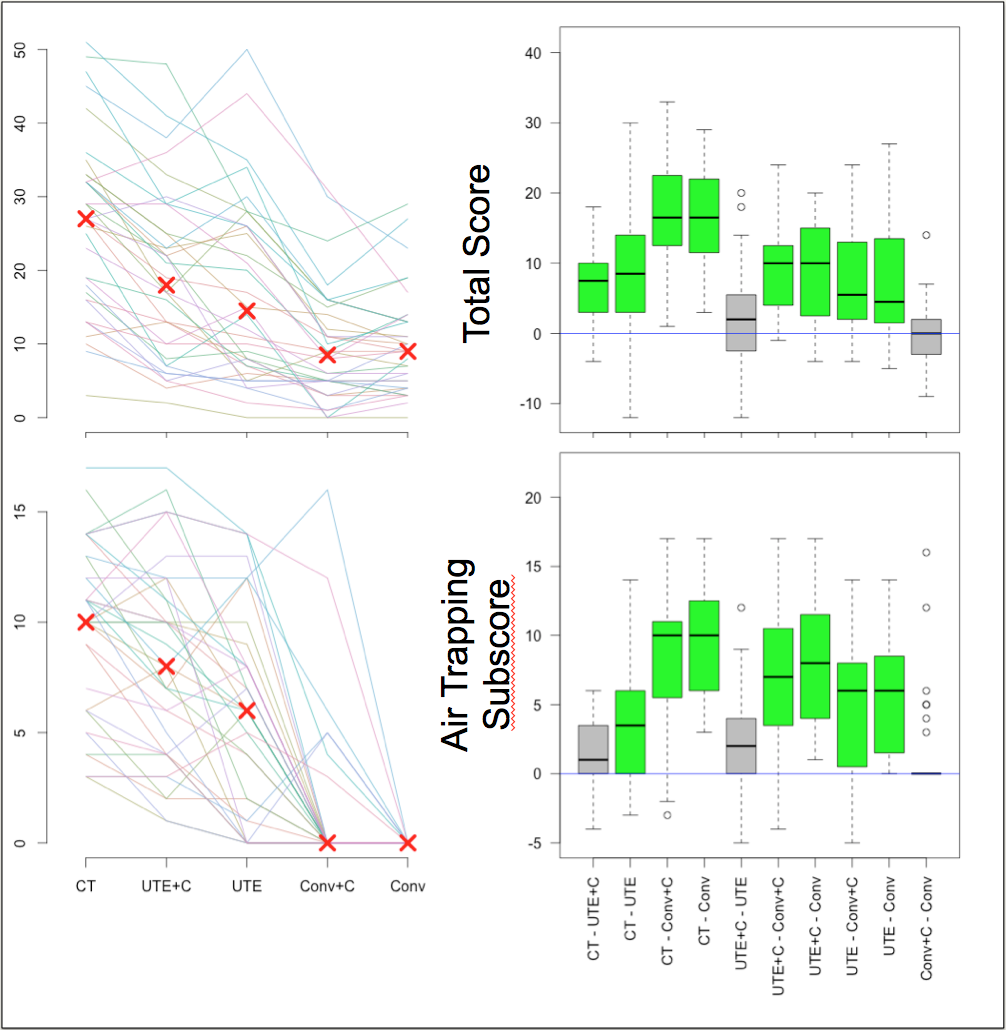
Using a repeated measures analysis, total scores from the reference standard CT were significantly higher than all MRI methods (p<0.01), and UTE scores were closer to CT than conventional MRI (p<0.01). Although contrast did affect the appearance of the images, in particular allowing differentiation of mucus from bronchial wall, it did not affect the resulting CF scores (UTE: p=0.66; Conv: p=0.98). When examining the air trapping subscore alone, UTE approached CT, and there was no difference between non-contrast and contrast-enhanced scans (Figure 5).
The short-term repeatability 95% limits of agreement did not differ significantly between modalities, potentially due to the small sample size.
Discussion
Using CT as the reference standard, 3D radial UTE MRI significantly outperformed 3D Cartesian conventional echo time MRI in the assessment of CF lung disease. Although the use of IV contrast did affect the appearance of the images, it did not significantly affect scoring. The performance of UTE MRI in the assessment of air trapping is particularly important. As air trapping is likely one of the earliest signs of CF lung disease, it is likely to be of increasing importance in assessing treatment response in young patients and those with mild disease. When combined with functional MRI methods such as ventilation or perfusion imaging, this could provide a CF biomarker superior to CT without the need for ionizing radiation.Acknowledgements
NIH UL1 TR000427 and NIH KL2 TR000428References
1. Johnson KM, Fain SB, Schiebler ML, Nagle S. Optimized 3D ultrashort echo time pulmonary MRI. Magn Reson Med 2013;70:1241–1250.
2. Eichinger M, Optazaite D-E, Kopp-Schneider A, Hintze C, Biederer J, Niemann A, Mall MA, Wielpütz MO, Kauczor H-U, Puderbach M. Morphologic and functional scoring of cystic fibrosis lung disease using MRI. Eur J Radiol 2012;81:1321–1329.
Figures