0826
Free-Breathing Pediatric Chest MRI: Utility of Self-Navigated Golden-Angle Ordered Conical Ultrashort Echo Time (UTE) Acquisition1Department of Radiology, Stanford University, Stanford, CA, United States, 2Applied Science Laboratory, GE Healthcare, San Diego, CA
Synopsis
To assess feasibility of conical k-space trajectory free-breathing UTE chest MRI versus 4D flow and effects of 50% data subsampling and soft-gated motion correction, 32 consecutive children were recruited. Images scored by two blinded radiologists showed good to excellent delineation of all evaluated structures. UTE surpassed 4D flow for lungs and airways and was equivalent for pulmonary arteries. 50% subsampling mildly reduced but maintained diagnostic image quality, favoring its shorter scan time. Soft-gating slightly improved pulmonary artery delineation for one reader but overall degraded images, possibly due to noise from data subsampling, and suggesting motion-robustness of the conical golden-ordered trajectory.
INTRODUCTION
Chest MRI is an important goal in pediatrics to avoid ionizing radiation but has been traditionally limited by inherent low lung signal and respiratory motion.1 Recently, 3D radial UTE chest MR has shown promise, but experience is limited to animal and small human studies.2-4. UTE imaging utilizing conical k-space sampling permits greater scan efficiency than do radial acquisitions, while still diffusing motion and aliasing artifacts for robustness to flow and motion and, thus, potentially yielding diagnostic free-breathing images. Here, we demonstrate a golden-angle ordered conical UTE MR technique to further diffuse motion artifacts, assess the utility of 50% data subsampling to decrease scan time, and use central k-space data phase for self-navigation and associated soft-gated motion correction. We assess its clinical performance for children undergoing ferumoxytol-enhanced 3T MRI in comparison to an established 4D SPGR-based MRA technique (4D flow).5-7METHODS
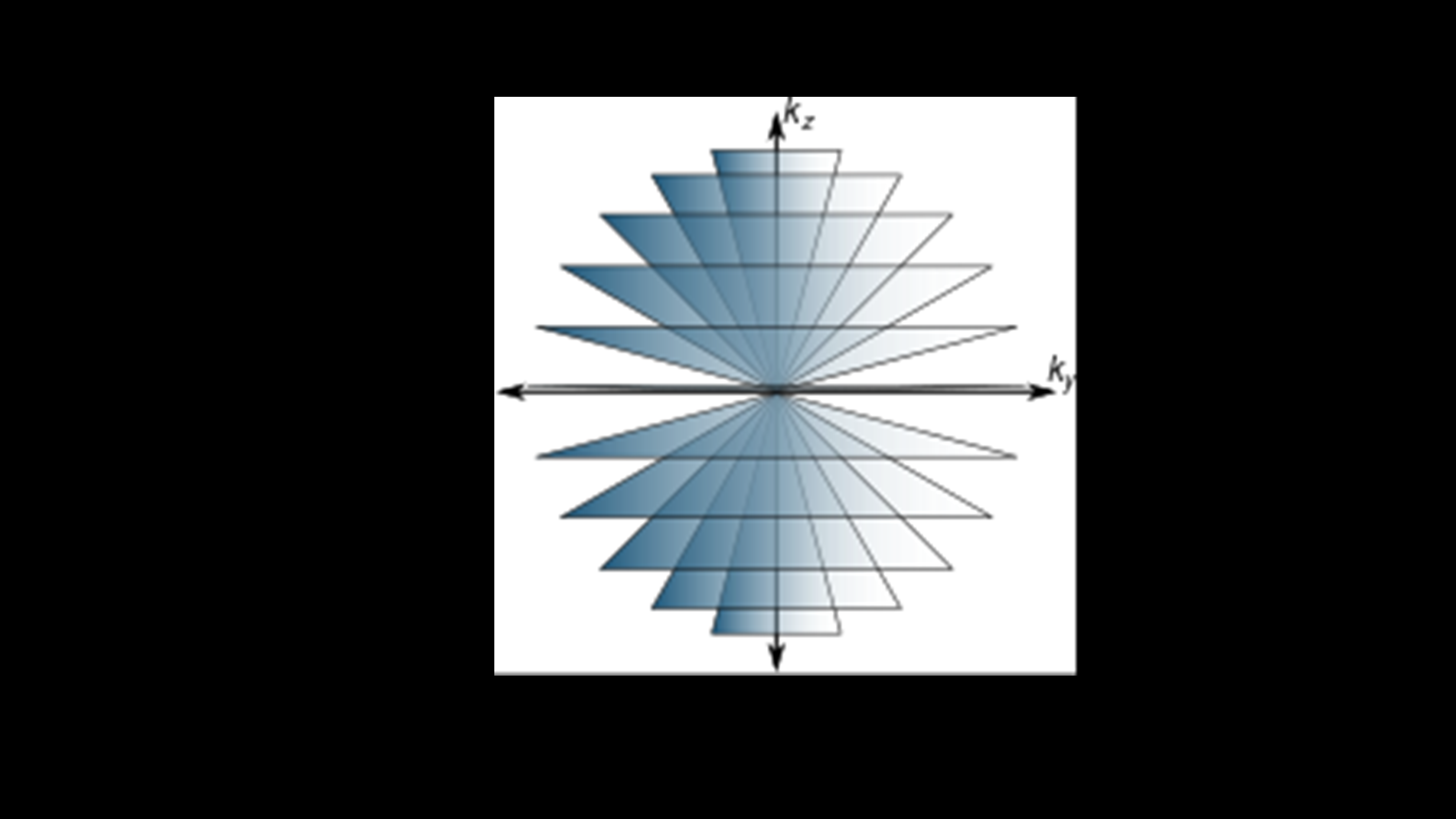
UTE data were acquired using an RF-spoiled GRE sequence with a 3D conical k-space sampling trajectory8-9 (Figure 1). The acquisition of each interleaf was ordered according to the golden-ratio permutation to increase motion robustness and to enable retrospective data subsampling. The DC signal from each conical interleaf was processed to compute motion waveforms. Images were reconstructed using either gridding, soft-gated parallel imaging and compressed sensing (PI & CS)10-11, or PI & CS with no soft-gating. All reconstructions were performed using the Berkeley Advanced Reconstruction Toolbox12. 4D flow acquisitions used minimum TE flow-encoding gradients and a 4-point encoding strategy in a cardiac synchronized 3D Cartesian RF-spoiled gradient echo sequence with pseudo-random k-space under-sampling and built-in navigators, as detailed in prior work.6 The 4D flow was cardiac resolved and corrected for respiratory-motion, providing a reference to compare motion effects.
With IRB approval, 32 consecutive children who underwent both 4D flow and UTE chest MR (mean age: 5.3 years, range: 4 days-15.7 years; 21 male) in one 3T exam were recruited. All scans were enhanced with 0.1 mL/kg ferumoxytol using a slow diluted infusion. 5 (15.6%) were performed without anesthesia, 9 (28.1%) under light anesthesia with facemask or nasal cannula, and the rest under deep anesthesia with laryngeal mask airway or endotracheal tube. From UTE k-space data, three image sets were reconstructed and reviewed: (i) one with all the data, (ii) one using 50% of the data, and (iii) a final set with soft-gating motion correction. Two blinded radiologists independently scored image quality of the lungs, pulmonary arteries (PAs), and airways on a 5-point scale (1-nondiagnostic, 3-diagnostic, 5-excellent) for each UTE reconstruction and 4D flow in random order, along with the smallest visible PA level (up to subsegmental). Scores and PA segment visibility were compared using Wilcoxon rank-sum, Wilcoxon signed-ranks, and Kruskall-Wallis tests. Interobserver agreement was assessed with the intraclass correlation coefficient (ICC).
RESULTS
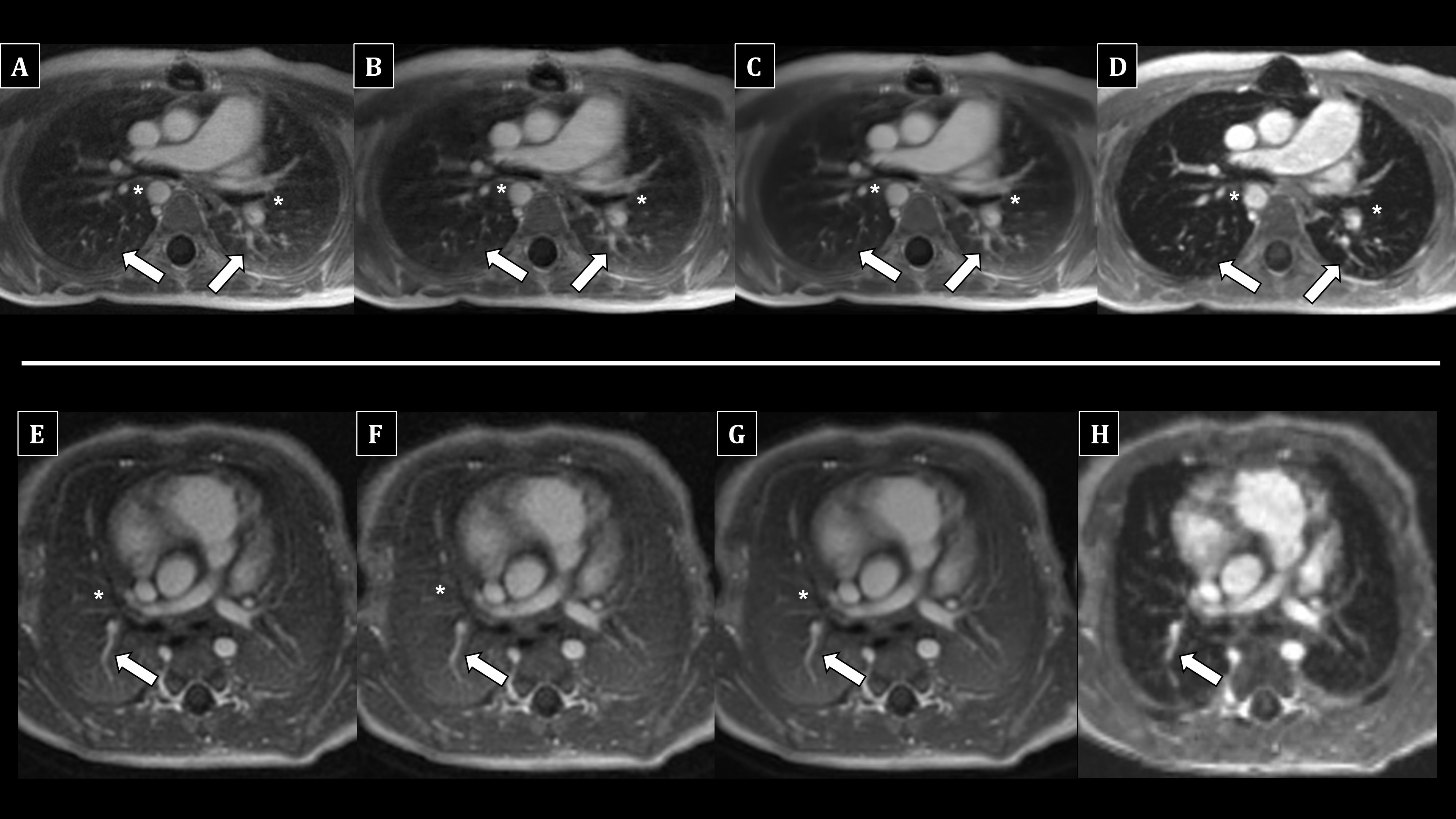
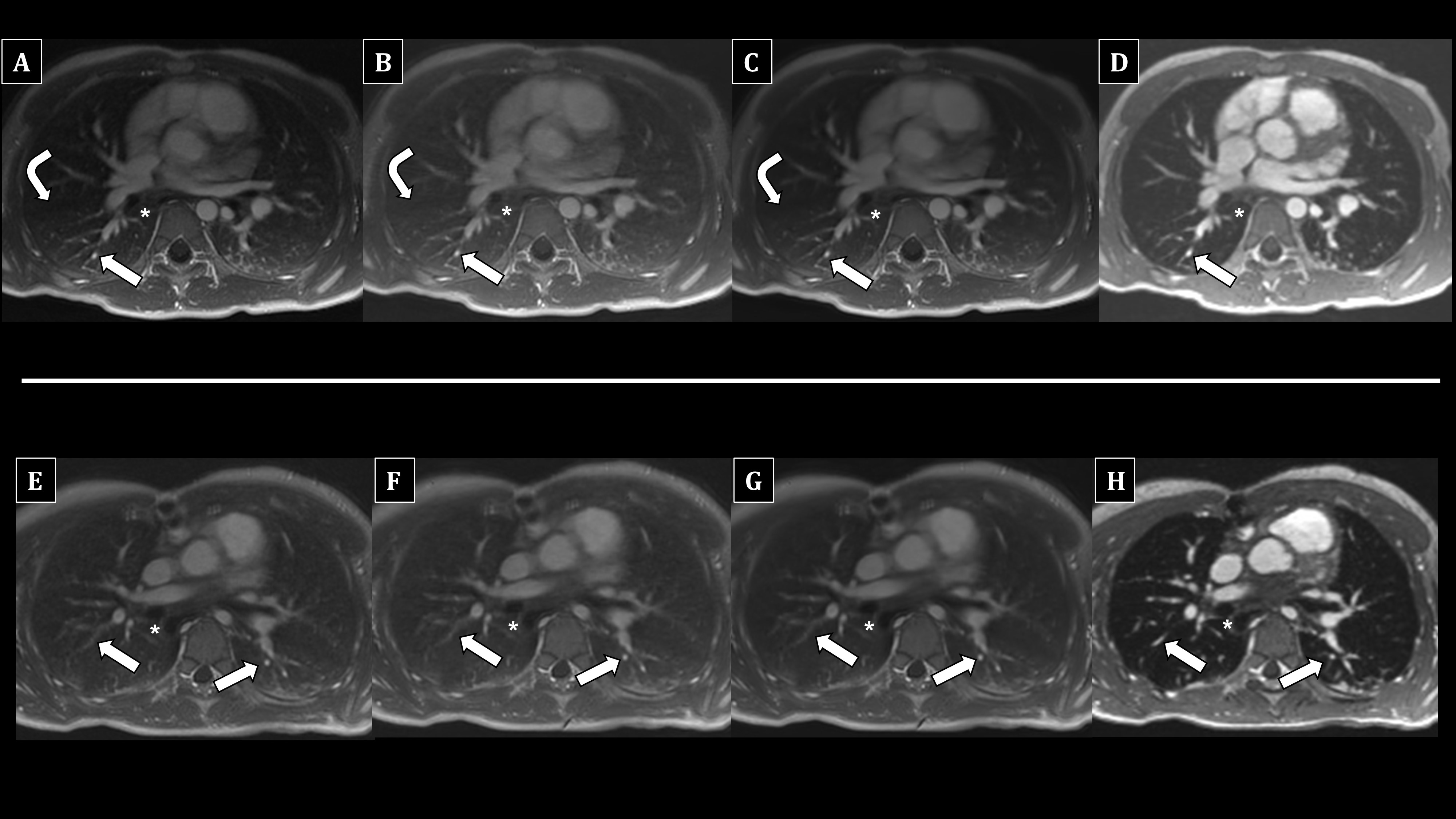
For fully sampled (raw) UTE, combined mean scores for all landmarks were >=4, indicating good to excellent image quality. Figure 2 shows a summary of scores. Raw UTE was superior to 4D flow for the lungs and airways (P<0.001 for both), with similar PA quality (P=0.62). 50% subsampling degraded quality for all landmarks (P<0.001), but the mean difference compared to raw UTE was only 0.4 for each structure. Overall, motion correction degraded lung (P<0.001) and airway (P=0.009) quality; PA quality trended down (P=0.09). However, for reader 2, it slightly improved PA quality (not statistically significant, P=0.61), without changing airway quality. PAs were visible to the subsegmental level in >93% scans for all techniques (P=0.27). Interobserver agreement was excellent for combined scores (ICC=0.83).DISCUSSION
Free-breathing conical UTE permits good or better visualization of lungs, airways, and PAs to the subsegmental level. Blurring from off-resonance in the chest did not noticeably impact UTE images. Lung and airway assessment was superior to 4D flow most likely due to greatly shorter TE, while PA delineation was similar. 50% subsampling only mildly degraded images, favoring the use of a decreased scan time (up to 150 seconds). Motion correction overall mildly degraded images, possibly due to greater noise from data subsampling or suboptimal tuning of the reconstruction parameters, and suggesting motion robustness of the conical golden-angle ordered trajectory. However, it may improve PA delineation in nonsedated patients, as evidenced by one reader’s scores. Notably, all scans were enhanced with ferumoxytol, which may further enhance SNR and overall image quality.CONCLUSION
Free-breathing conical k-space trajectory UTE chest MRI is feasible, with diagnostic image quality surpassing 4D flow for the lungs and airways and equivalent for PAs. Data subsampling will allow even shorter scan times. In select nonsedated cases, motion-correction may improve PA delineation.Acknowledgements
Research support from GE Healthcare, and support of NIH R01EB009690.
References
1. Liszewski MC, Hersman FW, Altes TA, et al. Magnetic resonance imaging of pediatric lung parenchyma, airways, vasculature, ventilation, and perfusion: state of the art. Radiol Clin North Am 2013; 51(4):555-582.
2. Bannas P, Bell LC, Johnson KM. Pulmonary embolism detection with three-dimensional ultrashort echo time MR imaging: experimental study in canines. Radiology 2016; 278(2):413-421.
3. Hahn AD, Higano NS, Walkup LL, et al. Pulmonary MRI of neonates in the intensive care unit using 3D ultrashort echo time and a small footprint MRI system. J Magn Reson Imaging 2016; [Epub ahead of print]. doi: 10.1002/jmri.25394
4. Roach DJ, Crémillieux Y, Fleck RJ, et al. Ultrashort echo-time magnetic resonance imaging Is a sensitive method for the evaluation of early cystic fibrosis lung disease. Ann Am Thorac Soc 2016; [Epub ahead of print]. doi: 10.1513/AnnalsATS.201603-203OC
5. Vasanawala SS, Hanneman K, Alley MT, Hsiao A. Congenital heart disease assessment with 4D flow MRI. J Magn Reson Imaging 2015; 42(4):870-886.
6. Cheng JY, Hanneman K, Zhang T, et al. Comprehensive motion-compensated highly accelerated 4D flow MRI with ferumoxytol enhancement for pediatric congenital heart disease. J Magn Reson Imaging 2016; 43(6):1355-1368.
7. Hanneman K, Kino A, Cheng JY, Alley MT, Vasanawala SS. Assessment of the precision and reproducibility of ventricular volume, function, and mass measurements with ferumoxytol-enhanced 4D flow MRI. J Magn Reson Imaging 2016; 44(2):383-392.
8. Carl M, Bydder GM, Du J. UTE imaging with simultaneous water and fat signal suppression using a time-efficient multispoke inversion recovery pulse sequence. Magn Reson Med 2016; 76(2):577-582.
9. Gurney PT, Hargreaves BA, Nishimura DG. Design and analysis of a practical 3D cones trajectory. Magn Reson Med 2006; 55(3):575-582.
10. Cheng JY, Zhang T, Ruangwattanapaisarn N, et al. Free-breathing pediatric MRI with nonrigid motion correction and acceleration. J Magn Reson Imaging 2015; 42(2):407-420.
11. Johnson KM, Block WF, Reeder SB, Samsonov A. Improved least squares MR image reconstruction using estimates of k-Space data consistency. Magn Reson Med 2012; 67(6):1600-1608.
12. Uecker M, Ong F, Tamir JI, et al. Berkeley Advanced Reconstruction Toolbox. In: 23rd Annual Meeting of ISMRM. Toronto, Ontario, Canada; 2015. p. 2486.
Figures