0803
Simultaneous acquisition of MR angiography and diagnostic images on contrast-enhanced view-sharing multi-arterial phases1Department of Radiology, Gifu University, Gifu, Japan, 2Department of Diagnostic Radiology, Faculty of Life Sciences, Kumamoto University, Japan, 3Department of Radiology, Faculty of Medicine, University of Miyazaki, Japan
Synopsis
While magnetic resonance angiography (MRA) is clinically used to evaluate vascular anatomy, whereas it needs independent scan leading to a decreased throughput. We generated MRA using early phase images in the contrast-enhanced multi-arterial phase images with view-sharing technique. Aortic branches and anatomical anomalies were clearly visualized on MRA without significant differences in contrast effect and conspicuity regardless of contrast material with different r1 value (gadoterate meglumine and gadobutrol).
Purpose
To prospectively evaluate the feasibility of magnetic resonance angiography (MRA) during abdominal dynamic contrast-enhanced MR imaging and to compare the contrast effect and conspicuity of aortic branches in MRA between gadobutrol and gadoterate meglumine.Materials and Methods
Institutional review board approval and written informed consent were obtained. From November 2015 and July 2016 in our hospital, 55 patients (29 men and 26 women; age range, 39–82 years; mean 64.2 ± 10.5 years) with known and suspected upper abdominal disease performed view-sharing dynamic contrast-enhanced MR imaging with five arterial phases.
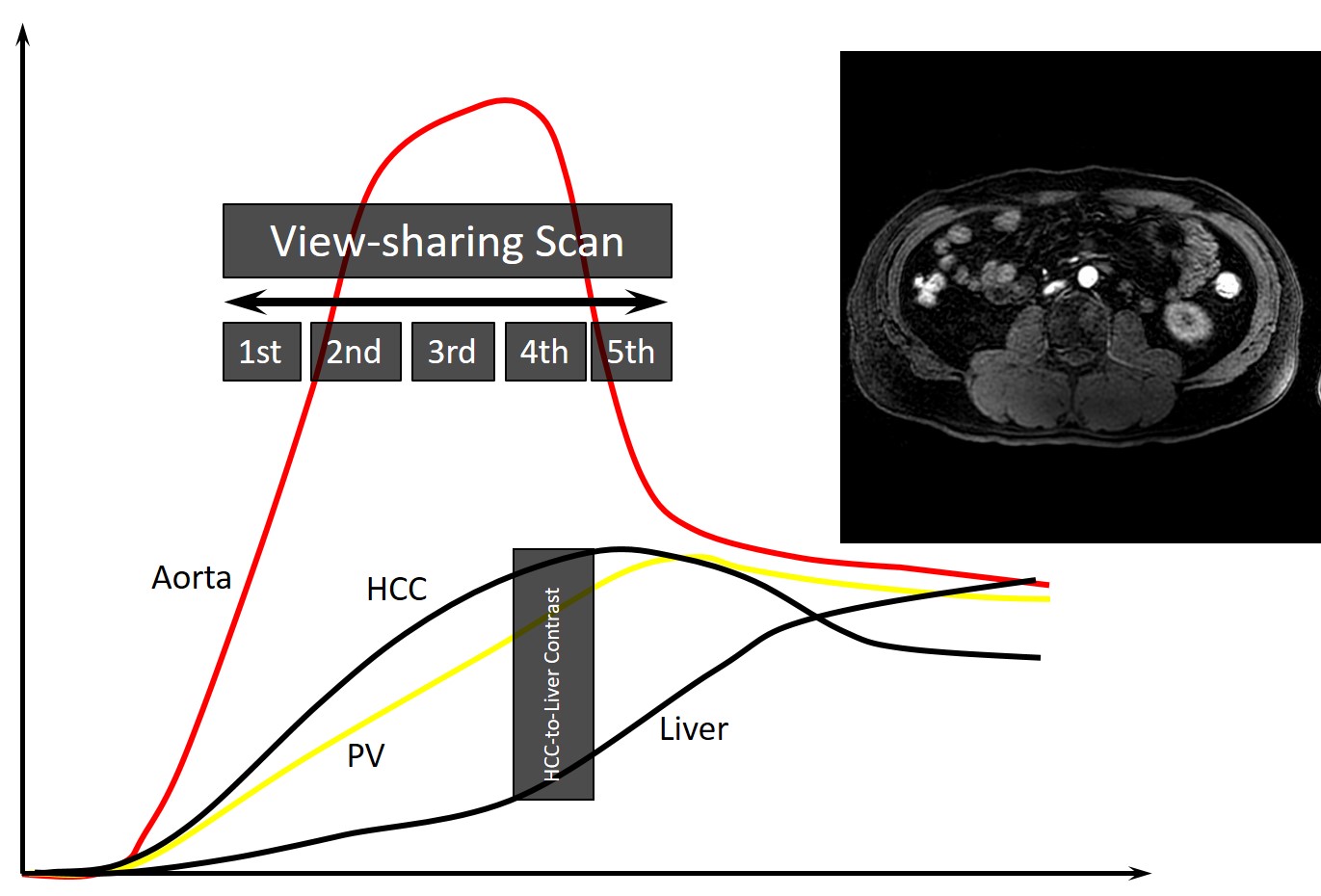
MR imaging was performed using 3-T MR system (Ingenia 3.0T CX, Philips Healthcare) and a 6-channel array coil. The contrast material was selected in random order. A dose of 0.1 mmol Gd/kg body weight (i.e. 0.1 mL/kg for gadobutrol and 0.2 mL/kg for gadoterate meglumine) was injected at a rate of 2 mL/sec followed by 30 mL saline flush at the same rate. Multi-arterial phase (5 phases) imaging was performed during a single breath hold using three-dimensional 4D-eTHRIVE sequence (view-sharing with a total of 25% in the slice and in-plane phase direction; repetition time [TR]/echo time [TE], 3.3/1.5 msec; field-of-view, 420 × 294 mm; 288 × 273 matrix (512 × 512 reconstruction); parallel imaging factor, 2; flip angle, 12˚; handwidth, 620 Hz; slice thickness, 4-mm section thickness with 2-mm overlap; acquisition time, 19-second breath holding for each phase consists of 90 slices) (Figure 1). Arterial phase scan was initiated immediately after the bolus tracking technique detected the contrast material arrival in the right ventricular.
The signal intensities of anatomical structures were measured on the first arterial phase images in the aorta, celiac artery (CA), splenic artery (SA), common hepatic artery (CHA), superior mesenteric artery (SMA), bilateral renal arteries (RAs), and paraspinal muscle. The signal intensity ratio (SIR) was calculated as a ratio of signal intensity of the artery to that of paraspinal muscle.
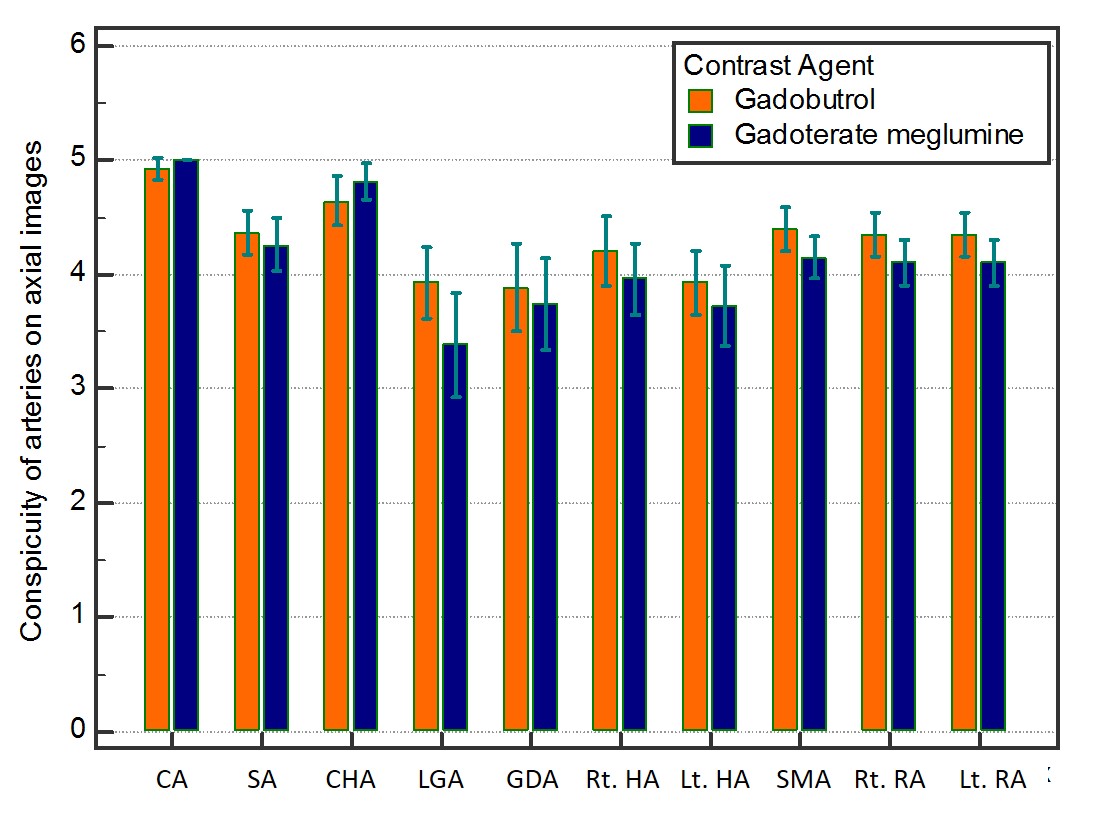
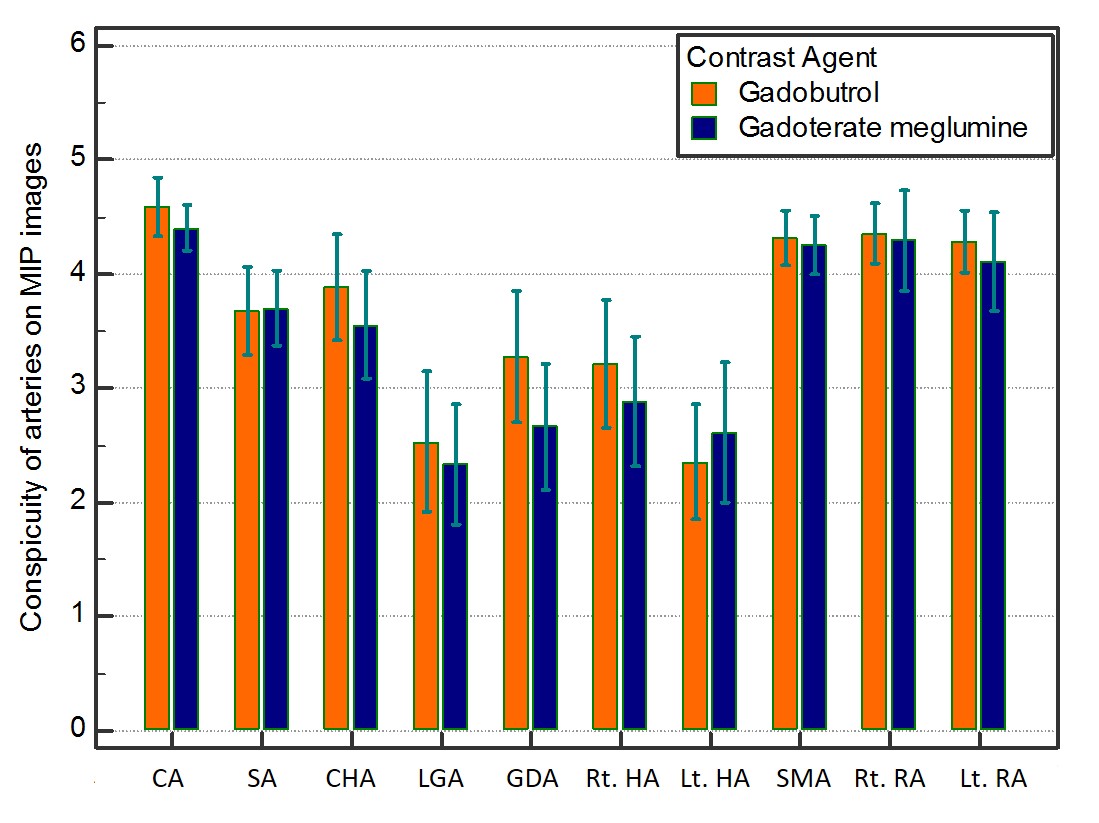
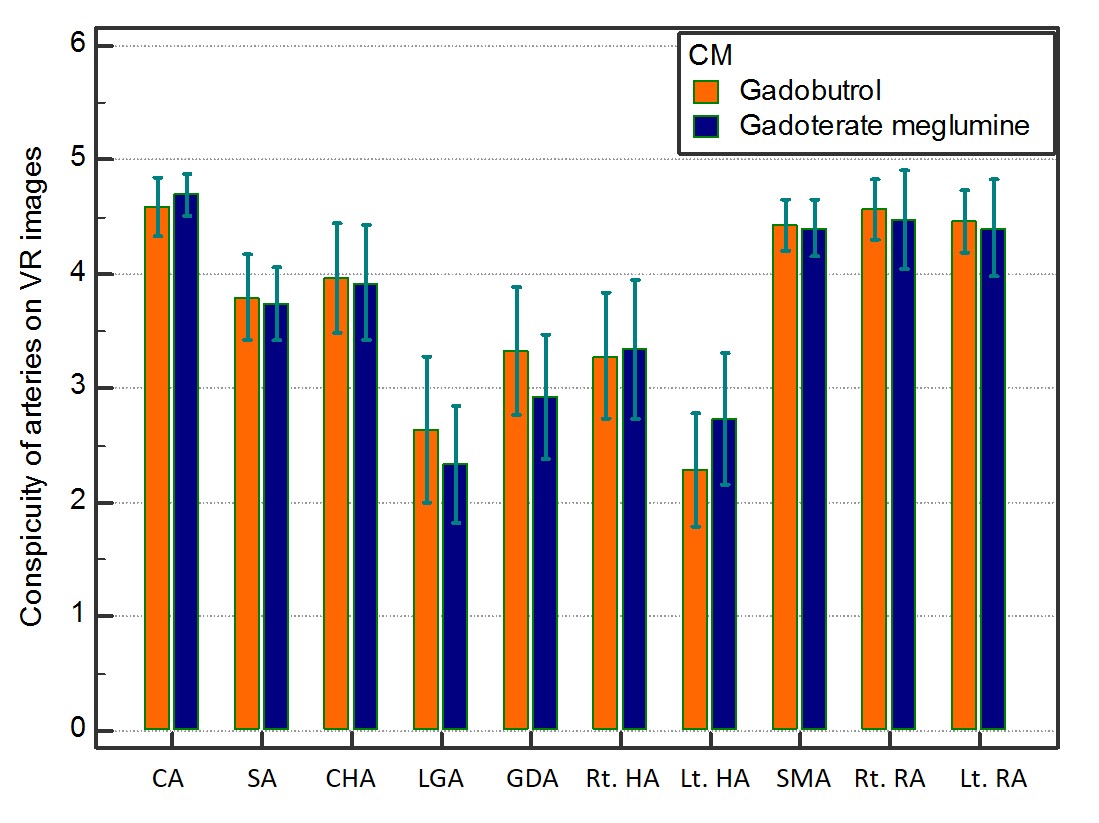
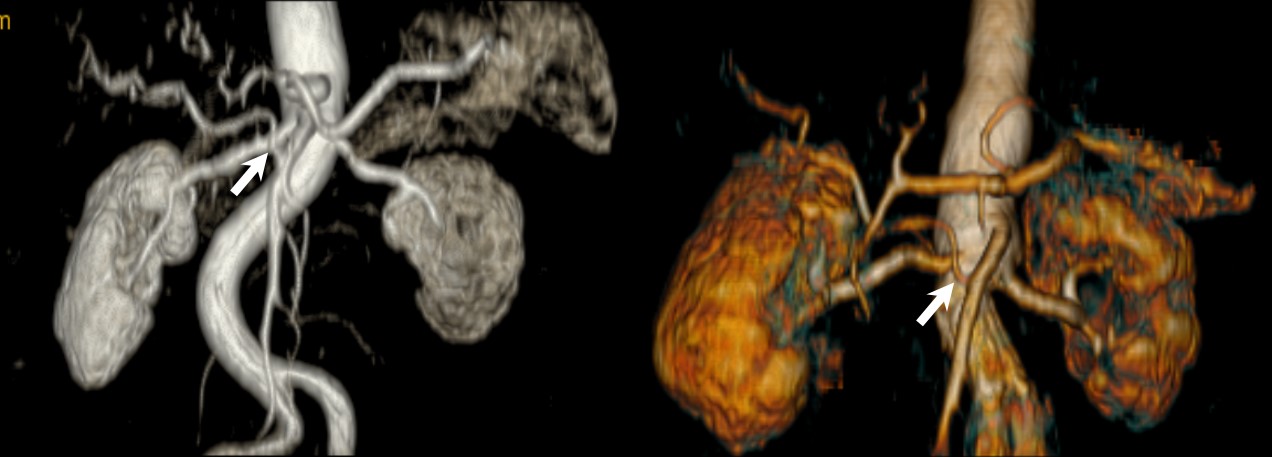
The vascular conspicuity of the CA, SA, CHA, left gastric artery (LGA), gastroduodenal artery (GDA), bilateral proper hepatic arteries (PHAs), SMA, and bilateral RAs was evaluated on the axial, maximum intensity projection (MIP), and volume-rendered images (VR) using a 5-point scale.
In the patients who had performed computed tomographic angiography (CTA) before MR angiography scan, the diameters of CA, SA, CHA, SMA, and bilateral RAs were measured and compared between on axial MRA and CTA images.
The SIRs of the CA, SA, CHA, SMA, and bilateral RAs, and qualitative ratings were compared between gadobutrol and gadoterate meglumine using the Mann-Whitney U test. The Spearman rank correlation coefficient was conducted to evaluate intermodality differences in the diameters of arteries between MRA and CTA.
Results
View-sharing multi-arterial phase imaging was successfully performed in all patients. Acceptable conspicuities were obtained in all anatomical structures (CA, SA, CHA, LGA, GDA, bilateral PHAs, SMA, and bilateral RAs) on axial, MIP, and VR images. No significant differences was found in vascular conspicuity between gadobutrol and gadoterate meglumine (P = 0.075–0.98) (Figures 2–5). The SIRs of the aorta, CA, SA, CHA, SMA, and bilateral RAs were tended to greater in gadobutrol than those in gadoterate meglumine, but there was no statistical significant difference (P = 0.053–0.17). The MRA and CTA vascular measurements were strongly correlated in all anatomical structures (r = 0.80–0.95, P < 0.0001).Discussion
In this study, we obtained an additional MRA by using view-sharing multi-arterial phase imaging without compensate for the diagnostic scan. We considered that the early and late arterial phase was suitable for MRA and organ assessment, respectively.
Our study demonstrated that the quantitative and qualitative results were comparable between gadobutrol and gadoterate meglumine. Gadolinium-based contrast agent (GBCA) magnetic properties, described by their T1 and T2 relaxivities, vary among different GBCA and depend in a complex of protein binding (1). The relaxivities of gadobutrol at 37 ℃ (r1 = 5.0, r2 = 7.1) are higher than that of gadoterate meglumine (r1 = 3.5, r2 = 4.9) (2). However, signal intensity in MR imaging in not directly proportional to the GBCA relaxivities and depend on different influencing factors. Privious study also showed no statistical significant difference in signal intensities of peripheral vascular between GBCA (3).
In conclusion, simultaneous acquisition of MRA and diagnostic images was feasible in contrast-enhanced upper abdominal MR imaging. Aortic branches and anatomical anomalies were clearly visualized on MRA without significant differences in contrast effect and conspicuity regardless of contrast material with different r1 value.
Acknowledgements
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.References
1. Saake M, Langner S, Schwenke C, et al. MRI in multiple sclerosis: an intra-individual, randomized and multicentric comparison of gadobutrol with gadoterate meglumine at 3 T. Eur Radiol. 2016;26(3):820-8.
2. Rohrer M, Bauer H, Mintorovitch J, Requardt M, Weinmann HJ. Comparison of magnetic properties of MRI contrast media solutions at different magnetic field strengths. Invest Radiol. 2005;40(11):715-24.
3. Loewe C, Arnaiz J, Krause D, et al. MR Angiography at 3 T of Peripheral Arterial Disease: A Randomized Prospective Comparison of Gadoterate Meglumine and Gadobutrol. AJR Am J Roentgenol. 2015;204(6):1311-21.
Figures