0802
Longitudinal Analysis of Vascular Inflammation and Intraluminal Thrombus Composition using High Resolution MRI in Abdominal Aortic Aneurysms1Radiology, University of California, San Francisco, San Francisco, CA, United States, 2Radiology, Changhai Hospital, Shanghai, People's Republic of China
Synopsis
Clinical management of abdominal aortic aneurysm (AAA) disease is based on the maximal diameter. Vascular inflammation and intraluminal thrombus (ILT) composition have been explored as novel imaging markers of progressive AAA disease, but studies to date have been limited by short follow-up time (~6 month). We followed 37 patients for an average of 4 years using CT/CTA and high resolution black-blood MRI. Our results show that inflammation identified by delayed ultrasmall superparamagnetic iron oxide (USPIO) particle uptake was strongly associated with AAA growth and/or intervention, whereas ILT composition was not. Imaging of vascular inflammation may improve AAA patient risk stratification.
Purpose
Abdominal aortic aneurysm (AAA) disease is common and has both high morbidity and mortality. Current management is based on the maximal AAA diameter. Studies suggest that vascular inflammation and fresh intraluminal thrombus (ILT) identified by MRI may serve as novel imaging markers of progressive AAA disease, but are limited by short follow-up (~6 month)1 2. We aim to evaluate the association between AAA growth and vascular inflammation/ILT composition over a longer follow-up duration.Methods
Study Population: 37 patients (36 male, age 72.6±7.6) with AAA disease were followed up by CTA and/or MRI. Scanning Protocols: Clinical CT/CTA has a 0.6-0.8mm in-plane and 0.625-1.25mm slice resolution. MRI was performed on a Siemens 3T scanner before and 3-5 days after ultrasmall superparamagnetic iron oxide (USPIO) administration (ferumoxytol). A previous developed 3D T1-weighted black blood MRI (DANTE-SPACE, blood suppressed fast-spin-echo 3) technique was used, and its accuracy and reproducibility has been validated against gold standard CTA 4. Scan Parameters: 1.3mm isotropic resolution, TR/TE 800ms/20ms; echo train length 60. A standard 2D T2* mapping sequence was used to quantify USPIO uptake by macrophages (i.e., inflammation). Scan parameter: 5mm slice thickness with 1.5mm in-plane resolution, 5 echoes from 4.8ms to 15ms. Image Analysis: Maximal diameters of AAA were measured by multi-planar reconstruction (MPR), and the growth rate (mm/year) was determined. Positive USPIO uptake was defined as over 55% drop of T2* values2. ILT was determined as fresh if its signal on black blood MRI was higher than 1.2 times of adjacent psoas muscles 1, and old ILT was determined when the ratio is lower than 1.2. The association between vascular inflammation/ILT composition and growth were analysed.Results
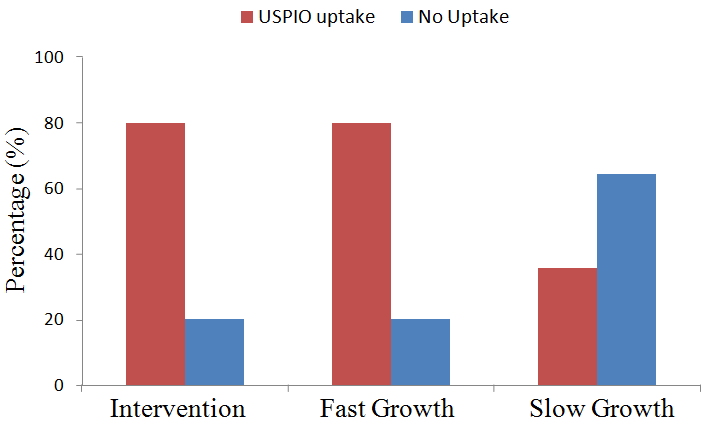
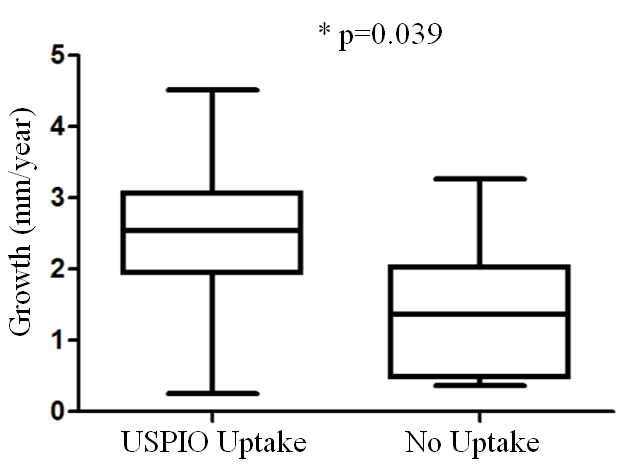
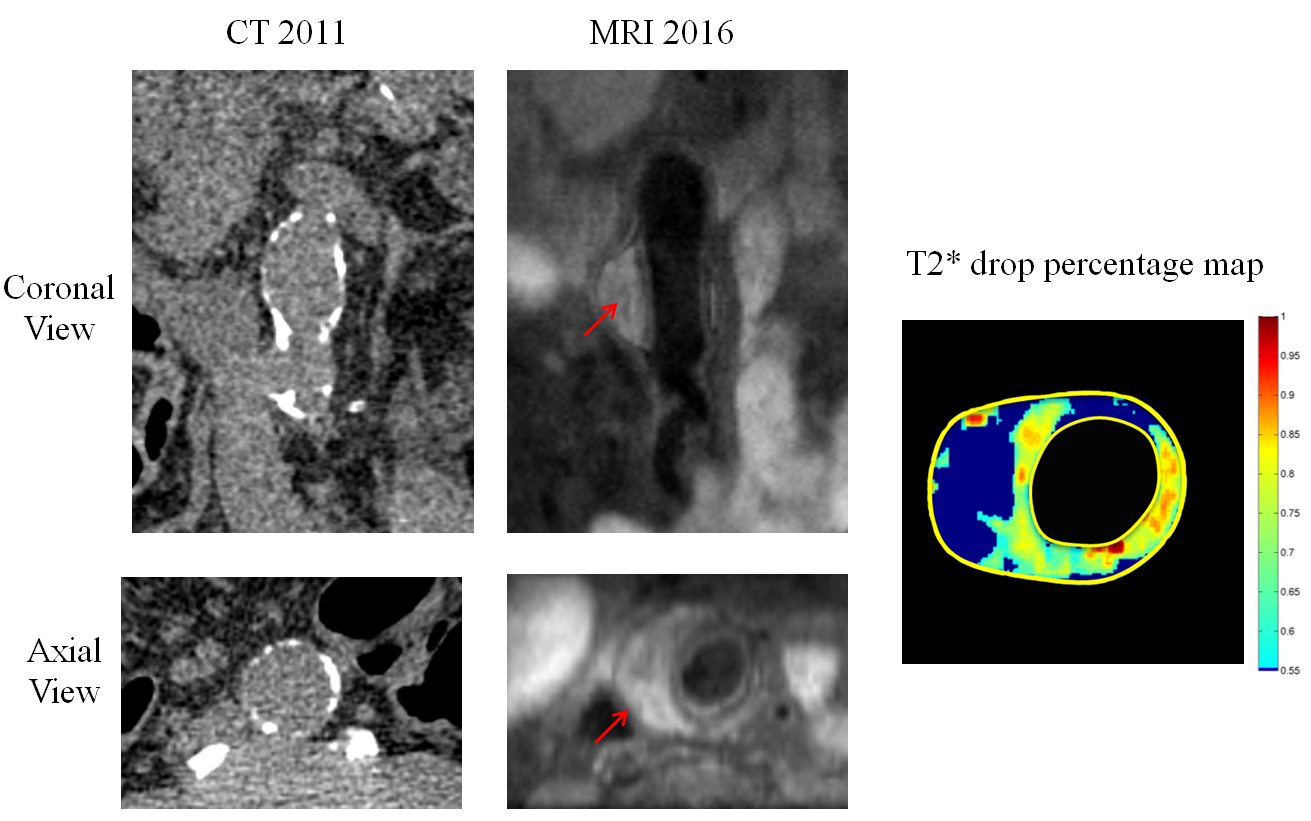
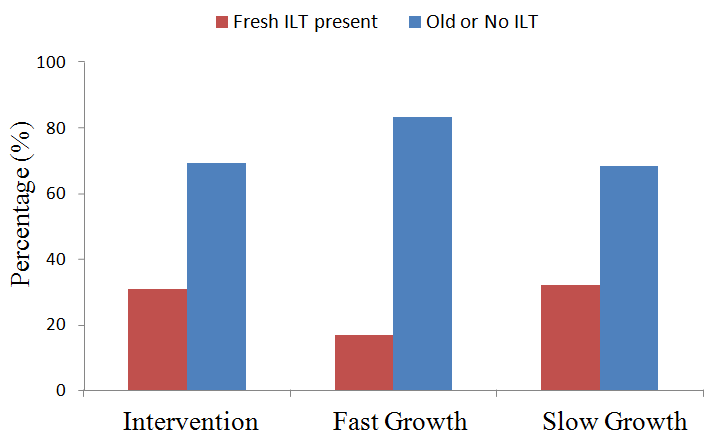
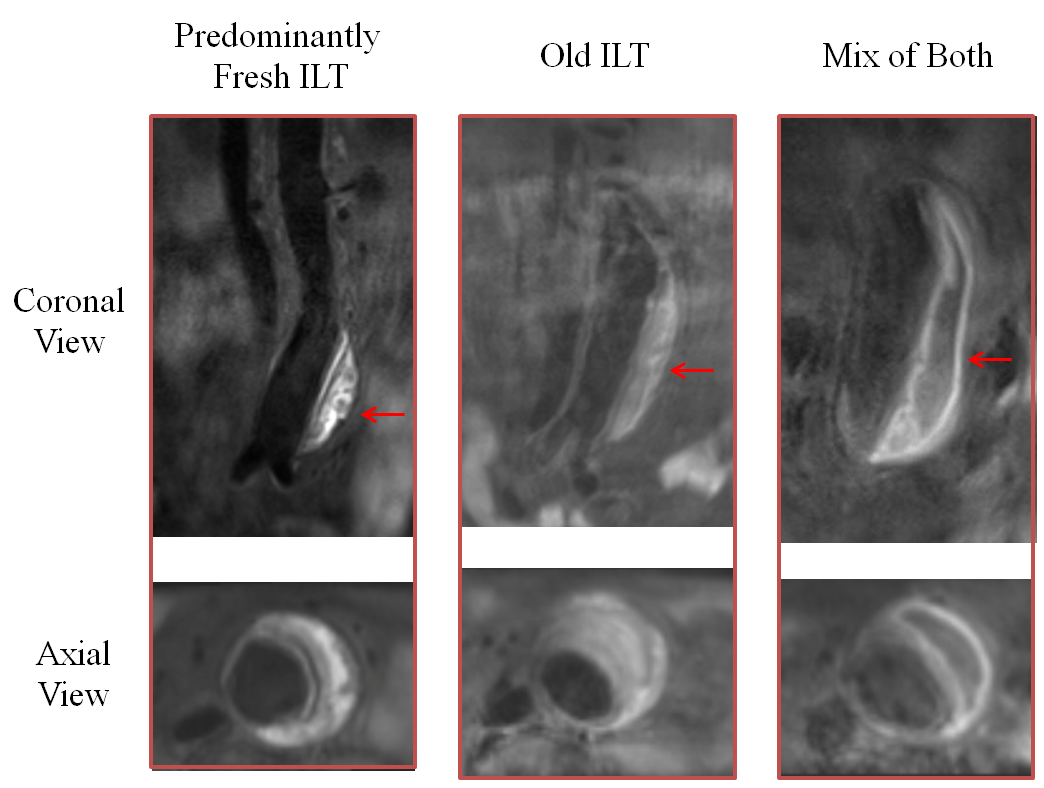
Average follow-up duration was 4.0±3.2 years (range 1.1 to 11.3). For analysis, patients were divided into 3 groups: 1) AAAs that were intervened upon (n=12); 2) fast AAA growth ≥ 3mm/year (n=6); and 3) slow AAA growth < 3mm/year (n=22). 3 patients belonged to both groups 1 and 2. 27 patients had full MRI studies with delayed USPIO imaging. The high-risk groups (groups 1 and 2) had significantly more AAAs with vascular inflammation compared with the slow growth group (8/10 and 4/5, versus 5/14, Figure 1). In 19 patients with full MRI studies, AAAs with USPIO uptake grew significantly faster than AAAs without USPIO uptake (2.5±1.2 versus 1.4±0.8mm/year, p=0.039, Figure 2), despite similar initial diameters and follow-up durations. Figure 3 shows a patient with delayed USPIO uptake and fast growth. No difference in fresh/old ILT composition was found between the groups (Figure 4). Different ILT types are shown in Figure 5.Discussion
To our knowledge, this is the first study to correlate both vascular inflammation and ILT composition with AAA growth over a long follow-up duration (average 4 years). We found that delayed USPIO uptake was associated with fast AAA growth and/or intervention. Our results regarding ILT composition differ from a previous study that showed a relationship between fresh ILT and AAA growth 1. The difference may attribute to 1) the use of maximal area change versus diameter change in our study to quantify AAA growth and 2) follow-up duration of ~6 month versus an average of 4 years in our study. Our results agree with prior work linking delayed USPIO uptake and AAA growth, and highlight that vascular inflammation is a promising marker of AAA progressive disease 2. Clinical imaging of AAA inflammation has the potential to better risk stratification of AAA disease. For example, it can be used to select high risk small AAAs (<5.5cm) for more aggressive treatment or invention, and eventually improve patient outcome.Acknowledgements
This study is supported by NIH grants R01HL114118 and R01HL123759.References
1. Nguyen VL, Leiner T, Hellenthal FA, Backes WH, Wishaupt MC, van der Geest RJ, et al. Abdominal aortic aneurysms with high thrombus signal intensity on magnetic resonance imaging are associated with high growth rate. Eur J Vasc Endovasc Surg. 2014;48:676-684
2. Richards JM, Semple SI, MacGillivray TJ, Gray C, Langrish JP, Williams M, et al. Abdominal aortic aneurysm growth predicted by uptake of ultrasmall superparamagnetic particles of iron oxide: A pilot study. Circ Cardiovasc Imaging. 2011;4:274-281
3. Zhu C, Haraldsson H, Faraji F, Owens C, Gasper W, Ahn S, et al. Isotropic 3d black blood mri of abdominal aortic aneurysm wall and intraluminal thrombus. Magn Reson Imaging. 2016;34:18-25
4. Zhu C, Tian B, Leach JR, Liu Q, Lu J, Chen L, et al. Non-contrast 3d black blood mri for abdominal aortic aneurysm surveillance: Comparison with ct angiography. Eur Radiol. 2016
Figures