0788
Prevalence of diffusely abnormal white matter in individuals with clinically isolated syndromes suggestive of multiple sclerosis1Radiology, University of British Columbia, Vancouver, BC, Canada, 2Pathology & Laboratory Medicine, University of British Columbia, Vancouver, BC, Canada, 3International Collaboration on Repair Discoveries, University of British Columbia, Vancouver, BC, Canada, 4Medicine (Neurology), University of British Columbia, Vancouver, BC, Canada, 5MS/MRI Research Group, University of British Columbia, Vancouver, BC, Canada, 6Statistics, University of British Columbia, Vancouver, BC, Canada, 7Medicine, University of Calgary, Calgary, AB, Canada
Synopsis
Diffusely abnormal white matter (DAWM) is present in individuals with clinically isolated syndromes (CIS) suggestive of multiple sclerosis (MS) at a similar frequency as seen in definite MS. CIS subjects with DAWM showed reduced brain volume and greater lesion load, both of which are known to correlate with clinical disability and progression. DAWM may have prognostic importance in CIS so examining its impact on conversion to MS, future disability and progression is warranted.
Purpose
To determine the prevalence of diffusely abnormal white matter in individuals with clinically isolated syndrome suggestive of multiple sclerosis.Background
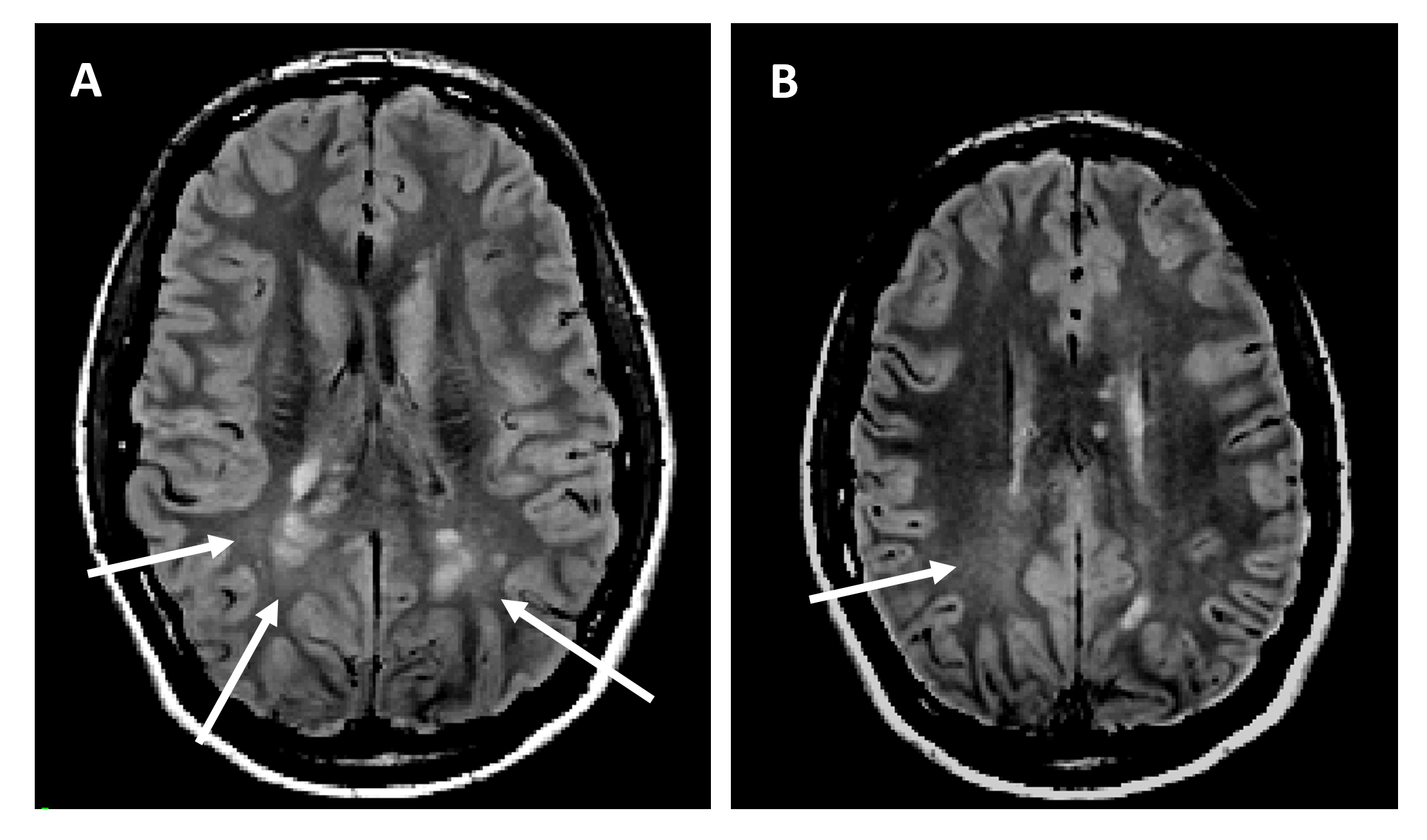
The most characteristic pathological feature of multiple sclerosis (MS) is the focal lesions in the brain. However, it is clear from the poor correlation between total lesion burden and measures of disability1, 2 that factors other than focal white matter plaques, such as non-lesional changes, contribute to clinical status and progression. “Diffusely-abnormal white matter” (DAWM) has poorly defined boundaries and a signal slightly higher than normal appearing white matter (NAWM) but not as high as a plaques on proton density (PD) and T2-weighted MRI3, 4. Up to 25% of relapsing remitting MS patients demonstrate DAWM on brain MRI3, and it is also reported in the spinal cord5. Few studies have examined DAWM in vivo, but generally MRI abnormalities, including reduced myelin water fraction6 and magnetization transfer ratio6-8, are more severe than in NAWM, but not as severe as within lesions. Post-mortem histological studies in primary and secondary progressive MS show signs of blood-brain barrier breakdown9 and reduced myelin and axons9, 10. Patients with DAWM reach the same EDSS sooner than those without DAWM and then progress faster11, 12. However, the incidence of DAWM in the very earliest stages of MS, a clinically isolated syndrome (CIS), has not been evaluated. We examined the prevalence of DAWM in individuals with CIS.Methods
Study participants: Subjects aged 18-60 years experiencing their first focal clinical demyelinating event within the previous 180 days were eligible to participate. At least two 3mm lesions on a T2-weighted screening brain MRI were required; one had to be ovoid, periventricular or infratentorial. Cerebrospinal fluid oligoclonal bands, or spinal MRI changes typical of demyelination were required for subjects over age 50 years. Key exclusions included: a better explanation for the signs and symptoms; a previous clinical event reasonably attributable to demyelination; or meeting the 2005 MacDonald criteria for MS13.
MRI Experiments: All MRI studies were performed according to a standardized protocol. Scanners (GE, Siemens, Philips) at 12 sites operating at field strengths from 1.5-3.0T were used. 180mm of contiguous head coverage in the axial plane with 3mm thick slices were obtained from the foramen magnum to just above the vertex using PD (TR/TE=2000–3400/8-20ms), T2-weighted fast spin echo (TR/TE=2800–8000/78-116ms), post-Gad T1 together with 1mm isotropic 3DT1 IR-prepped gradient echo (TR/TE/TI=5-13/2-4/450-800ms).
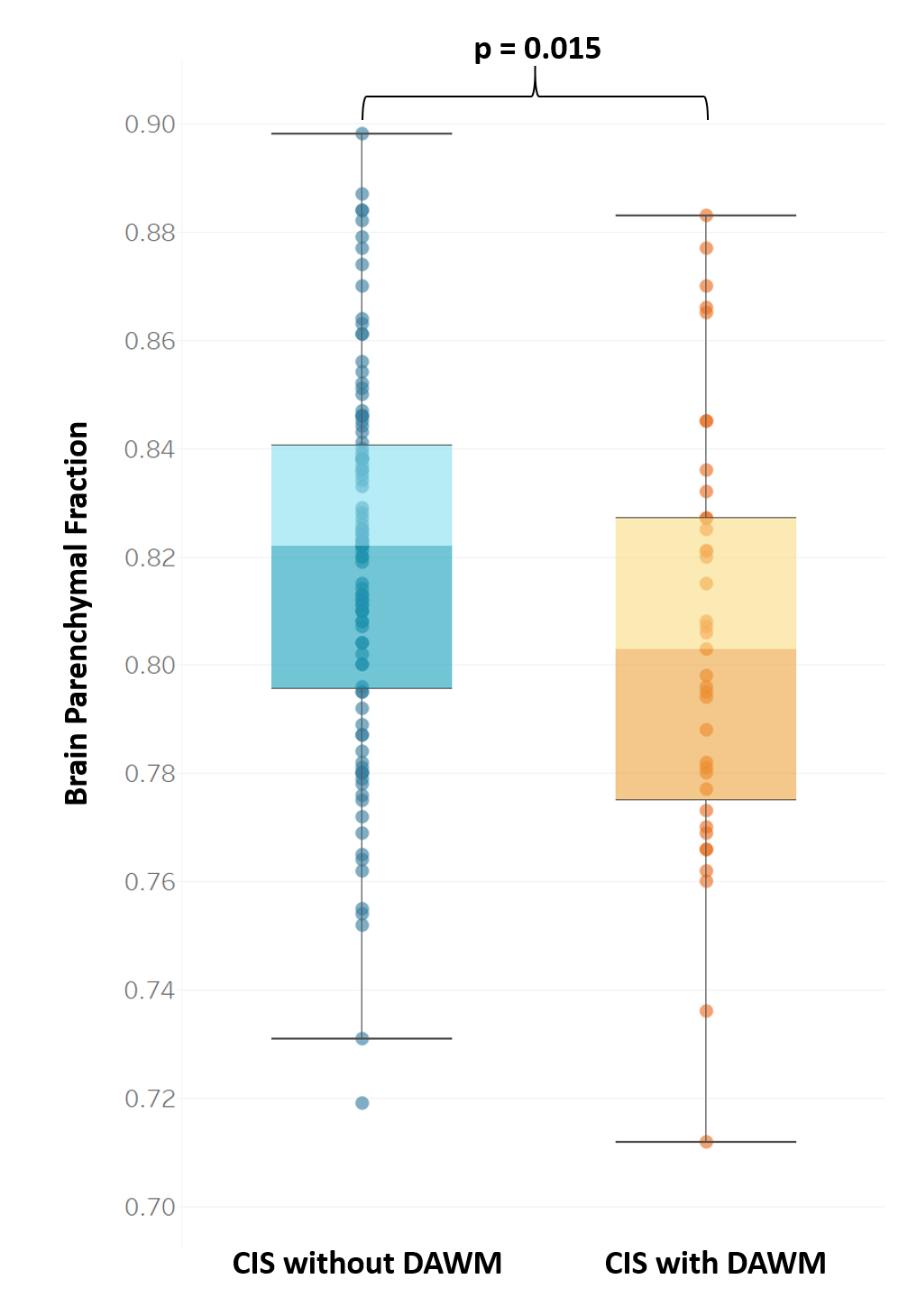
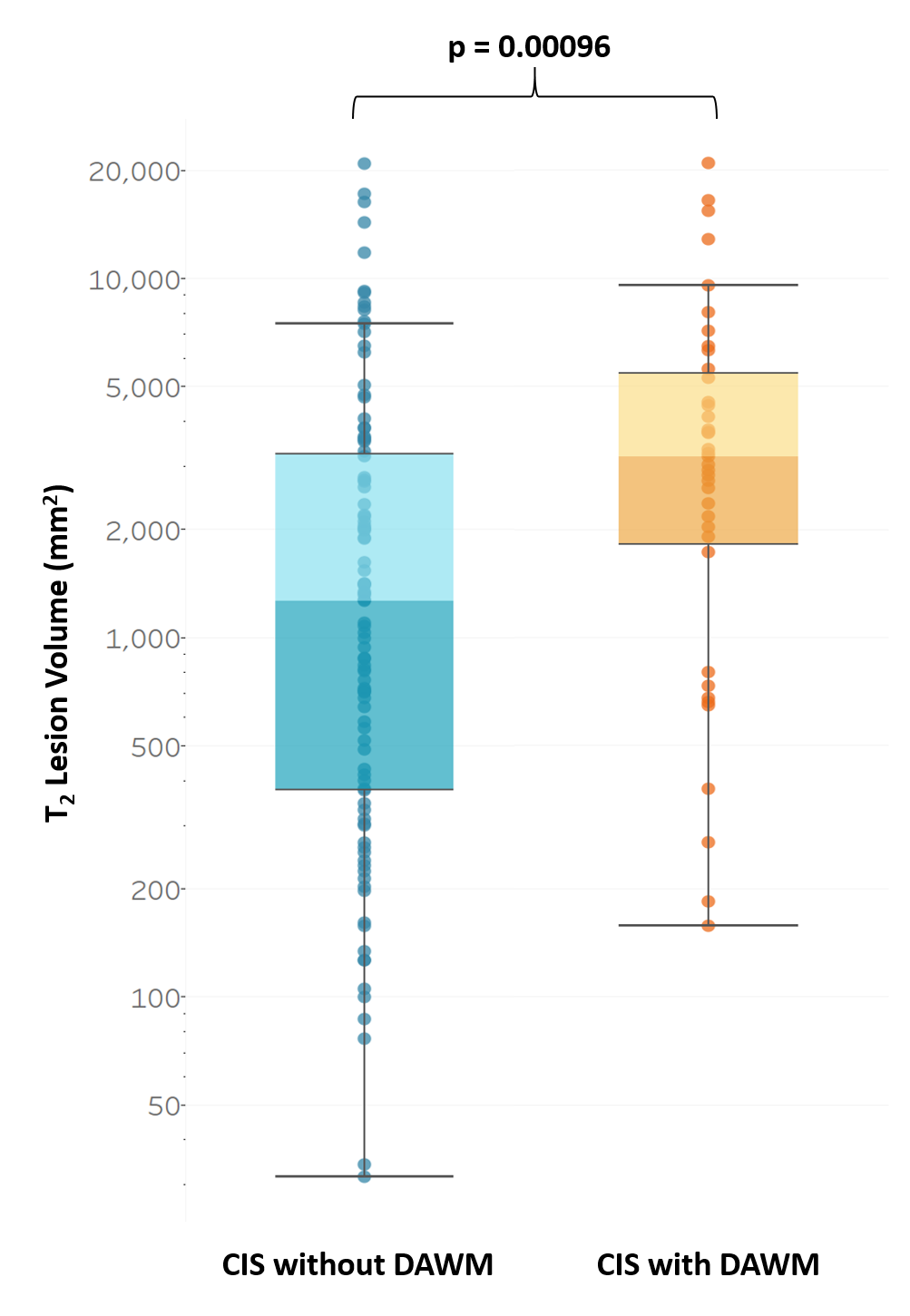
Data Analysis: T2-weighted scans were registered to PD images14 and reviewed by 2 experienced radiologists working independently. DAWM was defined as a region of white matter that was iso-intense to gray matter on PD images, present on at least 2 consecutive slices, and at least 10 mm in diameter. DAWM was electronically labeled using in-house analysis software. After both observers completed the entire analysis, a third experienced radiologist served as an arbitrator on those visits where either observer identified DAWM. The final arbitrated results are reported. In addition, T2 lesion volume (T2LV, excluding DAWM hyperintensities) and brain parenchymal fraction (BPF) were determined15. Sex, ethnicity and the presence of gadolinium lesions in CIS with and without DAWM were examined using a chi-square test for independence. Age, T2LV and BPF were compared between participants with and without DAWM using a Mann Whitney U-Test.
Results
142 subjects with CIS were evaluated (45 male, 97 female; mean age: 36.1 years, range: 18.2-56.9 years). DAWM was present in 39 subjects (27.5%). There was no difference in sex, ethnicity or the presence of gadolinium lesions in people with and without DAWM. Figure 1 shows DAWM from 2 subjects. Subjects with DAWM had significantly lower BPF [mean (standard error) with DAWM: 0.801 (0.007), without DAWM: [0.819 (0.003), p=0.015, Figure 2] and significantly higher lesion load [with DAWM: 4542 (759)mm2, without DAWM: 2681 (381)mm2, p=0.00096, Figure 3].Conclusions
Although its exact role in the pathogenesis of MS is not known, the presence of DAWM in 27.5% of individuals with CIS is similar to its frequency in those with definite MS. CIS subjects with DAWM also showed reduced brain volume and greater lesion load, both of which are known to correlate with clinical disability and progression. DAWM may have prognostic importance in CIS so examining its impact on conversion to MS, future disability and progression is warranted.Acknowledgements
We thank the MS study volunteers and MRI technologists at the participating sites. Funding support was provided by the MS Society of Canada.References
[1] The IFNB Multiple Sclerosis Study Group and The University of British Columbia MS/MRI Analysis Group., Interferon beta-1b in the treatment of multiple sclerosis: final outcome of the randomized controlled trial. . Neurology, 1995. 45(7): p. 1277-85.
[2] Li, D.K., et al., MRI T2 lesion burden in multiple sclerosis: a plateauing relationship with clinical disability. Neurology, 2006. 66(9): p. 1384-9.
[3] Zhao, G.J., et al., MRI dirty-appearing white matter in MS. Neurology, 2000. 54 (suppl 3): p. A121.
[4] West, J., et al., Normal appearing and diffusely abnormal white matter in patients with multiple sclerosis assessed with quantitative MR. PLoS ONE, 2014. 9(4): p. e95161.
[5] Lycklama a Nijeholt, G.J., et al., MR of the spinal cord in multiple sclerosis: relation to clinical subtype and disability. AJNR: American Journal of Neuroradiology, 1997. 18(6): p. 1041-8.
[6] Laule, C., et al., Pathological basis of diffusely abnormal white matter: insights from magnetic resonance imaging and histology. Mult Scler, 2011. 17(2): p. 144-50.
[7] Ropele, S., et al., A comparison of magnetization transfer ratio, magnetization transfer rate, and the native relaxation time of water protons related to relapsing-remitting multiple sclerosis. AJNR Am J Neuroradiol., 2000. 21(10): p. 1885-91.
[8] Ge, Y., et al., Dirty-appearing white matter in multiple sclerosis: volumetric MR imaging and magnetization transfer ratio histogram analysis. AJNR Am J Neuroradiol., 2003. 24(10): p. 1935-40.
[9] Vos, C.M., et al., Blood-brain barrier alterations in both focal and diffuse abnormalities on postmortem MRI in multiple sclerosis. Neurobiol Dis, 2005. 20(3): p. 953-60.
[10] Seewann, A., et al., Diffusely abnormal white matter in chronic multiple sclerosis: imaging and histopathologic analysis. Arch Neurol, 2009. 66(5): p. 601-9.
[11] Zhao, G., et al., Possible prognostic significance of dirty-appearing white matter on MRI in multiple sclerosis. Multiple Sclerosis, 2003. 9(Suppl 1): p. S61.
[12] Lycklama-a-Nijeholt, G.J., et al., Brain and spinal cord abnormalities in multiple sclerosis. Correlation between MRI parameters, clinical subtypes and symptoms. Brain, 1998. 121 ( Pt 4): p. 687-97.
[13] Polman, C.H., et al., Diagnostic criteria for multiple sclerosis: 2005 revisions to the "McDonald Criteria". Ann Neurol, 2005. 58(6): p. 840-6.
[14] Maes, F., et al., Multimodality image registration by maximization of mutual information. IEEE Trans Med Imaging, 1997. 16(2): p. 187-98.
[15] Jones, C., et al. Atrophy Measurements in Multiple Sclerosis. in International Society for Magnetic Resonance in Medicine. 2001. Glasgow, Scotland.
Figures