0776
Motion-compensated reconstruction of fetal cardiac MRI using a golden-angle radial acquisition, retrospective gating, and compressed sensing1Medical Biophysics, University of Toronto, Toronto, ON, Canada, 2Physiology and Experimental Medicine, Hospital for Sick Children, Toronto, ON, Canada, 3Pediatric Cardiology, Hospital for Sick Children, ON, Canada, 4Pediatric and Diagnostic Imaging, University of Toronto, Toronto, ON, Canada
Synopsis
Fetal cardiac MRI requires high spatial and temporal resolution but is often limited by stochastic and periodic motion. To compensate for these sources of artifact, a radial golden-angle acquisition was used to acquire and reconstruct real-time fetal cardiac images. In-plane motion and fetal heart rate were then calculated from the real-time images and used to reconstruct reordered CINE images at high spatial and temporal resolution. Using this approach, motion-robust imaging of the fetal heart was successful in seven pregnant volunteers for both short-axis and long-axis multi-slice acquisitions.
Introduction
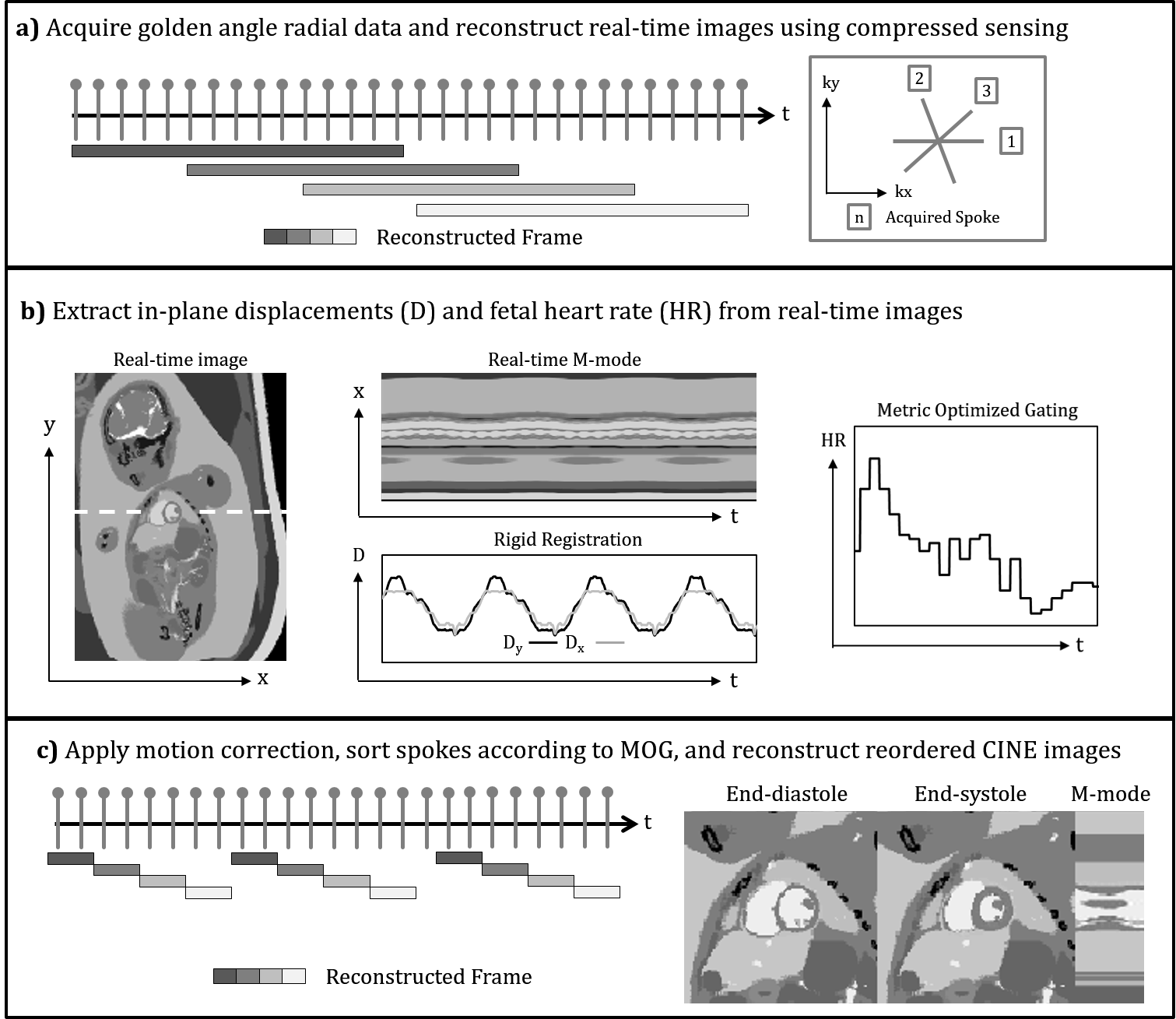
Time-resolved MRI of the fetal heart is challenging due to the size of fetal cardiac structures (vessel size: 5-10 mm), the relatively fast fetal heart rate (110-180 bpm), and both stochastic (gross fetal movement) and periodic (maternal respiration) sources of motion. Building on our previously published methods for accelerated fetal cardiac imaging with retrospective gating (1,2), in this work, we develop and evaluate a novel framework for reconstructing high spatial and high temporal resolution images of the fetal heart in the presence of motion. Fetal data are acquired using a continuous golden angle radial trajectory (Fig. 1a) and real-time images are reconstructed using compressed sensing. These real-time images enable assessment and correction of both stochastic and periodic motion (Fig. 1b) by retrospectively rejecting data undergoing through-plane motion, correcting data corrupted by in-plane motion using rigid registration of the real-time images (3–5), and extracting cardiac gating signals using metric optimized gating applied to the real-time images (2,6). The corrected data are sorted by cardiac phase and reconstructed, again using compressed sensing, to produce motion-robust reordered CINE images of the fetal heart (Fig. 1c).Methods
A steady state free precession sequence with continuous golden angle radial sampling was applied to seven human fetuses (normal fetal cardiac anatomy = 3, congenital heart disease = 4, gestational age 34-38 weeks). Slices were prescribed in both short-axis and long-axis views on a Siemens 1.5T clinical system using both body and spine matrices with approximately thirty active channels (Avanto Fit, Siemens Healthcare – Germany). For each view, 10-15 slices were prescribed spanning the heart, resulting in 127 slices of cardiac anatomy across all volunteers. Scans were performed free-breathing with the following acquisition parameters: flip angle: 70°, acquired spokes: 3000, TR: 4.95 ms, samples per spoke: 256, field-of-view: 256 x 256 mm2, spatial resolution: 1 x 1 x 4 mm3, and scan length: ~15 s per slice. Compressed sensing was used for both real-time and reordered CINE reconstructions using spatial total-variation, temporal total-variation, and temporal Fourier transforms for regularization (1). Quantitative comparison of images with and without motion correction was performed using the image error as described previously (7).Results
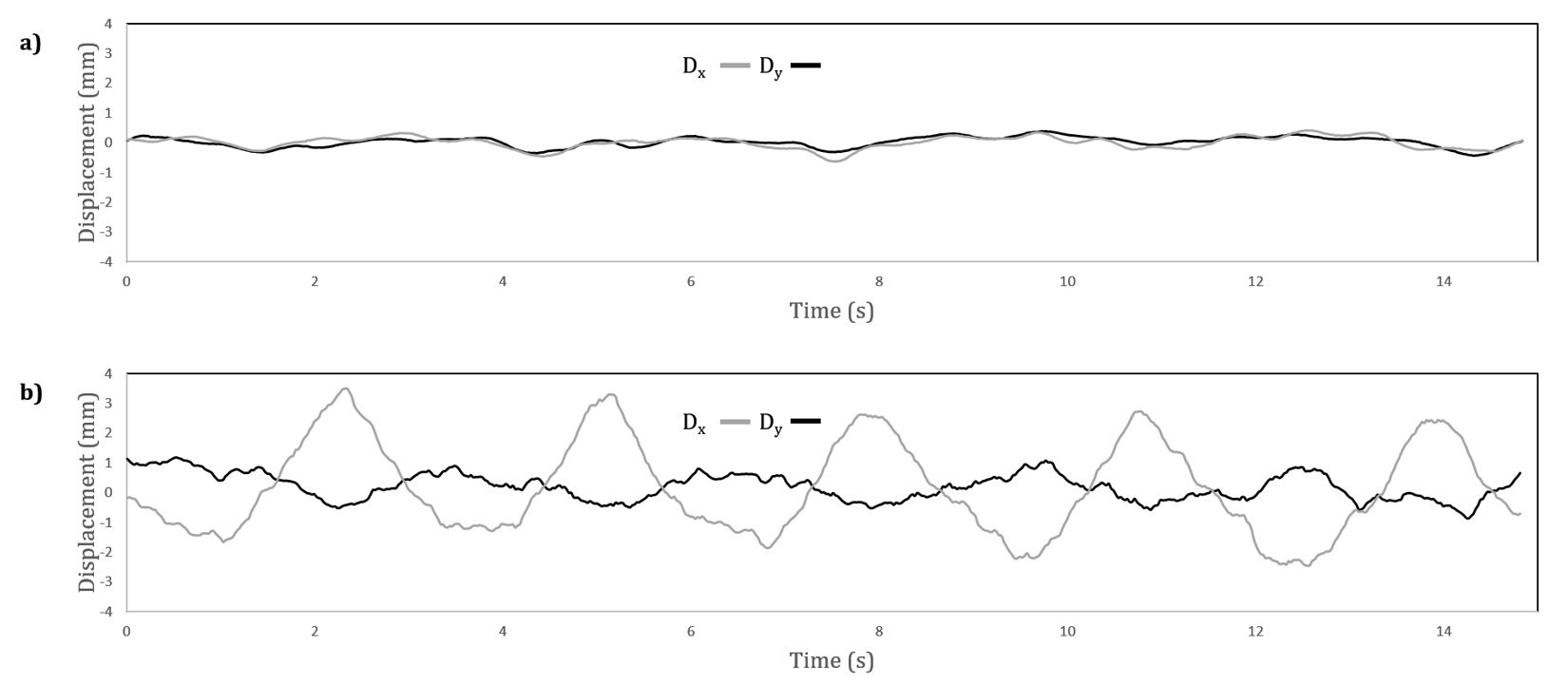
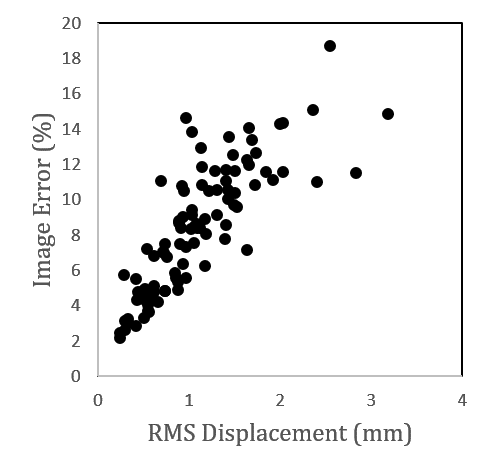
Overall, dynamic fetal cardiac anatomy could be assessed by both the real-time and reordered CINE reconstructions. In-plane motion was estimated from the real-time images, and the root-mean-squared (RMS) heart displacement over time ranged from 0.5 to 2.2 mm across all subjects. The fetal heart rate was also calculated from the real-time images and the average ranged from 118 to 170 bpm. Fig. 2 shows representative displacement curves for cases with minor (Fig. 2 a) and more dramatic (Fig. 2 b) in-plane motion. Real-time and reordered CINE reconstructions corresponding to these cases are presented in Figs. 3 and 4 respectively (click on figures to play videos). For the case with minor in-plane motion (Fig. 3), reordered CINEs (Fig. 3 b & c) showed improved image quality over real-time reconstructions (Fig. 3a). For example, a right ventricular diverticulum (Fig. 3b), and hepatic vessels (Fig. 3c) are better resolved in the reordered CINE reconstructions. However, there were negligible differences between reconstructions pre (Fig. 3b) and post (Fig. 3c) motion correction for this case due to the minor level of in-plane displacement. Conversely, the case with significant in-plane motion (Fig. 4) showed differences in spatial blur when comparing reconstructions pre (Fig. 4b) and post (Fig. 4c) motion-correction. These qualitative results agree with quantitative evaluation of reconstructions (Fig. 5). Image error, obtained by comparing images pre and post motion correction, increased with increasing displacement of the fetal heart. In particular, for RMS displacements larger then the acquired spatial resolution (1 mm) the image error is greater then 10% indicating a significant increase in image blur (1). These results highlight the need for motion correction strategies in fetal cardiac MRI.Discussion
High resolution imaging of the fetal heart was possible using a golden-angle radial acquisition. Real-time image reconstruction of the data enabled calculation of in-plane displacement and fetal heart rate. These parameters were then used to create motion-robust reordered CINE reconstructions. Dynamic cardiac anatomy was well visualized in both real-time and reordered CINE reconstructions, with fine cardiac structures best assessed using the motion-corrected reordered CINE images. This reconstruction framework has the potential to facilitate studies of the fetal heart using MRI, and scanning of fetuses at younger gestation where movement is more problematic.Acknowledgements
No acknowledgement found.References
1. Roy CW., Seed M., Macgowan CK. Accelerated MRI of the fetal heart using compressed sensing and metric optimized gating. Magn Reson Med 2016;0:1–11. Doi: 10.1002/mrm.26290.
2. Roy CW., Seed M., Macgowan CK. High resolution multislice imaging of the fetal heart using MOG and iGRASP. Scmr 2016;18(Suppl 1):1–2. Doi: 10.1186/1532-429X-18-S1-P44.
3. Kellman P., Chefd’hotel C., Lorenz CH., Mancini C., Arai AE., McVeigh ER. High spatial and temporal resolution cardiac cine MRI from retrospective reconstruction of data acquired in real time using motion correction and resorting. Magn Reson Med 2009;62(6):1557–64. Doi: 10.1002/mrm.22153.
4. Hansen MS., Sørensen TS., Arai AE., Kellman P. Retrospective reconstruction of high temporal resolution cine images from real-time MRI using iterative motion correction. Magn Reson Med 2012;68(3):741–50. Doi: 10.1002/mrm.23284.
5. van Amerom JFP., Kuklisova Murgasova M., Price AN., et al. Fetal cardiac cine imaging from motion-corrected super-resolution reconstruction of highly-accelerated real-time MRI. Proc Int Soc Magn Reson Med 2016:458.
6. Chaptinel J., Mivelaz Y., Yerly J., et al. A Golden-Angle Acquisition Coupled with k-t Sparse SENSE Reconstruction for Fetal Self Retro-Gated Cine Cardiac MRI: an In Vivo Feasibility Study. Int Soc Magn Reson Med 2016;(3):459.
7. Gamper U., Boesiger P., Kozerke S. Compressed sensing in dynamic MRI. Magn Reson Med 2008;59(2):365–73. Doi: 10.1002/mrm.21477.
Figures