0742
AN MR-SAFE METAL-BRAIDED CATHETER DESIGN FOR INTERVENTIONAL CMR1Cardiovascular and Pulmonary Branch, Division of Intramural Research, National Heart Lung and Blood Institute, NIH, Bethesda, MD, United States, 2Institute of Biomedical Engineering, Bogazici University, Istanbul, Turkey
Synopsis
Interventional cardiovascular magnetic resonance (iCMR) can enable radiation-free catheterization procedures. However, the lack of MR-safe devices limits clinical iCMR procedures. An MR-safe, metal-braided catheter that avoids RF-heating at 1.5 Tesla was prototyped. RF-heating of the device was eliminated by virtue of segmenting its metal components. RF-safety and mechanical integrity were confirmed through in vitro tests per ASTM standards. The proposed method could be an attractive technique to construct MR-safe metal-braided catheters for iCMR procedures.
PURPOSE
Interventional Cardiovascular Magnetic Resonance (iCMR) is an attractive alternative to X-Ray guided interventional procedures, as it avoids ionizing radiation and provides superior soft tissue contrast. Despite the technical developments in MRI, advances in iCMR remain incremental due to the lack of MRI-compatible devices, i.e. catheters and guidewires1.
Most commercial catheters incorporate metal braids in order to provide the required torque response and pushability. However, metal braids are subject to radiofrequency (RF)-induced heating under MR. The resultant temperature rise can be significant and may risk patient safety. Replacing metal wires in braids with polymer fibers avoids heating, however results in inferior mechanical, hence operational, performance2. Alternatively, if the electrical length of the conductors is restricted to its quarter-wavelength at a specified Larmor frequency, standing wave formation, thus, heating may be eliminated3, 4. This critical electrical length is approximately 10 cm at 1.5 Tesla (T) in humans5.
Here we demonstrate feasibility of a segmented, metal-braided 7 Fr catheter design that is MR-safe at 1.5 T.
METHODS
To circumvent RF heating, we first constructed a 1 meter long braided catheter sample using 16 PFA (Perfluoroalkoxy alkane)-insulated stainless steel wires on a vertical braiding machine (K80/16, Steeger Inc, US). The braid was then segmented by laser cutting two adjacent wires every 10 centimeters using a 1064 nm Nd:YAG laser system (Lasag, Switzerland). Segmentation was performed according to a helical segmentation pattern (Figure 1), which interrupted electrical conduction yet allowed to sustain a continuous braid structure.
RF-induced heating tests were performed on continuous- and segmented-braid samples according to ASTM 21196 at 1.5 T (Aera, Siemens, Germany) using SSFP and GRE sequences (TE/TR=1.7/3.4 ms, flip angle=50°, FOV=300 mm, matrix=192x192, slice thickness=6 mm). Temperature was measured using a fiberoptic temperature probe (OpSens, Canada) as previously described7.
To confirm that braid segmentation does not compromise mechanical performance of a braided catheter, torque response (torquability) and tensile tests were performed on a bare wire-braided tube that mechanically resembles a catheter. All mechanical test methods were described in a previous work 7.
RESULTS
Braid wire segmentation was confirmed visually under a light microscope (Hirox KH-1300, NJ) (Figure 2).
RF-heating tests conducted on the segmented- and continuous-braid samples revealed a temperature increase of 0.1 °C and 54.8 °C, respectively (Figure 3).
In addition, we measured torque response of the continuous- and segmented-braid samples, as shown in Figure 4.
Table 1 depicts tensile strength of the continuous- and segmented-braid samples.
Table 1: Tensile test results show the force at break measured when samples are placed under tensile stress.
| Force (N) | |||
| Continuous-braid | Segmented-braid | ||
| Distance (mm) | 5 | 46.5 | 46.3 |
| 10 | 72.3 | 68.6 | |
| 15 | 76.7 | 76.7 | |
DISCUSSION
A braid structure consisting of 16 individually insulated wires was developed in-house. It was evaluated for RF-heating, but not for mechanical properties, because the materials used in its construction (except the braiding wires) were insufficient to construct a commercial-grade catheter. Therefore, to test the effect of segmenting a braid on mechanical integrity, a bare-wire braided catheter shaft sample was segmented in the same helical pattern as the in-house sample, then evaluated mechanically through comparison tests.
We detected RF-induced temperature increase up to 54.8 oC in a braid structure that was constructed in-house, using insulated wires and a conventional catheter braid pattern. When this pattern was segmented helically at quarter-wavelength intervals, we showed that the observed temperature increase reduced to clinically insignificant (<2 oC) levels. The segmentation pattern followed in this study is important in that it disrupts electrical continuity, yet preserves mechanical integrity; mechanical tests indeed confirmed that the segmentation pattern of the metal braid does not compromise mechanical integrity.
CONCLUSION
We demonstrate that segmenting an insulated-metal braid layer by laser cutting the braid wires in pairs at quarter-wavelength intervals successfully eliminates RF-induced heating under MRI. We show that this process is inconsequential to the mechanical performance of a braided catheter. This was achieved by constructing a braid structure using insulated wires, then segmenting it in a helical pattern, whereby electrical conduction is disrupted to eliminate RF-heating, yet overall continuity of the braid structure is preserved to maintain mechanical integrity. This would be an attractive technique to construct clinical-grade metal braided catheter devices for iCMR.Acknowledgements
Robert J. Lederman and Ozgur Kocaturk contributed equally to this work.References
1. Lederman R.J. Cardiovascular Interventional Magnetic Resonance Imaging. Circulation. 2005; 112:3009-3017.
2. Rogers T, Lederman R. Interventional CMR: Clinical Applications and Future Directions. Current Cardiology Report. 2015; 17(5):1–9.
3. Armenean C., Perrin E., Armenean M., et al. RF-Induced Temperature Elevation Along Metallic Wires in Clinical Magnetic Resonance Imaging: Influence of Diameter and Length. Magnetic Resonance in Medicine 2004; 52:1200–1206.
4. Pictet J., Meuli R., Wicky S., et al. Radiofrequency heating effects around resonant lengths of wire in MRI. Physics in Medicine and Biology. 2002; 47:2973–2985.
5. Yeung CJ, Susil RC, Atalar E. RF safety of wires in interventional MRI: using a safety index. Magnetic Resonance in Medicine. 2002; 47(1):187–93.
6. ASTM F2119-07(2013), Standard Test Method for Evaluation of MR Image Artifacts from Passive Implants, ASTM International, West Conshohocken, PA, 2013.
7. Basar B., Rogers, T., Ratnayaka, K., et al. Segmented nitinol guidewires with stiffness-matched connectors for cardiovascular magnetic resonance catheterization: preserved mechanical performance and freedom from heating. Journal of Cardiovascular Magnetic Resonance. 2015; 17:105.
Figures
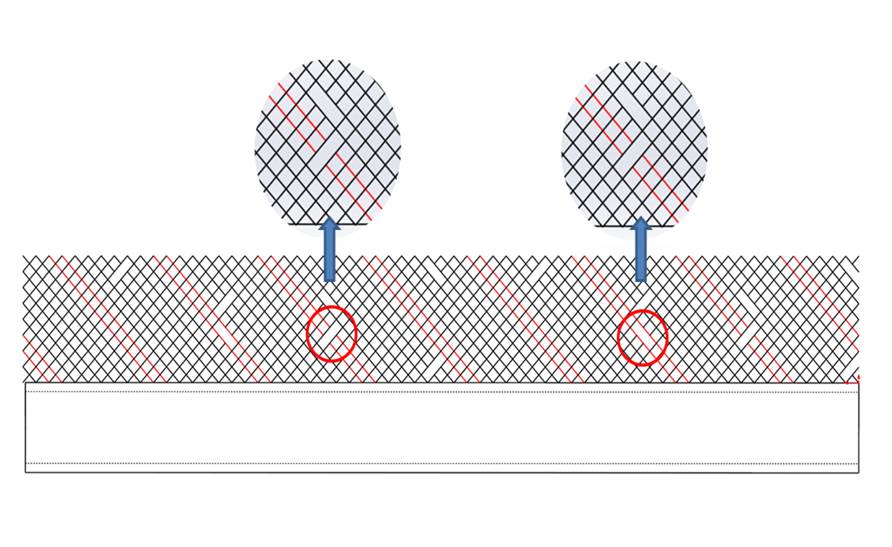
Schematic of a full cycle braiding segmentation pattern is shown on a 2D plane. The pair of red wires depicts the pattern of braid segmentation. The two red circles show the breaks in the pair of wires shown in red where they were segmented by laser cutting. As seen here, the pair of wires is laser cut at a 4-turn interval, which corresponds to 10 cm.
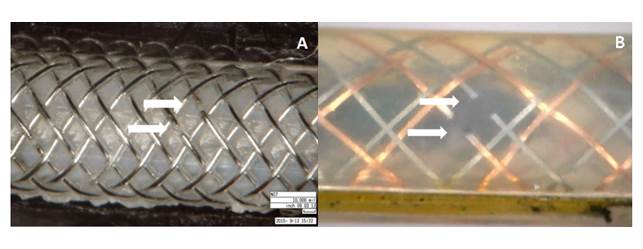
(a) The segmented-braid catheter sample that was developed in-house, and (b) and a bare-wire braided polymer tube that was commercially available are photographed under a light microscope. The segmentation points on the braiding are shown with white arrows.
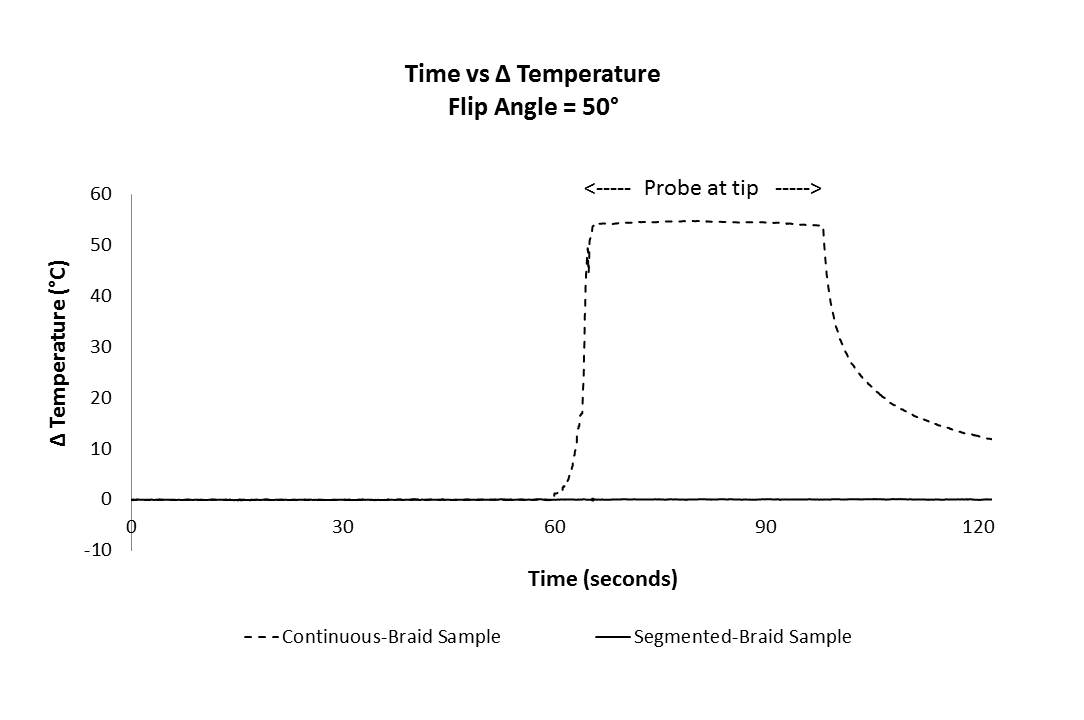
Temperature increase measured at the segmented catheter sample tip was 0.1 ºC in comparison to 54.8 ºC measured at the tip of the continuous-braid catheter sample. Probe was placed distally to the tip of each sample tested. Scanning was initiated at t=30 seconds. Probe was positioned at the distal tip at t=60 seconds. Temperature at the catheter samples’ tips was recorded for 30 seconds. Flip angle was 50º.
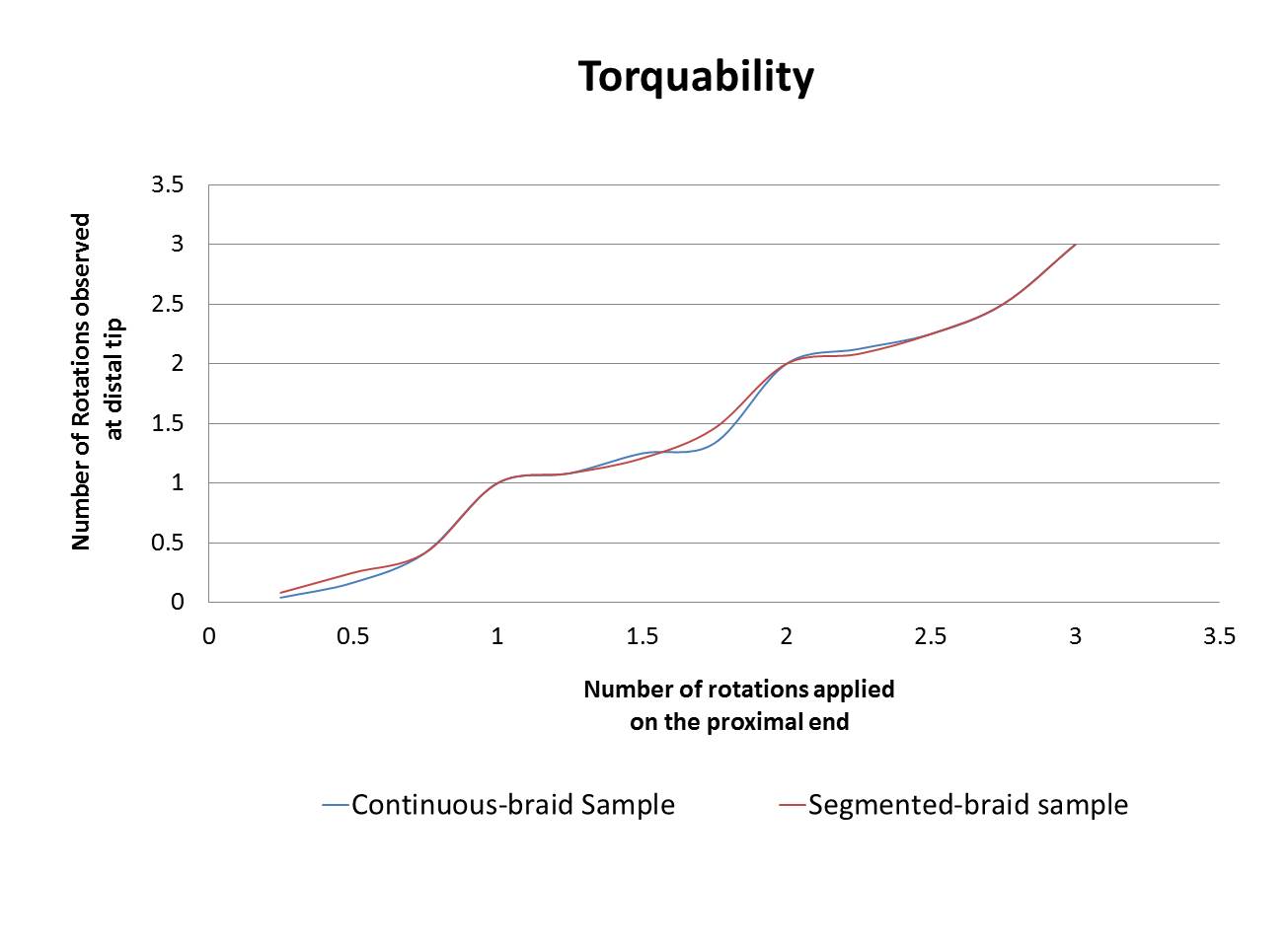
Torquability test results are depicted. The number of rotations applied on the proximal end of the continuous- and segmented-braid samples is graphed versus the number of rotations transmitted to (observed at) the distal end.