0684
Evidence of arteriovenous shunting in arterial spin labeling MRI in adults with sickle cell anemia1Radiology and Radiological Sciences, Vanderbilt University Medical Center, Nashville, TN, United States, 2Pediatrics - Division of Pediatric Neurology, Vanderbilt University Medical Center, Nashville, TN, United States, 3Radiology, University Medical Center Utrecht, Utrecht, Netherlands
Synopsis
High cervical arterial flow velocity may cause rapid erythrocyte transit through cerebral capillaries resulting in arteriovenous shunting, which may present as hyperintensities in pseudo-continuous arterial spin labeling (pCASL) MR difference images in draining veins. In an analysis of 36 adults with sickle cell anemia (SCA) and 11 age-matched controls, hyperintense superior sagittal sinus pCASL signal was present in 9% of controls and 61% of patients and correlated with elevated flow velocities. This shunting effect also trended with other markers of hemo-metabolic impairment in patients, such as elevated oxygen extraction fraction, elevated cerebral blood flow, and decreased blood hematocrit.
Introduction
High cervical arterial flow velocity may cause rapid erythrocyte transit through cerebral capillaries and impair efficiency of oxygen off-loading, resulting in arteriovenous shunting. Such shunting effects have been difficult to measure but may have relevance for oxygen extraction fraction (i.e., ratio of oxygen consumed to oxygen delivered), which depends partly on the duration of time for erythrocytes to traverse the capillary bed. Pseudo-continuous arterial spin labeling (pCASL) is an MRI technique that allows for cerebral blood flow (CBF) quantification after magnetically labeled blood water exchanges with tissue1. Labeled blood water that traverses capillaries without exchanging with tissue may lead to hyper-intense venous signal on the subtracted pCASL image (control – label). Patients with sickle cell anemia (SCA) have high blood velocities to compensate for reduced hemoglobin oxygen carrying capacity. The purpose of this study is to determine the prevalence of pCASL venous hyperintensity in such patients with elevated flow velocities, confirm the mechanism underlying this hyperintensity, and determine whether this novel metric corresponds with other tissue-level hemometabolic indicators of impairment.Methods
Experiment. SCA adult (n=36) and age-matched control (n=11) volunteers provided informed consent and were scanned at 3T (Philips Achieva). pCASL labeling was performed using a Hanning-windowed pulse-train with post-labeling delay=1900ms (spatial resolution=3x3x7 mm3; TR/TE = 3675/13ms; averages=20). Single-slice phase contrast angiography (PCA) data2 were acquired at the approximate level of the pCASL labeling plane for the left and right internal carotid arteries (ICAs) (velocity-encoding gradient=40 cm/s; in-plane spatial resolution=0.5x0.5 mm2). For OEF determination, TRUST data3 were acquired at a location 20 mm superior to confluence of the sinuses from an imaging slice containing the superior sagittal sinus (TR/TE=1978/3.6 ms; spatial resolution=3.4x3.4x5mm3). Blood hematocrit was measured in all subjects from venipuncture.
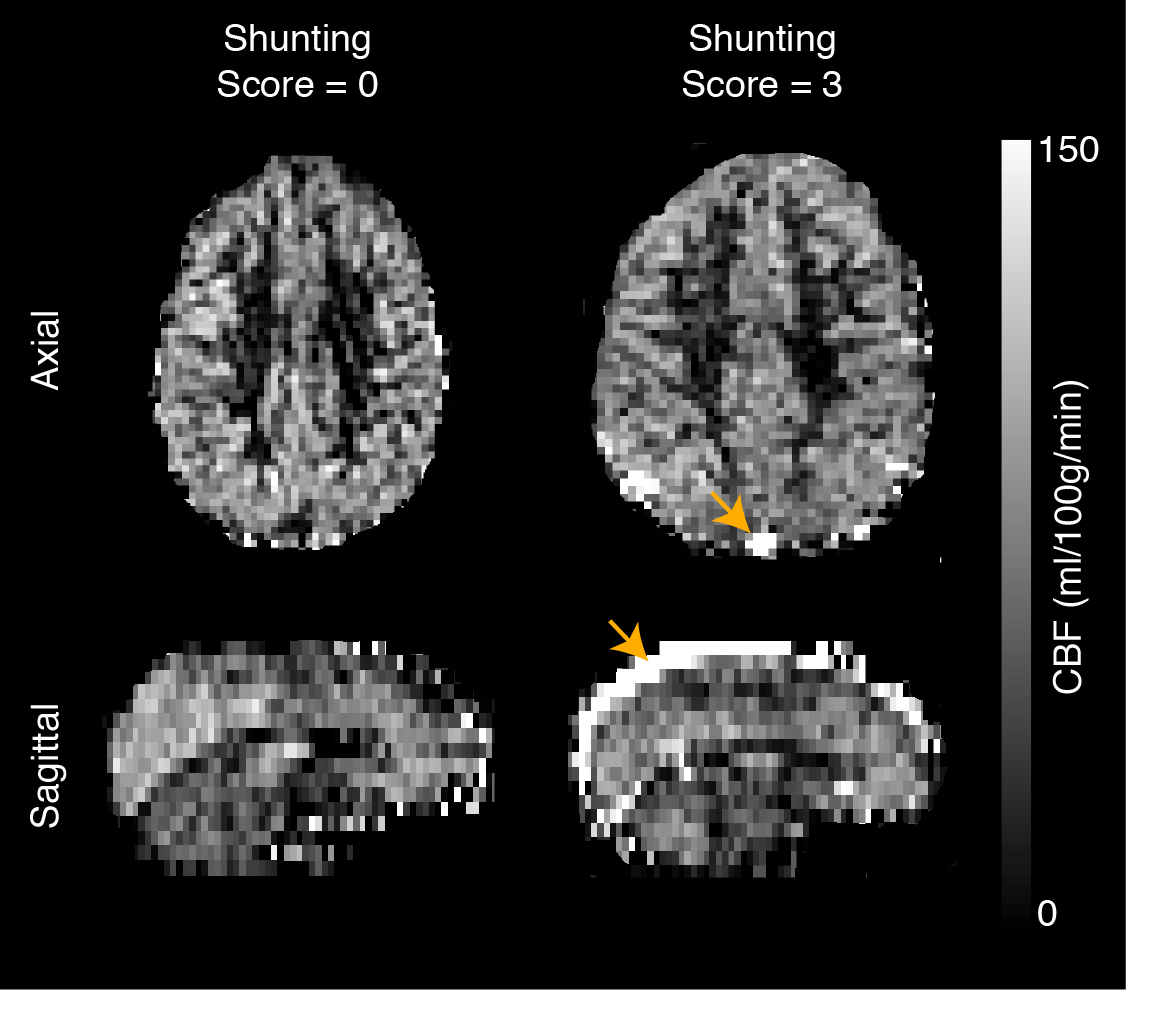
Analysis. CBF images were derived from the pCASL data utilizing a recommended kinetic model4 and gray matter CBF was computed for each participant. For categorical assessment of shunting, three reviewers (two imaging physicists and one stroke neurologist) independently assessed the CBF images for hyperintensity in the superior sagittal sinus and assigned scores of 0=none, 1=mild focal, 2=significant focal, or 3=significant diffuse hyperintensity. A consensus score for each participant was determined. For participants in whom shunting was discovered (i.e. shunting score > 0), venous hyperintensity was quantified as the mean signal inside the sagittal sinus in the superior parietal lobe. For velocity assessment, mean velocities were computed inside vessel masks and averaged across left and right ICAs. For OEF measurement, TRUST data were quantified5 to compute venous blood T2. Venous T2 was then converted to venous oxygen saturation (Yv) and, along with arterial oxygenation saturation (Ya), to OEF as (Ya-Yv)/Ya. Wilcoxon rank-sum tests were applied to determine differences of study measurements at two-sided significance level of 0.05. Spearman’s correlation testing was applied to evaluate relationships between study measurements at a significance level of 0.05.
Results
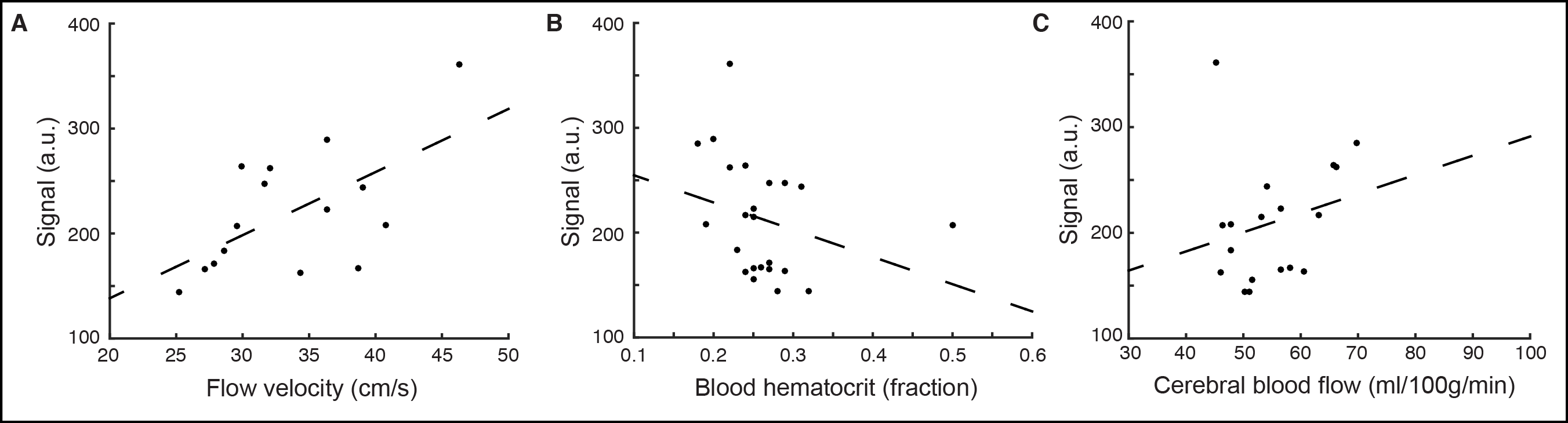
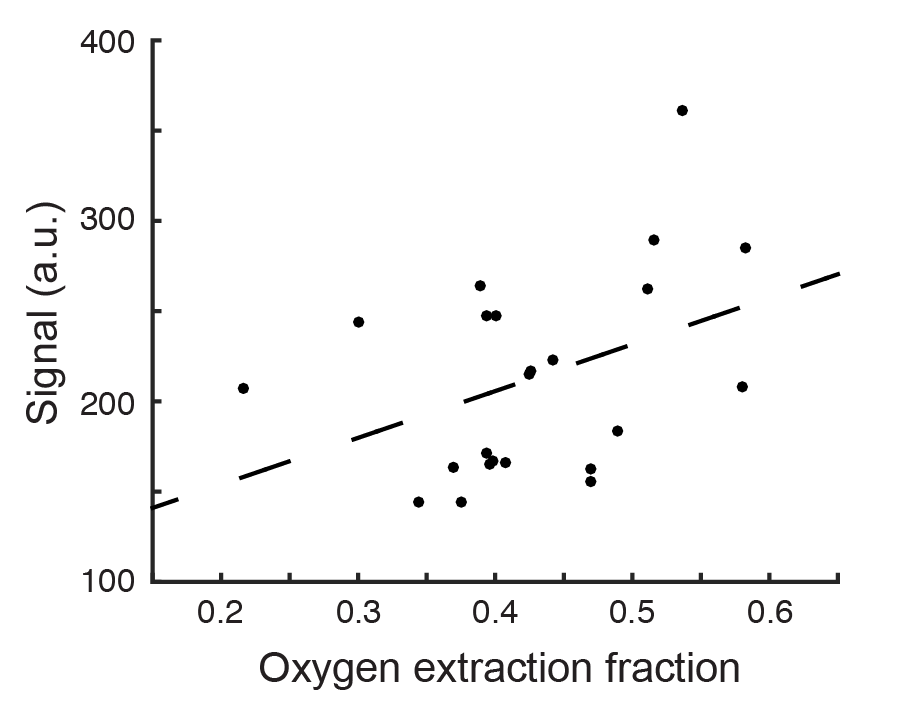
Arteriovenous shunting (Figure 1) was found in the CBF images of 1/11 controls (9%) and 22/36 adults with SCA (61%). Inter-observer agreement was high (Fleiss’ κ=0.91), and consensus shunting score in SCA adults (1.2±1.1) was significantly (p<0.01) higher than in controls (0.1±0.3). In participants with venous hyperintensity present (i.e. shunting score > 0) and velocity data available, the mean hyperintensity in the superior sagittal sinus was strongly correlated (Figure 2) with cervical flow velocity (ρ=0.53; p<0.05). In addition, trends for a relationship (Figure 3) between mean hyperintensity and OEF (ρ=0.40; p=0.06) and for a relationship (Figure 2C) between mean hyperintensity and CBF (ρ=0.36; p=0.15) were observed. The mean hyperintensity was strongly correlated (Figure 2B) with blood hematocrit in adults with SCA (ρ=-0.49; p<0.05).Discussion
High cervical arterial flow velocity may cause rapid erythrocyte transit through cerebral capillaries and impair efficiency of oxygen off-loading to brain tissue, resulting in capillary arteriovenous shunting. This effect would manifest as a hyperintensity in subtracted ASL data, and we have demonstrated that this contrast is more prevalent in adults with SCA and high cervical flow velocity compared to controls. Furthermore, the degree of hyperintensity in the superior sagittal sinus is correlated with cervical ICA flow velocity and reduced hematocrit, as expected. Finally, these hyperintensities trend with increasing OEF, an indicator of impairment in SCA5. These findings indicate that the presence and degree of venous hyperintensity in pCASL data may be due to arteriovenous shunting and reflect a new measure of impairment.Conclusion
Venous hyperintensity in ASL images may indicate arteriovenous shunting, due to elevated flow velocities, and may reflect markers of impairment in adults with SCA such as elevated OEF, elevated CBF, and decreased blood hematocrit.Acknowledgements
No acknowledgement found.References
1. Dai W, Garcia D, de Bazelaire C, et al. Continuous flow-driven inversion for arterial spin labeling using pulsed radio frequency and gradient fields. Magn Reson Med. 2008;60:1488-1497.
2. Aslan S, Xu F, Wang PL, et al. Estimation of labeling efficiency in pseudocontinuous arterial spin labeling. Magn Reson Med. 2010;63:765-771.
3. Lu H, Ge Y. Quantitative evaluation of oxygenation in venous vessels using t2-relaxation-under-spin-tagging mri. Magn Reson Med. 2008;60:357-363.
4. Alsop DC, Detre JA, Golay X, et al. Recommended implementation of arterial spin-labeled perfusion mri for clinical applications: A consensus of the ismrm perfusion study group and the european consortium for asl in dementia. Magn Reson Med. 2015;73:spcone.
5. Jordan LC, Gindville MC, Scott AO, et al. Non-invasive imaging of oxygen extraction fraction in adults with sickle cell anaemia. Brain. 2016;139:738-750.
Figures