0660
Interobserver Agreement and Diagnostic Performance of LI-RADS v2014 on contrast-enhanced MRI for non-HCC malignancies.1Memorial Sloan Kettering Cancer Center, NY, NY, United States
Synopsis
Patients at risk for hepatocellular carcinoma (HCC) are often also at risk for intrahepatic cholangiocarcinoma (ICC) and combined hepatocellular cholangiocarcinoma (cHCC-ICC). The purpose of this study was to evaluate the sensitivity and specificity of MRI in 4 radiologists using LI-RADS v2014 and their inter-reader agreement for diagnosing
Introduction
Patients at risk for hepatocellular carcinoma (HCC) are often also at risk for intrahepatic cholangiocarcinoma (ICC) and combined hepatocellular cholangiocarcinoma (cHCC-ICC). The Liver Imaging Reporting and Data System (LI-RADS) provides an algorithm for reporting liver observations in patients at risk for HCC, but also includes descriptions of ancillary features (AF) that favor non-HCC malignancies (LR-M) with the goal of identifying masses that are considered malignant and not definitely HCC (1). The purpose of this study was to evaluate the sensitivity and specificity of MRI in 4 radiologists using LI-RADS v2014 and their inter-reader agreement for diagnosing non-HCC malignancies (ICC and cHCC-ICC).
Methods
The Institutional Review Board approved this retrospective study. Consecutive patients were included if they had pathologically proven HCC, ICC or cHCC-ICC and availability of pre-operative contrast-enhanced MRI between January 2000 to June 2015. The exclusion criteria were the presence of multiple lesions, pre-surgical treatment and poor image quality. The final study population consisted of 102 patients, 40 ICC, 11 cHCC-ICC, in addition to 51 size-matched HCC. After receiving instructions on the use of LI-RADS, two senior (SR) and two junior (JR) abdominal radiologists who were blinded to the pathologic diagnoses, reviewed each case to assign LI-RADS imaging features and a final LR category. A consensus was considered present if at least three of the four readers agreed on a feature or diagnosis. Otherwise, two different abdominal radiologists reviewed the remaining cases to reach a consensus. Sensitivity and specificity of each reader for non-HCC malignancies were calculated. Inter-reader agreements (kappa statistics) for ancillary features and LR-M diagnosis were analyzed.
Results
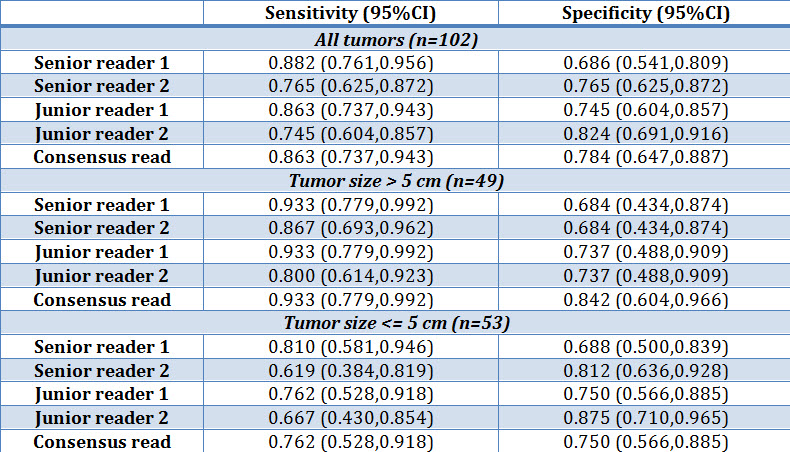
The sensitivity for non-HCC malignancies ranged from 74% to 88% across SR and JR, with specificity ranging from 69% to 82% (Table 1). The sensitivity and specificity of LR-M based on consensus read were 86% and 78%, respectively. Sensitivities for non-HCC malignancies were higher when radiologists analyzed 49 tumors that were larger than 5 cm (sens: 80% to 93%) compared to 53 tumors up to 5 cm or below (sens: 62% to 81%). Based on consensus read, 7 out of 51 (14%) non-HCC malignancies were not assigned an LR-M category, 4 (57%) of which were cHCC-CC and 3 were ICC. 4 tumors had no AF favoring non-HCC malignancies detected. One cHCC-ICC demonstrated tumor in vein, and was categorized as LR-5V. Imaging findings of these tumors are summarized in Table 2. The interreader agreement for the final LI-RADS category as LR-M or non LR-M were moderate for SR (kappa = 0.49, 95%CI 0.308-0.643) and JR (kappa = 0.573, 95%CI 0.405-0.709). The overall inter-reader agreement between all readers was moderate (kappa = 0.53, 95%CI 0.431-0.635). The overall interreader agreement for the identification of AF favoring non-HCC malignancy was also moderate (kappa = 0.431, 95%CI 0.326-0.541).
Conclusion
Applying LI-RADS v2014 and MRI, sensitivities between 74% to 88% can be achieved for the diagnosis of non-HCC malignancies, in line with previous report (2, 3). However, lower sensitivity was seen for smaller tumors, which are known to overlap with HCC in imaging appearance. These findings suggest that the absence of AF for non-HCC malignancies will not exclude ICC or cHCC-ICC in potential transplant patients with tumors smaller than 5 cm. Further research is needed with the goal of improving the diagnosis of non-HCC malignancies in patients where LI-RADS is applicable.
Acknowledgements
No acknowledgement found.References
1. American College of Radiology. Liver Imaging Reporting and Data System version 2014. [updated 2014. Available from: https://nrdr.acr.org/lirads/.
2. Potretzke TA, Tan BR, Doyle MB, Brunt EM, Heiken JP, Fowler KJ. Imaging Features of Biphenotypic Primary Liver Carcinoma (Hepatocholangiocarcinoma) and the Potential to Mimic Hepatocellular Carcinoma: LI-RADS Analysis of CT and MRI Features in 61 Cases. AJR American journal of roentgenology. 2016;207(1):25-31.
3. Hwang J, Kim YK, Park MJ, Lee MH, Kim SH, Lee WJ, et al. Differentiating combined hepatocellular and cholangiocarcinoma from mass-forming intrahepatic cholangiocarcinoma using gadoxetic acid-enhanced MRI. Journal of magnetic resonance imaging : JMRI. 2012;36(4):881-9.
Figures