0655
Simultaneous Multi-Slice Accelerated High Resolution MRI of the Knee: Comparison with In-plane Parallel Imaging Acceleration1The Johns Hopkins University School of Medicine, Baltimore, MD, United States, 2Orthopaedic University Hospital Balgrist, 3University of Minnesota, 4Zhejiang University, 5Siemens Healthcare USA
Synopsis
Simultaneous multi-slice acceleration techniques excite, acquire, and reconstruct multiple slices simultaneously and provide the potential to create substantially accelerated clinical TSE protocols with similar spatial and contrast resolution to current TSE protocols. We quantified the signal-to-noise and contrast-to-noise ratios of various combinations of parallel and simultaneous multi-slice acceleration and compared two 4-fold accelerated TSE protocols against a clinical 2-fold accelerated TSE standard. Our results demonstrate that 4-fold TSE acceleration enables 43-60% shorter acquisition times with similar image quality, structural visibility and observer satisfaction than standard parallel imaging acceleration.
Introduction
Two-dimensional turbo spin echo (TSE) pulse sequences are widely used for MRI of the knee. Clinical protocols often include intermediate-weighted and fat-suppressed fluid-sensitive MR images, which provide excellent contrast resolution of musculoskeletal tissues. High spatial resolution with pixel sizes of 0.3-0.4 x 0.3-0.4 mm2 visualizes fine detail and subtle abnormalities, but may require acquisition times of 3-5 minutes per pulse sequence. Integrated parallel acquisition technique (PAT) for in-plane acceleration can improve acquisition speed through k-space under-sampling, but comes at the expense of substantial loss in signal to noise ratio (SNR) due to signal under-sampling and g-factor noise amplification. Simultaneous multi-slice (SMS) acceleration techniques excite, acquire, and reconstruct multiple slices simultaneously and thus permit shorter acquisition times through shorter repetition time (TR) [1, 2]. Because SMS acceleration does not have signal under-sampling and multi-slice CAIPIRINHA can help reduce the g-factor penalty [3, 4], SMS acceleration provides the potential to create substantially accelerated clinical TSE protocols with similar spatial and contrast resolution to current TSE protocols [5].Purpose
To quantify the signal-to-noise (SNR) and contrast-to-noise (CNR) ratios of various combinations of PAT and SMS acceleration and compared two 4-fold accelerated (PAT2-SMS2) high resolution TSE prototype protocols for MRI of the knee against a clinical 2-fold accelerated (PAT2) TSE standard.Methods
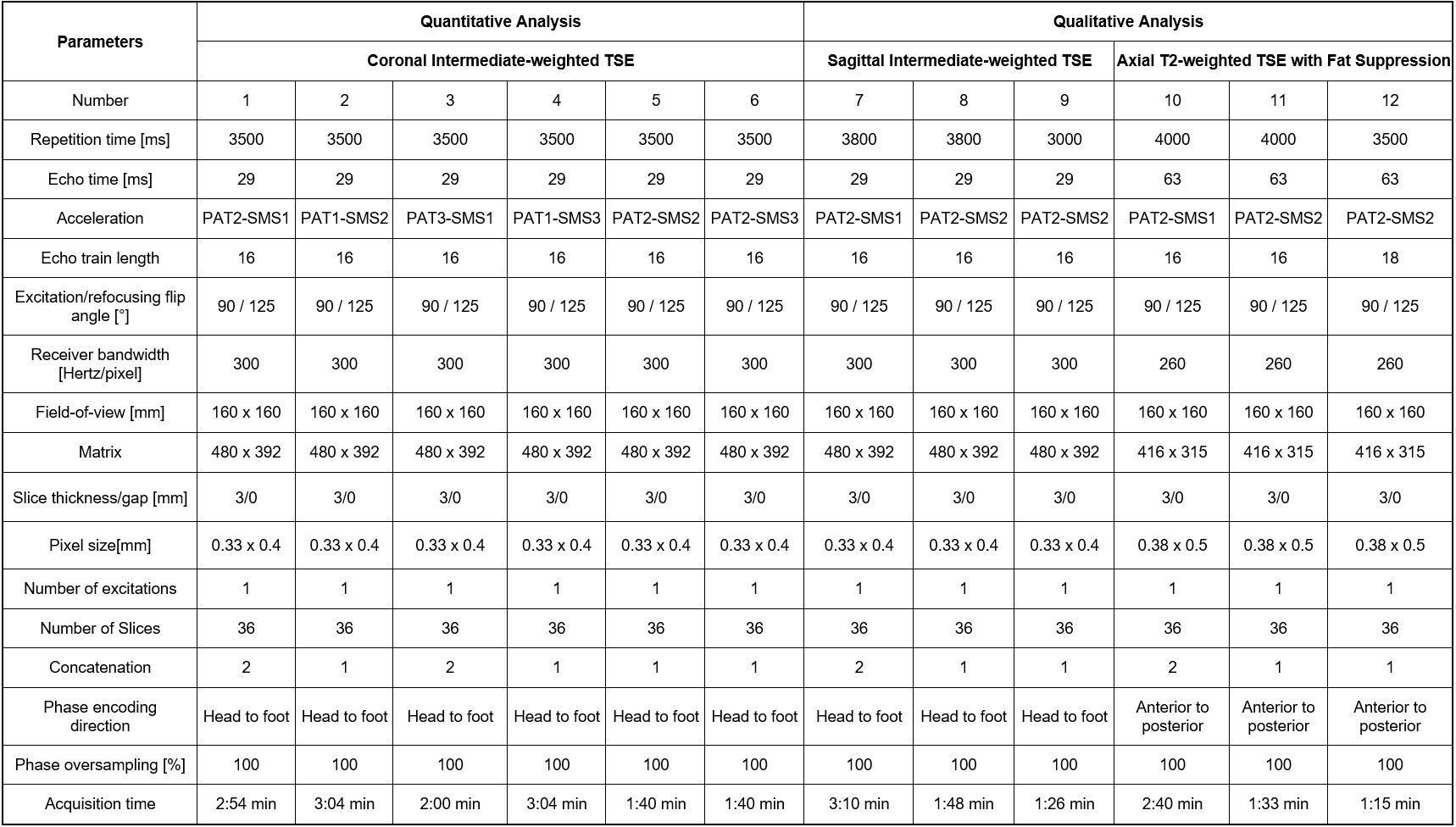
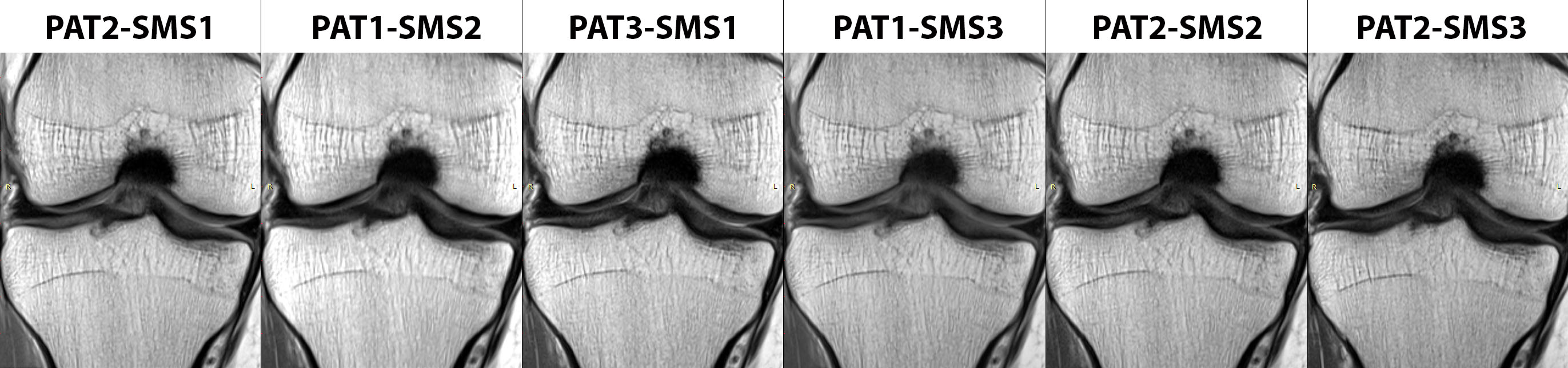
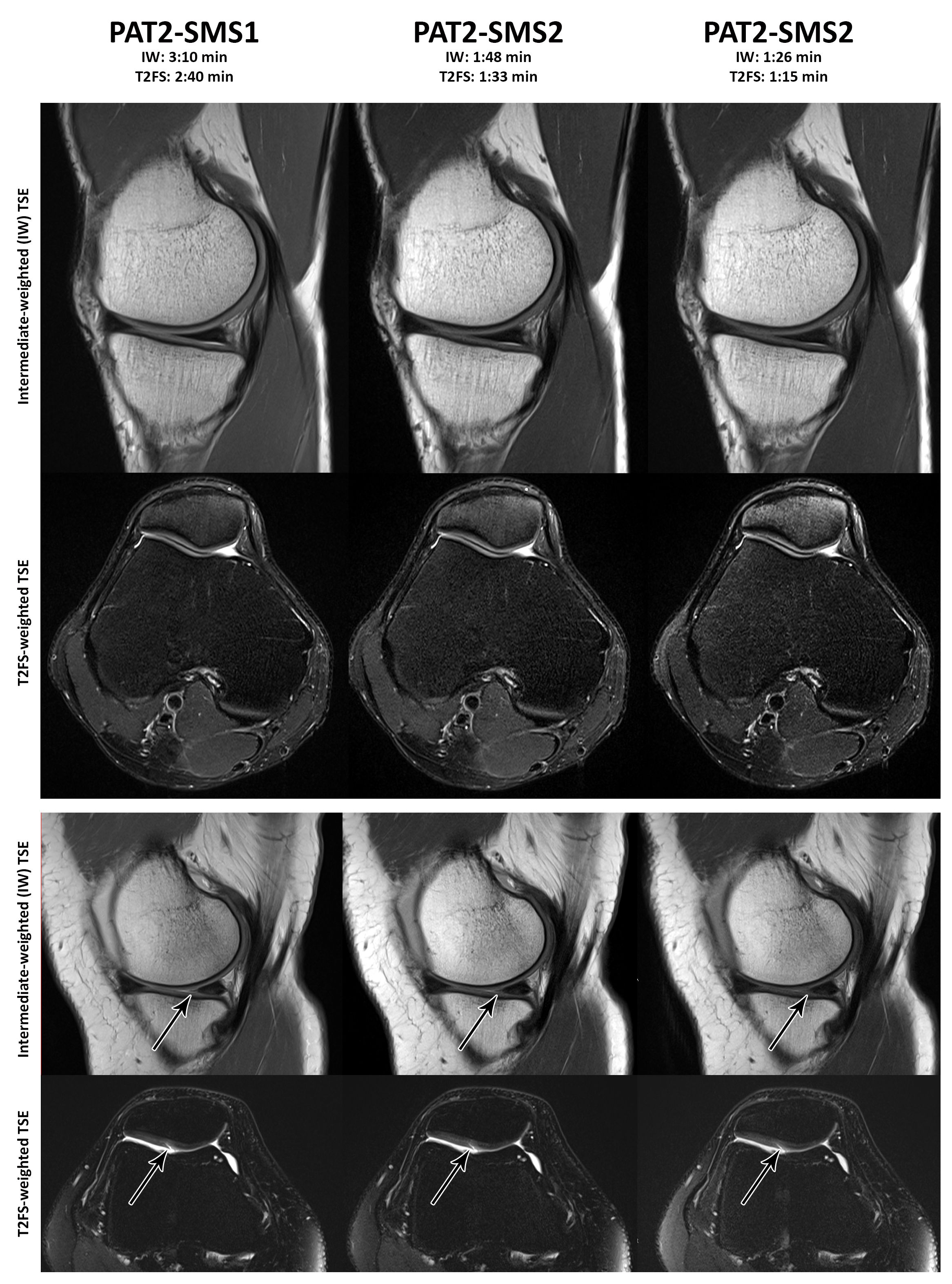
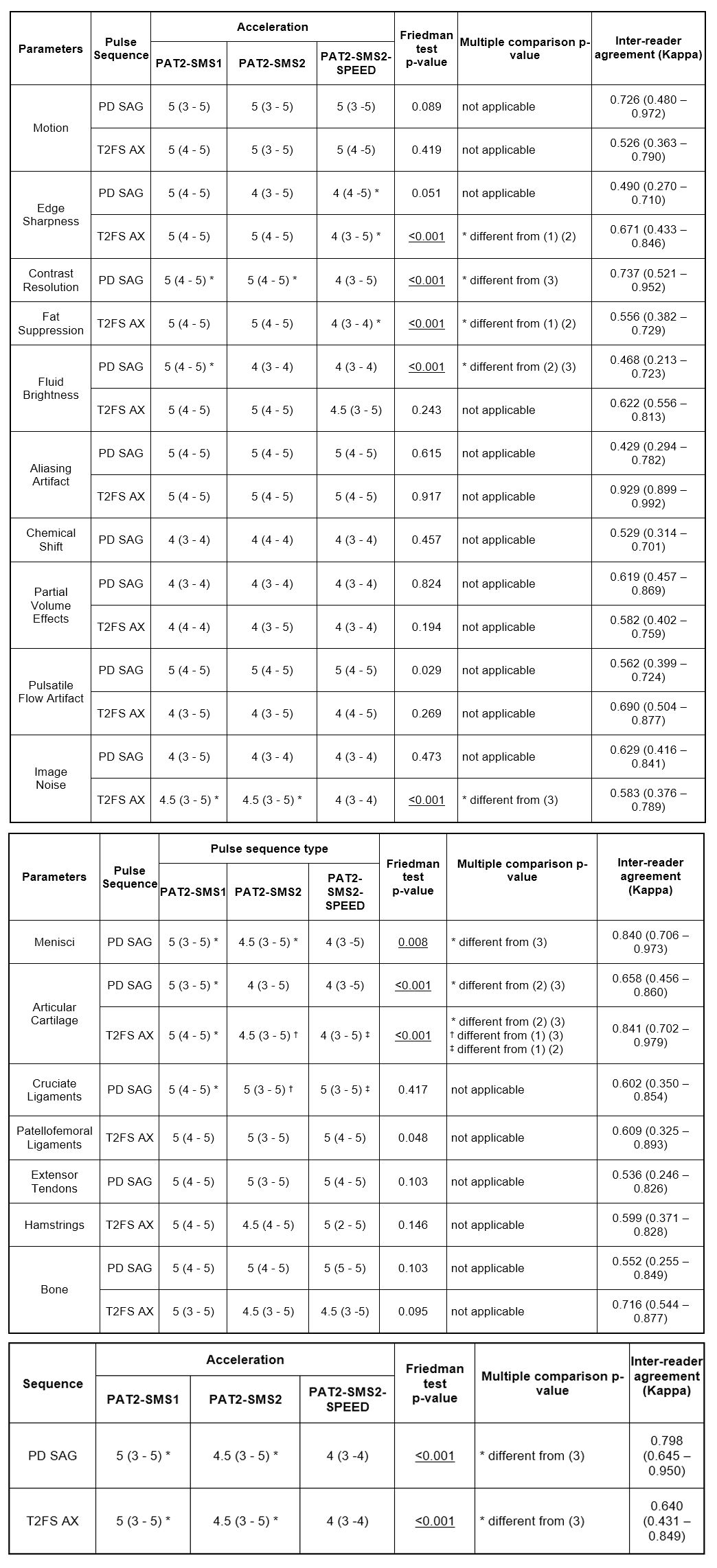
Institutional review board approval was obtained, and all subjects gave informed consent. Fourteen knees MRI exams were obtained (8 men, 6 women; mean age, 46 years; age range, 28–62 years) using a 3T MRI system (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) and a 1-channel transmit/15 channel receive coil (QED, Mayfield, OH). Predicted whole body specific absorption rates were recorded for all pulse sequences. For quantitative analysis, intermediate-weighted TSE pulse sequences with six different acceleration schemes including PAT2-SMS1, PAT3-SMS1, PAT1-SMS2, PAT1-SMS3, PAT2-SMS2, and PAT2-SMS3 were acquired twice and subtraction images were created (Figure 1, # 1-6). Using region-of-interest measurements, SNR was calculated with the difference method in accordance to SNRROI=[(SIimage1+SIimage2)/2]/(SQRT(2)xSD(SIimage1-SIimage2)) and CNR was calculated as |SNRROI1–SNRROI2|[6]. For qualitative analysis, sagittal intermediate-weighted (Figure 1, #7-9) and axial fat-suppressed T2-weighted (Figure 1, #10-12) MR images were obtained with PAT2-SMS1 and two PAT2-SMS2 acceleration schemes. For the PAT2-SMS1 and first PAT2-SMS2 protocols, TR/TE/ Echo Train Length (ETL) were kept constant, whereas for the second PAT2-SMS2 protocol, TR was lowered and ETL increased for T2FS in order to increase speed. Two fellowship-trained, full time musculoskeletal radiologists graded the randomized and blinded data sets in an independent fashion for image quality (motion, sharpness, contrast, fat suppression, fluid brightness, aliasing, chemical shift, partial volume effects, pulsatile flow artifacts, image noise), structural visibility (menisci, articular cartilage, cruciate and patellofemoral ligaments, extensor and hamstring tendons, bone) and overall observer satisfaction, using equidistant 5-point Likert scales. Friedman, Kruskal-Wallis, and inter-rater agreement tests were used. Bonferroni-corrected p-values of less than 0.01 were considered significant.Results
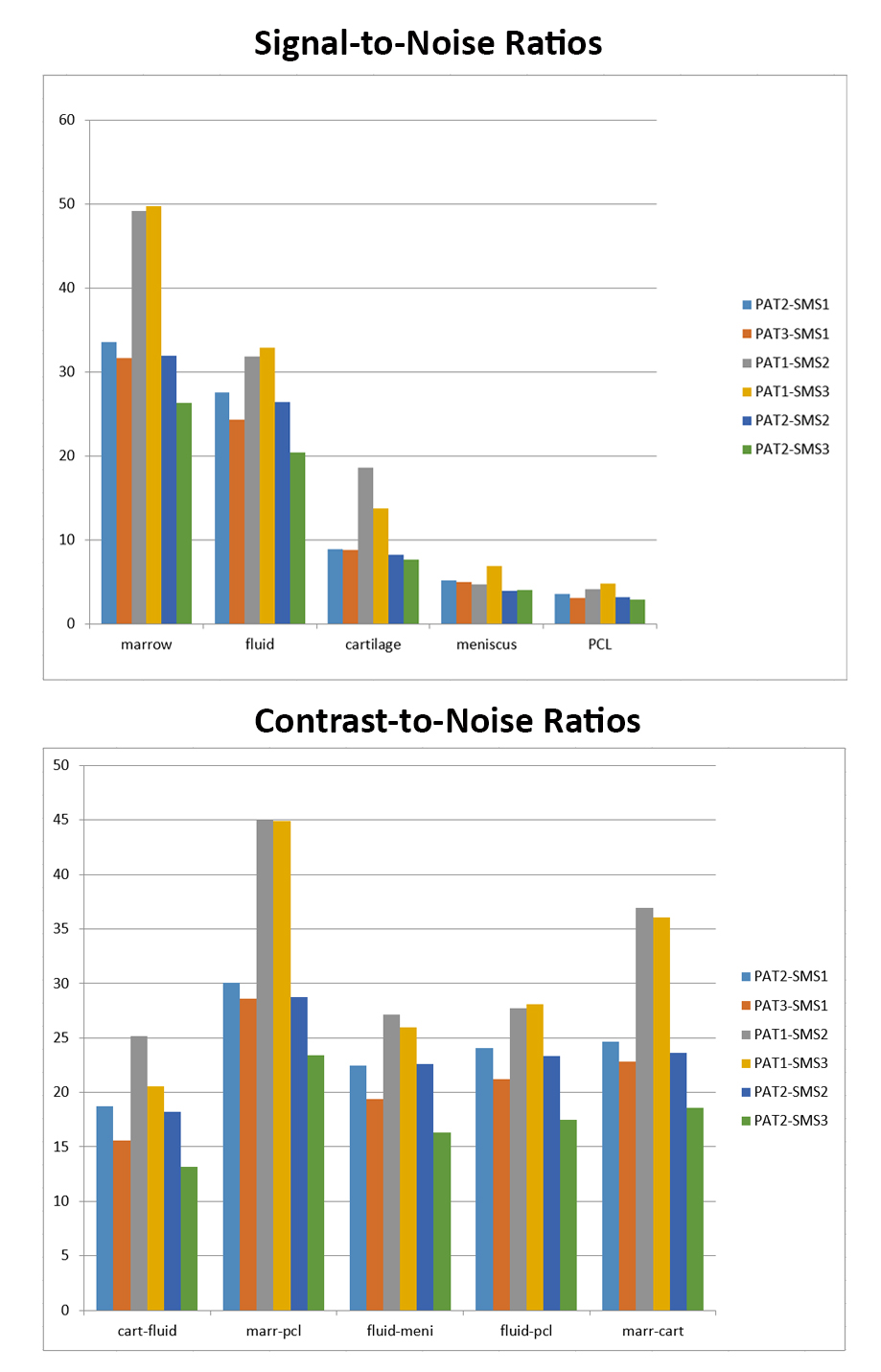
All pulse sequences were successfully executed and reconstructed inline. Whole body specific absorption rates (SAR) ranged between 1.4 and 3.9 W/lb and remained within mandated limits. Quantitative analysis demonstrated the signal preservation capabilities of SMS2 and SMS3 when compared to PAT2 and PAT3 and similar SNR and CNR of PAT2-SMS2 and PAT2 acceleration (Figure 2 and 3). Qualitative analysis showed no differences in motion artifacts and moderate to very good observer agreement. Fluid was brightest for PAT2, whereas image noise, edge sharpness, contrast resolution, and fat suppression were mildly inferior for the faster PAT2-SMS2 images (Figures 4 and 5). Articular cartilage received mildly higher grades on PAT2 images, whereas visibility of menisci was mildly inferior on the faster PAT2-SMS2 images. Observer grades for preferences were similarly high for PAT2-SMS1 and PAT2-SMS2, whereas grades were mildly inferior for the faster PAT2-SMS2 images.Discussion
Our results indicate that a 4-fold TSE acceleration through the combination of PAT2 and SMS2, which results in 43-60% shorter acquisition times, can achieve similar image quality, structural visibility and observer satisfaction than standard PAT2 acceleration. While our results demonstrate the near signal neutrality of SMS, SMS may result in mildly lower signal intensity of fluid and cartilage. The difference was minimal when TR was kept constant; however, increased when TR was lowered to additionally shorten acquisition time. We believe PAT2-SMS2 acceleration can be equivalent to PAT2, for which a clinical study is needed for confirmation.Conclusion
Four-fold acceleration TSE through the combination of PAT2 and SMS2 enables 43-60% shorter acquisition times with similar image quality, structural visibility and observer satisfaction than standard PAT2 acceleration and holds promise for a meaningful increase of the efficiency of clinical MRI of the knee.Acknowledgements
Grant support from NIH P41 EB015894References
[1] Larkman DJ, Hajnal JV, Herlihy AH, Coutts GA, Young IR, Ehnholm G. Use of multicoil arrays for separation of signal from multiple slices simultaneously excited. J Magn Reson Imaging. 2001;13:313–317.
[2] Moeller S, Yacoub E, Olman CA, Auerbach E, Strupp J, Harel N, Ugurbil K. Multiband multislice GE-EPI at 7 tesla, with 16-fold acceleration using partial parallel imaging with application to high spatial and temporal whole-brain fMRI. Magn Reson Med. 2010;63:1144-1153.
[3] Breuer FA, Blaimer M, Heidemann RM, Mueller MF, Griswold MA, Jakob PM. Controlled Aliasing in Parallel Imaging Results in Higher Acceleration (CAIPIRINHA) for Multislice Imaging. Magn Reson Med 2005;53:684–691.
[4] Setsompop K, Gagoski BA, Polimeni JR, Witzel T, Wedeen VJ, Wald LL. Blipped-Controlled Aliasing in Parallel Imaging for Simultaneous Multislice Echo Planar Imaging With Reduced g-Factor Penalty. Magn Reson Med 2012;67:1210-1224
[5] Wang D, Padua A, Ellermann J, Li X, Ugurbil K, and Deshpande V, "Multiband Slice Accelerated TSE for High Resolution Knee Imaging", International Society for Magnetic Resonance in Medicine 22th Scientific Meeting, Milan, Italy, May 2014
[6] Reeder SB, Wintersperger BJ, Dietrich O, et al. Practical approaches to the evaluation of signal-to-noise ratio performance with parallel imaging: application with cardiac imaging and a 32-channel cardiac coil. Magn Reson Med 2005; 54:748-754.
Figures