0627
MRI Detection of Extramural Venous Invasion in Rectal Cancer: Correlation with Histopathology Utilizing Elastin Stain1UHN, University of Toronto, Toronto, ON, Canada
Synopsis
Extramural venous invasion (EMVI) in Rectal cancer is an independent predictor of local and distant recurrence, nodal disease and overall survival. Accurate preoperative EMVI detection has implications for treatment decisions. Previously, MRI has been evaluated for this purpose previously against histopathology with Hematoxylin-Eosin(HE) staining. Recently histopathology with Elastin stain has been recommended for EMVI detection given its 2-3-fold increase in accuracy and improved prognostication compared to HE stain. The diagnostic performance of MRI for EMVI detection compared to elastin stain based histopathology is unknown and in this study, we present our results to address this issue.
Background
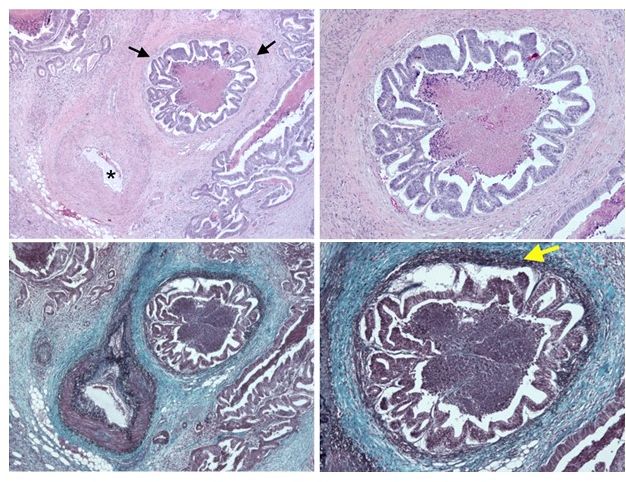
Extramural venous invasion (EMVI) is an independent predictor of local and/or distant recurrence [1], and reduced overall survival [2] in rectal cancer. Traditionally the histopathological diagnosis of EMVI (pEMVI) is based on assessment of H&E-stained slides. Recent studies show that application of special stains that identify elastin in vessel walls(Fig.1) dramatically increases the detection rate [3-4] and is increasing utilized as histological method of choice. [5].Previous studies correlating performance of MRI versus hisotpathology detection of EMVI have all been based on assessment of H&E stain[6-9] and the diagnostic performance of MRI versus elastin stain detected EMVI is currently unknown.Purpose
To evaluate the diagnostic performance of magnetic resonance imaging (MRI) for detection of extramural venous invasion (EMVI) in rectal cancer compared to histopathology using elastin staining.Methods
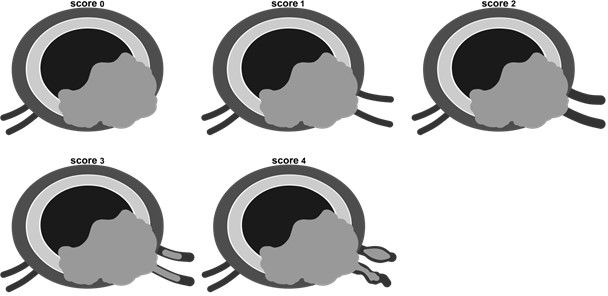
49 patients with rectal cancers who had undergone surgical resection with pre-operative MRI were identified. Thirty-seven patients had received pre-operative chemoradiation (CRT). The MRI examinations had been performed using 1.5T or 3T systems (Avanto or Verio, Siemens Healthcare sector, Erlangen, Germany) with phased-array coil and standard rectal protocol. Intravenous anti-peristaltic agent was used. The standard sequences included multiplanar T2-weighted (T2W) Fast Spin Echo imaging including high-resolution oblique imaging (perpendicular to the rectal tumor axis in the sagittal view). In addition, the protocol included multiparametric MRI sequences including diffusion-weighted imaging (DWI) and gadolinium contrast-enhanced (CE) MR imaging Sixty-nine MRI scans were independently reviewed by two blinded radiologists for EMVI using a scoring system (Fig.2) of 0‒4( 0‒1 as negative, 2 as equivocal, and 3‒4 as positive for EMVI). The imaging findings suggestive for EMVI included expansion and/or irregularity of vessels, loss of normal vascular flow void or contrast enhancement, or intraluminal intermediate tumoral signal intensity, contiguous or separated from the main tumor. Comparison was made with histopathology results obtained by two pathologists reviewing the elastin-stained slides in consensus. EMVI status was also correlated with other tumoral and prognostic features on imaging and pathology. Statistical analysis was performed using Fisher’s exact and McNemar tests.Results
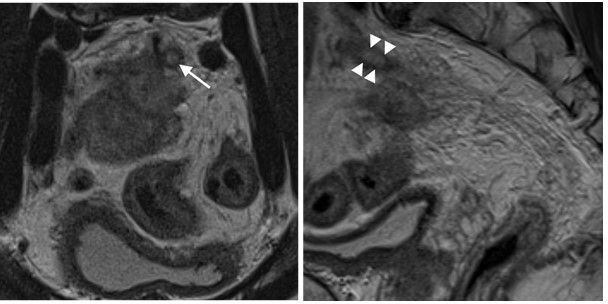
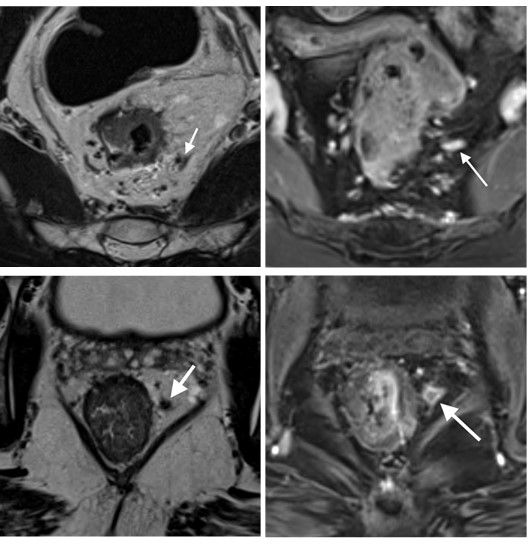
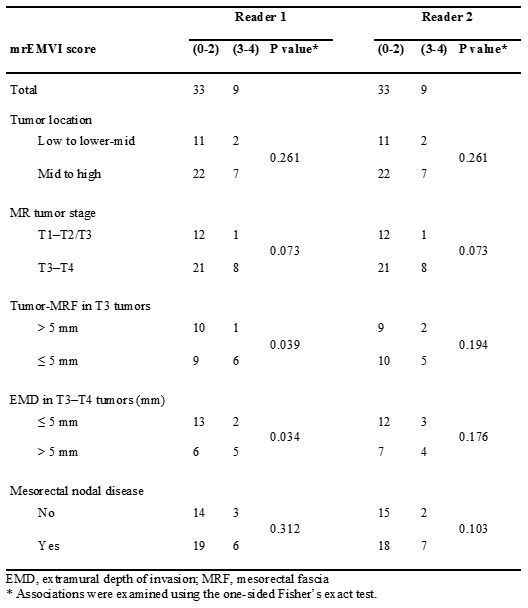
EMVI was present in 31% of the pathology specimens. MRI EMVI score of 3‒4 was 54% sensitive and 96% specific in detection of EMVI in veins with 3mm in diameter or larger(Fig.3). The interobserver reader agreement was excellent on baseline (kappa, 0.858), and good on post-treatment scans (kappa, 0.604). Addition of score 2 to the data pool of score 3-4 considered as positive for EMVI,increased sensitivity to 79% but decreased the specificity to 74% with poor PPV. Preoperative CRT had no significant detrimental impact on the diagnostic performance of MRI. For reader 1, the sensitivity and specificity of MRI were 50% and 92.9% respectively in both baseline and post-treatment scans (P=1.0). For reader 2, following the treatment despite unchanged specificity of 92.9% (P=1.0), the sensitivity decreased from 50% to 33%; however, this change was not statistically significant (P=1.0). Contrast-enhanced (CE) MRI increased reader confidence for diagnosis or exclusion of EMVI compared to T2-weighted (T2W) imaging(Fig.4). Inclusion of CE images correctly changed the EMVI status from equivocal to positive in 6 scans (3 for reader 1 and 3 for reader 2) and to negative in 4 scans (for reader 1) . Each reader had one false positive result when included CE images by incorrectly changing an equivocal status to positive. EMVI status correlated positively with depth of extramural invasion and proximity to mesorectal fascia(Fig.5)Discussion
In this study, when MRI score of greater than 2 was assigned as positive result for EMVI, MRI yielded 54% sensitivity and 96% specificity with marked precision by giving substantial interobserver agreement.The results of this study support MRI as an accurate modality for preoperative detection of EMVI in rectal cancer, maintaining moderate sensitivity and high specificity when compared with histopathology employing elastin staining which is known to increase sensitivity for pathological diagnosis 2-3-fold compared to H&E staining. MRI diagnosis of EMVI should be made when there is tumoral signal intensity within a vein to avoid false positive results given its prognostic and clinical implications. Contrast-enhanced MRI tends to increase confidence for diagnosis as well as exclusion of EMVI compared to T2 imaging alone. Preoperative CRT did not negatively impact the diagnostic performance of MRI for detection of EMVI in this study. Finally,there was close association between EMVI status and extent of mesorectal tumor extension and nodal disease but not with tumor size or grade .
Conclusion
Despite significant expected increase in sensitivity for EMVI detection by histopathology with elastin stain compared to HE stain, MRI proves to be an accurate modality for preoperative detection of EMVI, irrespective of patients having received pre-operative CRT.Acknowledgements
NoneReferences
1.Hunter CJ, Garant A, Vuong T, et al. Adverse features on rectal MRI identify a high-risk group that may benefit from more intensive preoperative staging and treatment. Annals of surgical oncology 2012; 19:1199-1205
2. Betge J, Pollheimer MJ, Lindtner RA, et al. Intramural and extramural vascular invasion in colorectal cancer: prognostic significance and quality of pathology reporting. Cancer 2012; 118:628-638
3.Kirsch R, Messenger DE, Riddell RH, et al. Venous invasion in colorectal cancer: impact of an elastin stain on detection and interobserver agreement among gastrointestinal and nongastrointestinal pathologists. The American journal of surgical pathology 2013; 37:200-210
4. Howlett CJ, Tweedie EJ, Driman DK. Use of an elastic stain to show venous invasion in colorectal carcinoma: a simple technique for detection of an important prognostic factor. Journal of clinical pathology 2009; 62:1021-1025
5.Messenger DE, Driman DK, Kirsch R. Developments in the assessment of venous invasion in colorectal cancer: implications for future practice and patient outcome. Human pathology 2012; 43:965-973
6.Smith NJ, Barbachano Y, Norman AR, Swift RI, Abulafi AM, Brown G. Prognostic significance of magnetic resonance imaging-detected extramural vascular invasion in rectal cancer. The British journal of surgery 2008; 95:229-23628.
7.Brown G, Radcliffe AG, Newcombe RG, Dallimore NS, Bourne MW, Williams GT. Preoperative assessment of prognostic factors in rectal cancer using high-resolution magnetic resonance imaging. The British journal of surgery 2003; 90:355-364
8.Smith NJ, Shihab O, Arnaout A, Swift RI, Brown G. MRI for detection of extramural vascular invasion in rectal cancer. AJR American journal of roentgenology 2008; 191:1517-1522
9. Chand M, Evans J, Swift RI, et al. The Prognostic Significance of Postchemoradiotherapy High-resolution MRI and Histopathology Detected Extramural Venous Invasion in Rectal Cancer. Annals of surgery 2015; 261:473-479
Figures