0620
Feasibility and evaluation of free-breathing and self-gated cartesian-sampled T1-weighted 4D MRI with compressed sensing resulting in combined diagnostic image quality and perfusion analysis1Diagnostic and Interventional Radiology, University Hospital Tuebingen, Tuebingen, Germany, 2Section on Experimental Radiology, University Hospital Tuebingen, 3Siemens Healthcare, Erlangen, Germany
Synopsis
In clinical practice, a remaining challenge of dynamic contrast-enhanced (DCE)-MRI is to acquire a high spatio-temporal resolution without motion artifacts and diagnostic quality, despite acquisitions over several minutes. In particular, iterative reconstruction techniques have brought free-breathing acquisitions in clinical range. In this study, we proved feasibility and evaluated a prototype Cartesian-sampled fat-saturated T1-weighted 3D gradient-echo sequence with automated respiratory self-gating and compressed sensing reconstruction (VIBESG-CS) for continuous dynamic contrast-enhanced (DCE) MRI and perfusion analysis including lesion detection of the liver using a Tofts model. VIBESG-CS including perfusion analyisis showed better motion robustness and similar lesion conspicuity compared to a standard morphology sequence (fat-saturated T2-TSE).
Purpose
To prove feasibility and evaluate free-breathing and self-gated (SG) fat-saturated T1-weighted 3D gradient-echo acquisitions with compressed sensing (CS) reconstruction for continuous dynamic contrast-enhanced (DCE) MR imaging and perfusion analysis.Methods and Materials
This IRB-approved study was performed according to the declaration of Helsinki. 15 patients (age: 16-80y) referred to abdominal and liver examination were imaged at 1.5 T (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). A prototypical Cartesian sampled self-gated T1-weighted 3D fat-saturated gradient echo sequence (1) and CS reconstruction (VIBESG-CS) was continuously acquired for 128 seconds starting with the administration of the contrast agent (Gadobutrol; Bayer Healthcare, Germany). Parameters of the VIBESG-CS acquisition included FoV = 380x285x210mm3, image matrix = 320x240x60, TE/TR= 1.79/3.69ms, flip angle = 10°. From the acquired raw data, 16 consecutive volumes (temporal resolution 8 seconds, spatial resolution 1.2x1.2x3 mm³) were reconstructed using 40% of the data chosen by best consistency of the assigned respiratory navigation signal. Perfusion analysis was performed with a post-processing prototype (Frontier MR DCE; Siemens Healthcare, Germany) using the Tofts model (6), with a focus on Ktrans as the most commonly used for pharmacokinetic parameter to assess of malignancy (7). We evaluated image quality and lesion conspicuity compared to a standard morphology sequence (fat-saturated T2-TSE). T2-TSE served as a standard of reference regarding lesion conspicuity. Parameters of the T2-TSE acquisition included FoV 360x285x180mm3, image matrix = 320x240x60, TE/TR= 100/5340ms, 1,1x1,1x6mm³. Image quality was assessed qualitatively (lesion conspicuity, overall image quality, hepatic edge sharpness, hepatic vessel clarity, differentiation of renal parenchyma, (respiratory) motion robustness and homogeneity of fat saturation; two readers independently; 5-point Likert scale; 5=excellent). Statistical analyses were performed using SPSS (Version 22, IBM, USA). Paired t-test was performed for quantitative measurements.Results
9 out of the 15 patients had liver metastases of primary abdominal malignancies. Overall image quality (4,7±0,5 vs 4,0±1,0), hepatic vessel clarity (4,4±0,7 vs 3,8±0,8), differentiation of renal parenchyma (4,9±0,3 vs 3,8±1,2), (respiratory) motion robustness (4,3±0,6 vs 3,8±1) and homogeneity of fat saturation (4,7±0,5 vs 3,8±0,8) were rated higher in VIBESG-CS and perfusion maps compared to T2-TSE (Fig. 1 and 3). Hepatic edge sharpness was rated similar to T2-TSE (4,3±0,7 vs 4,5 ± 0,9).
VIBESG-CS including perfusion analysis detected 45 of 48 liver lesions compared to fat-saturated T2-TSE.
4D DCE-MRI and the calculated parameter maps have the additional value of depicting perfusion patterns and tumor heterogeneity (Fig. 3, 4, and 5).
Discussion
Our initial results indicate that free-breathing and self-gated 4D DCE-MRI becomes feasible for Cartesian acquisitions with compressed sensing reconstruction at high temporal and spatial resolution, resulting in diagnostic image quality by providing better overall image quality, better motion robustness and similar lesion conspicuity by including perfusion analysis compared to standardized morphology sequence T2-TSE fs. As depicted in Fig. 3 and 4, 4D DCE-MRI and perfusion analysis provide a helpful tool to better characterize lesions regarding their arterialization and need of treatment, respectively. Therefore, VIBESG-CS is a promising approach to improve the validity and reliability of DCE-MRI and perfusion analysis. For calculating quantitative perfusion parameters as known from 4D CT imaging, in which a temporal resolution of around 2 seconds is achieved, spatial and temporal resolution in 4D DCE-MRI still needs to be improved to provide comparable additional information about the perfusion characteristics of pathologies. Organ perfusion could also be investigated in further studies, as drug-induced liver damage is a common side effect of modern chemotherapy such as check-point inhibitors.Conclusion
VIBESG-CS is applicable for continuous free-breathing self-gated 4D DCE-MRI at high temporal and spatial resolution with diagnostic image quality. It provides better image quality and motion robustness and similar lesion detection compared to a standard T2-weighted morphology sequence. In addition, 4D DCE-MRI and derived perfusion maps allow assessing perfusion patterns and tumor heterogeneity.Acknowledgements
No acknowledgement found.References
1. Nickel D, Chen X, Mailhe B, et al. Motion-resolved 3D dynamic contrast enhanced liver MRI. Proc Intl Soc MRM 24 (2016);4253.
2. Reiner CS, Neville AM, Nazeer HK, et al. Contrast-enhanced free-breathing 3D T1-weighted gradient-echo sequence for hepatobiliary MRI in patients with breath-holding difficulties. Eur Radiol 2013;23(11):3087-3093.
3. Kazmierczak PM, Theisen D, Thierfelder KM, et al. Improved detection of hypervascular liver lesions with CAIPIRINHA-Dixon-TWIST-volume-interpolated breath-hold examination. Invest Radiol 2015;50(3):153-160.
4. Feng L, Axel L, Chandarana H, et al. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn Reson Med 2016;75(2):775-788.
5. Chandarana H, Feng L, Block TK, et al. Free-breathing contrast-enhanced multiphase MRI of the liver using a combination of compressed sensing, parallel imaging, and golden-angle radial sampling. Invest Radiol 2013;48(1):10-16.
6. Chandarana H, Feng L, Ream J, et al. Respiratory Motion-Resolved Compressed Sensing Reconstruction of Free-Breathing Radial Acquisition for Dynamic Liver Magnetic Resonance Imaging. Invest Radiol 2015;50(11):749–756.
7. Tofts P. T1-weihgted DCE Imaging Concepts: Modelling, Acquisition and Analysis. Magnetom Flash 03/2010.
Figures
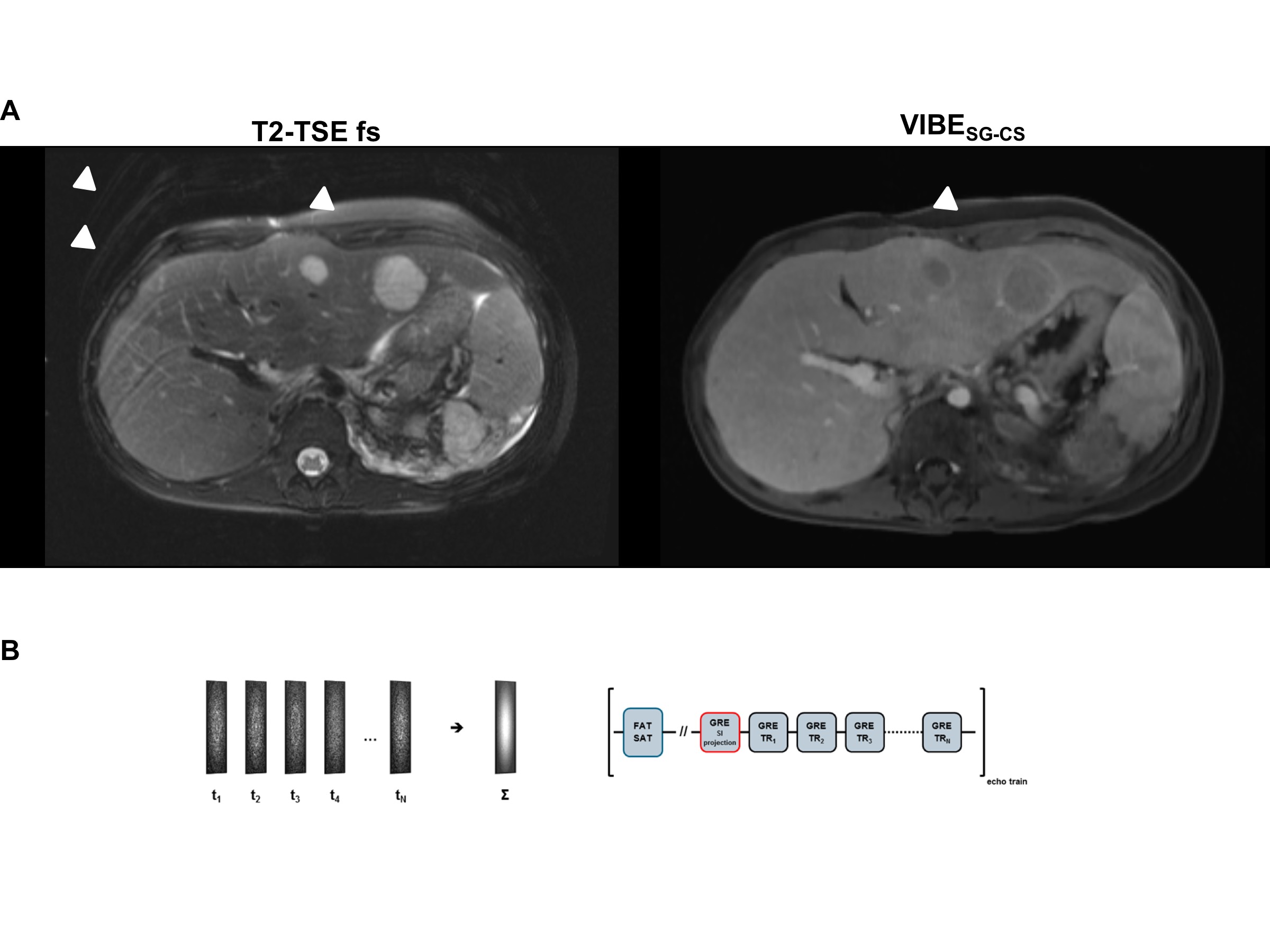
Fig. 1: Example of 16-year old patient with hepatic metastases of nephroblastoma.
(A) Motion and fat saturation robustness and superiority of free-breathing and self-gated 4D MRI with compressed sensing (VIBESG-CS) compared to T2-TSE fs sequence.
(B) Technical aspects of self-gated 4D MRI with compressed sensing. Left: Interleaved Cartesian sampling in the phase-encoding plane. Right: Echo trains following a fat suppression pulse include a readout module without phase encoding and with readout in SI direction, thereby allowing the extraction of motion information (self-gating).
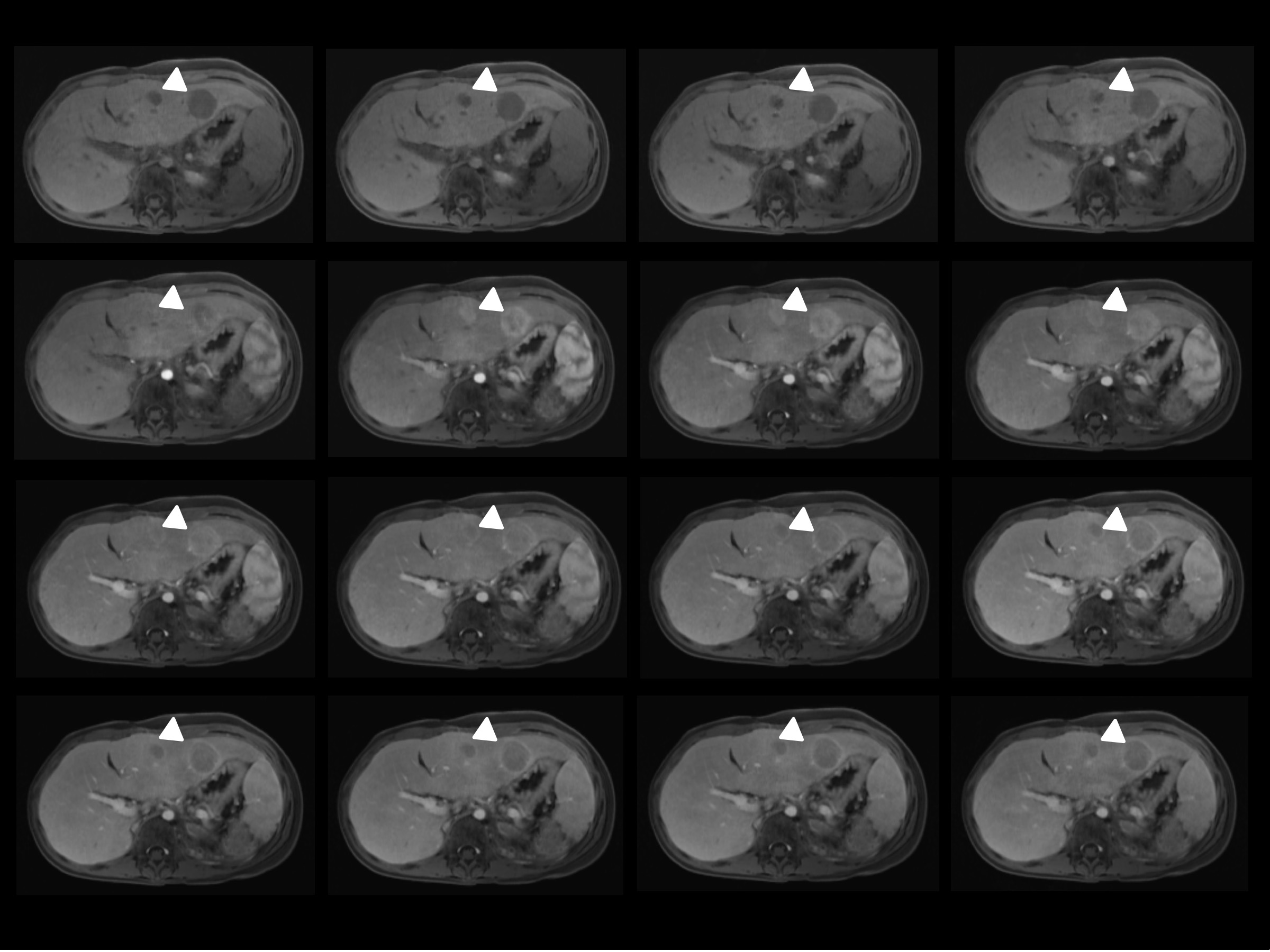
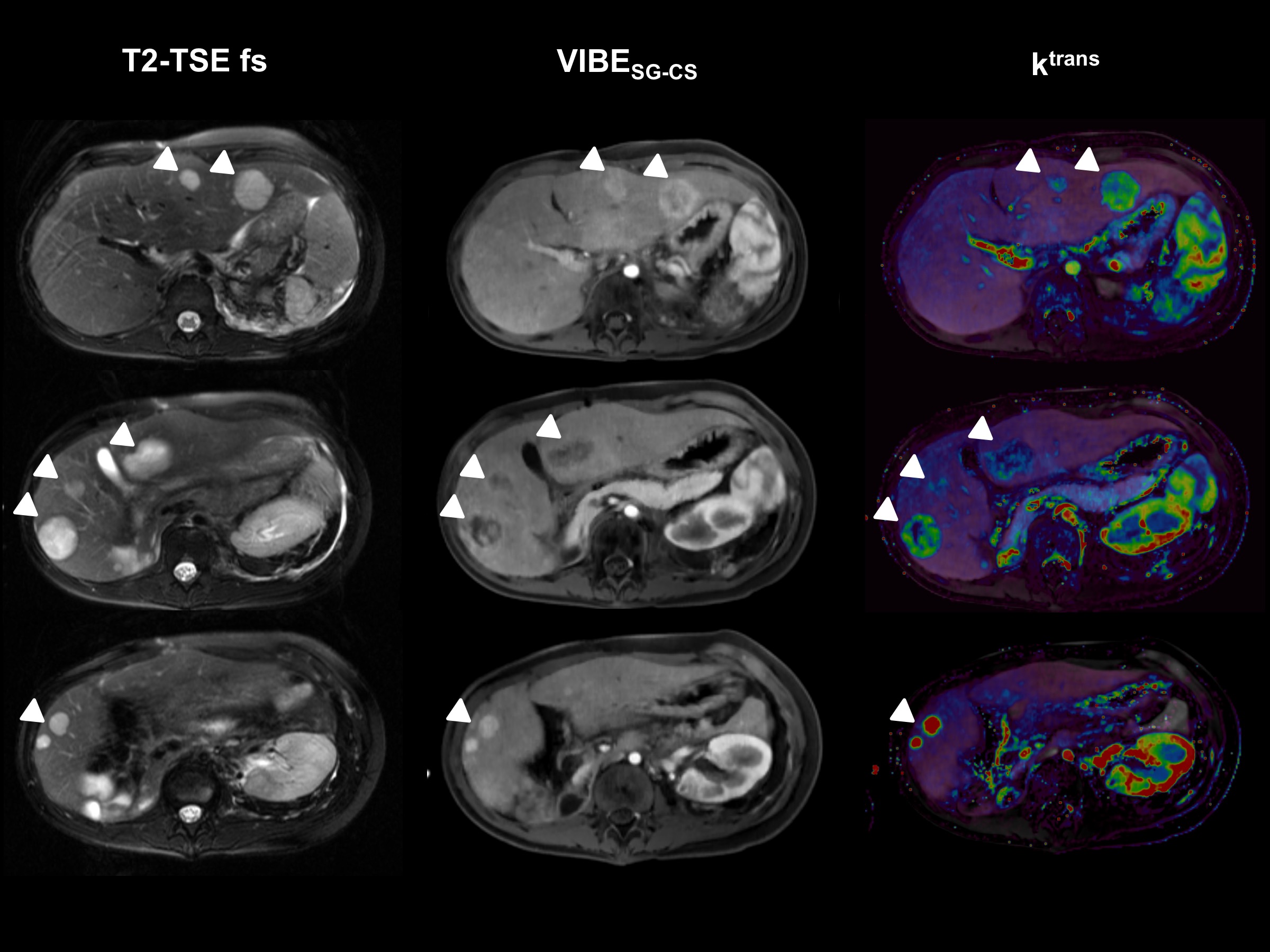
Fig. 3: Example of 16-year old patient with hepatic metastases of nephroblastoma.
Comparison of T2-TSE fs, free-breathing and self-gated 4D MRI with compressed sensing (VIBESG-CS) and calculated perfusion maps (Tofts model, ktrans). Perfusion maps show heterogeneous perfusion patterns of various metastastic lesions in contrast to homogeneous T2-hyperintense signal in T2-TSE fs sequence without variations.
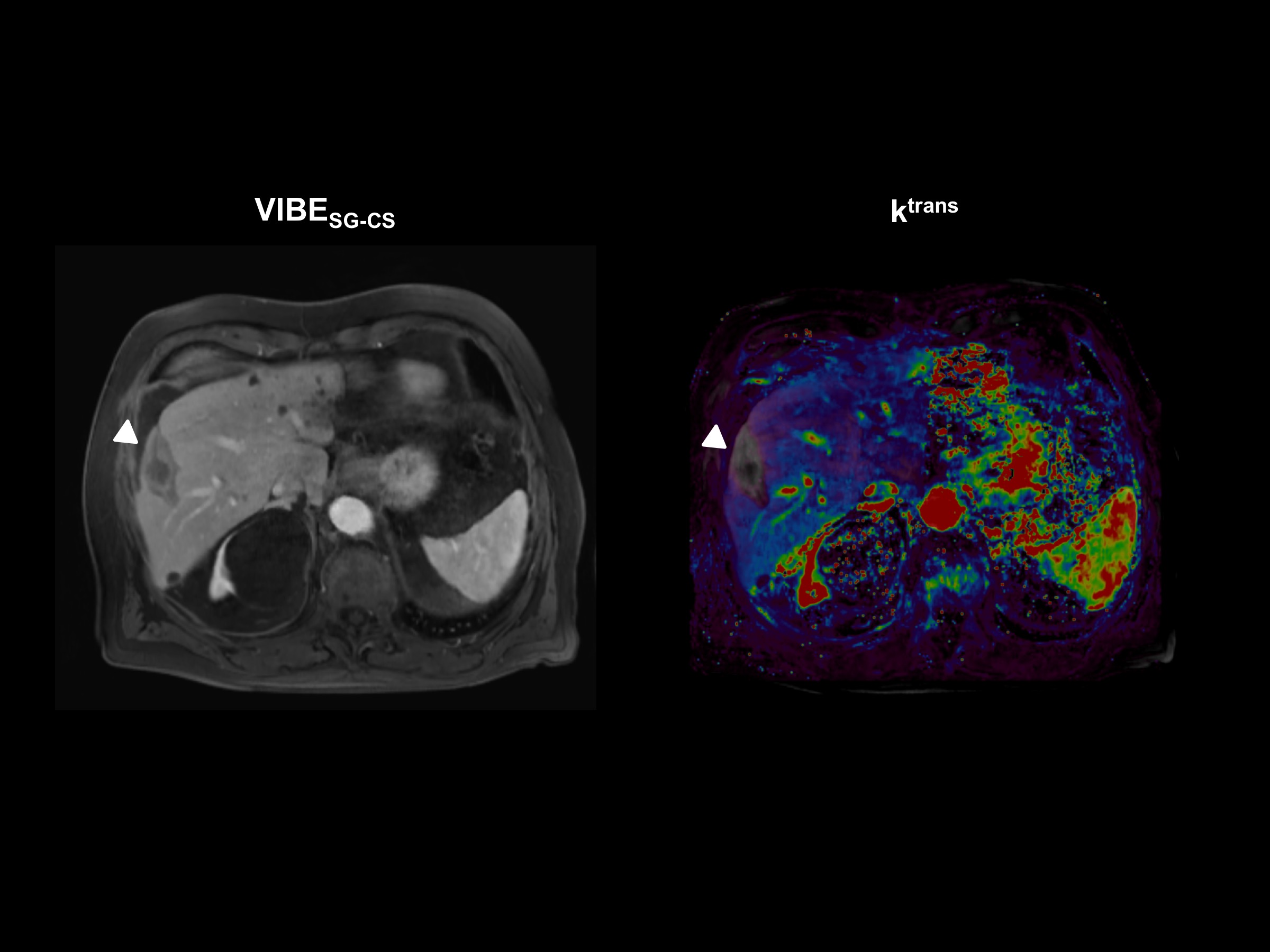
Fig. 4: Example showing 80-year old patient having undergone treatment of a single hepatic melanoma metastasis in liver segment V by using percutaneous radio-frequency ablation (RFA).
The ablated area shows a hyperintense rim demonstrating ablation limits. The calculated perfusion map (Tofts model, ktrans) shows no perfusion in the ablated area, indicating no recurrence of metastatic manifestation.
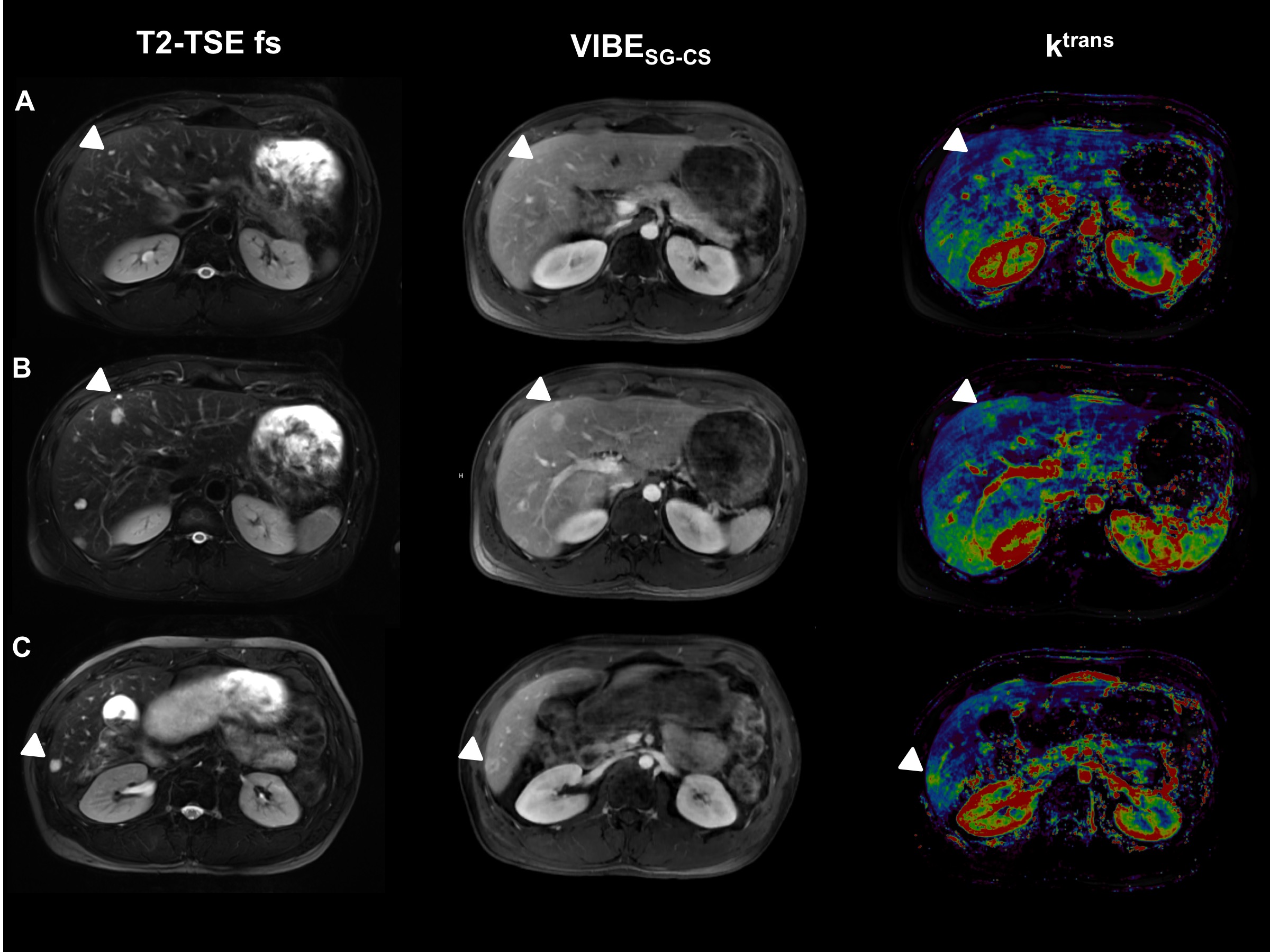
Fig. 5: Limitations of lesion detection by using perfusion analysis.
Example showing 36-year old patient with multiple liver metastases of neuroendocrine tumour (NET). Small metastatic lesions < 5 mm (A and B) are not clearly visible in perfusion maps (Tofts model, ktrans).