0552
Ungated myocardial perfusion imaging with complete left ventricular coverage using radial simultaneous multi-slice imaging1Radiology and Imaging Sciences, University of Utah, Salt lake city, UT, United States, 2Cardiology, University of Utah, Salt lake city, UT, United States
Synopsis
Myocardial perfusion imaging is a promising tool to determine the downstream effects of blocked coronary arteries. Ungated perfusion imaging is a promising alternative to conventional ECG-gated acquisitions. Existing ungated methods can acquire only 4-5 short-axis slices often with large slice gaps. Continuous and complete coverage is desired in order to avoid missed regions of perfusion deficit. Here we use an undersampled radial simultaneous multi-slice (SMS) acquisition to obtain complete coverage of the left ventricle. We use a block matching constrained reconstruction that is robust to inter-time frame cardiac and respiratory motion. We obtain 12 short axis slices in ~250 msec.
Purpose
To develop a rapid ungated cardiac perfusion acquisition with complete left ventricular coverage. CMR myocardial perfusion imaging is a useful tool to characterize coronary artery disease. Ungated perfusion imaging is a promising alternative to conventional ECG-gated acquisitions [1-3]. Ungated acquisitions ignore the ECG gating signal and continuously acquire data at a very high temporal sampling rate. Ungated acquisitions break the slice coverage vs temporal resolution dilemma especially in cases with poor ECG gating signal or in patients with atrial fibrillation where R-R interval is inconsistent. However, the high temporal sampling rate requirement (for example, four times a second) restricts the number of slices that can be acquired with an ungated acquisition. Existing methods with radial undersampling and advanced reconstructions can acquire 4-5 slices, which often have large slice gaps [2-5]. Continuous and complete coverage is desired to avoid missed regions of perfusion deficit. Here we extend a recently proposed undersampled radial simultaneous multi-slice (SMS) acquisition [6] to obtain significantly increased slice coverage for ungated perfusion acquisitions. We use a block matching constrained reconstruction that is robust to inter-time frame cardiac and respiratory motion. We obtain 12 short axis slices in ~250 msec allowing for an average sampling rate of four times a second.Methods
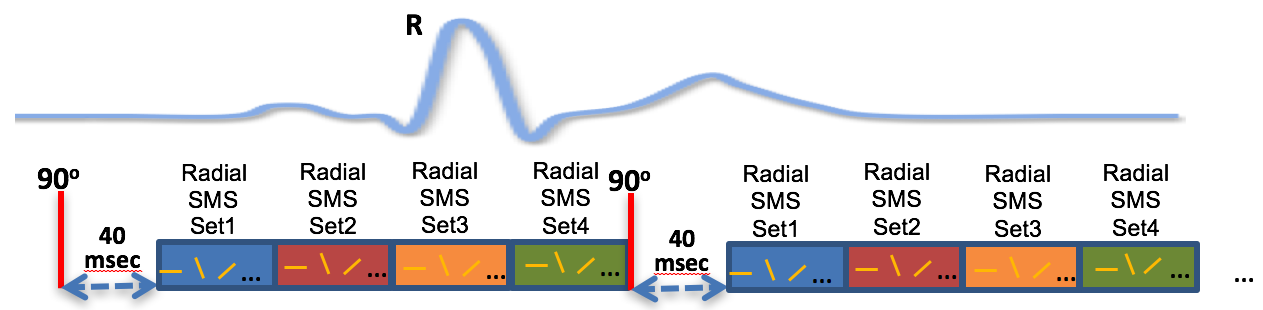
Ungated free-breathing myocardial perfusion imaging data was acquired in 3 subjects at rest. Imaging was performed on a 3T Siemens Prisma scanner using a body array coil with 24 channels. Scan parameters were TR=2.2 msec, TE=1.2 msec, FOV=260 mm2, slice thickness=8mm, number of slices=12. Acquisition matrix size was 144 x 24. A radial SMS sequence with a slice acceleration factor of three and golden ratio based angular spacing was used [6]. Phase modulation of the simultaneously excited slices was done in a CAIPIRINHA fashion [7]. Figure 1 shows a schematic of the ungated data acquisition. After a saturation pulse and a recovery time of 40 msec, 24 radial rays for each of the four SMS sets were acquired. Each SMS set corresponded to three short-axis slices. The process was repeated irrespective of the ECG-gating.
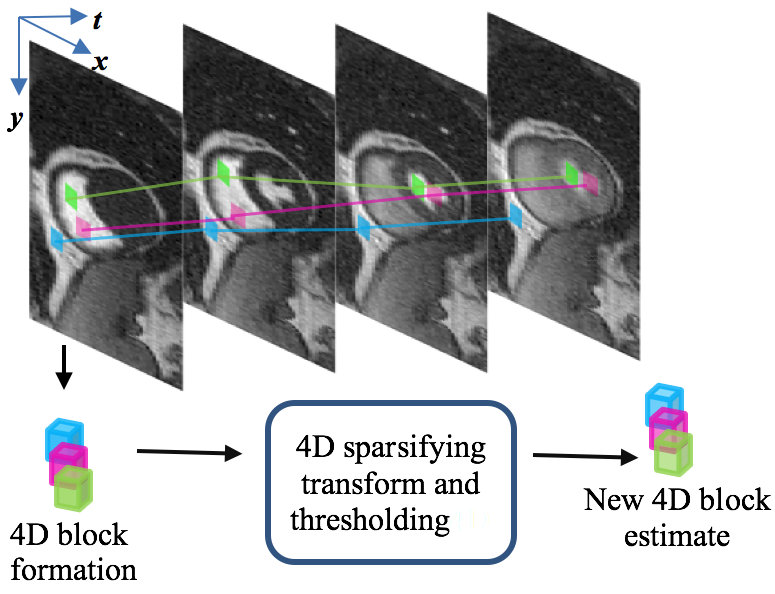
Undersampled radial SMS data was reconstructed using a 4-dimensional block matching constrained reconstruction. Matching 2D spatial blocks within and across time frames were first extracted to form a 3D block. Multiple such 3D blocks were grouped to form a 4D block. Separable sparsifying transforms were applied along the four dimensions and thresholding was done to obtain new image estimates. The idea of forming a 4D block is illustrated in Figure 2. Motion tracking of the 2D blocks across time frames was done by applying a smoothness constraint on the estimated motion vectors. The constraint effectively exploited non-local spatial and temporal redundancies and led to improved overall image quality as compared to local total variation (TV) constraints. A similar approach was used to produce state-of-the-art denoising results for natural videos [8].
Joint reconstruction of all simultaneously excited slices was performed in a POCS framework [6, 9, 10] alternating between applying the data fidelity constraint and the block matching filtering step. After a preliminary TV reconstruction of all time frames [6], acquired data was binned into near systole and diastole using the self-gating technique[1, 2]. Final block-matching constrained reconstruction was performed on data from each bin separately.
Results
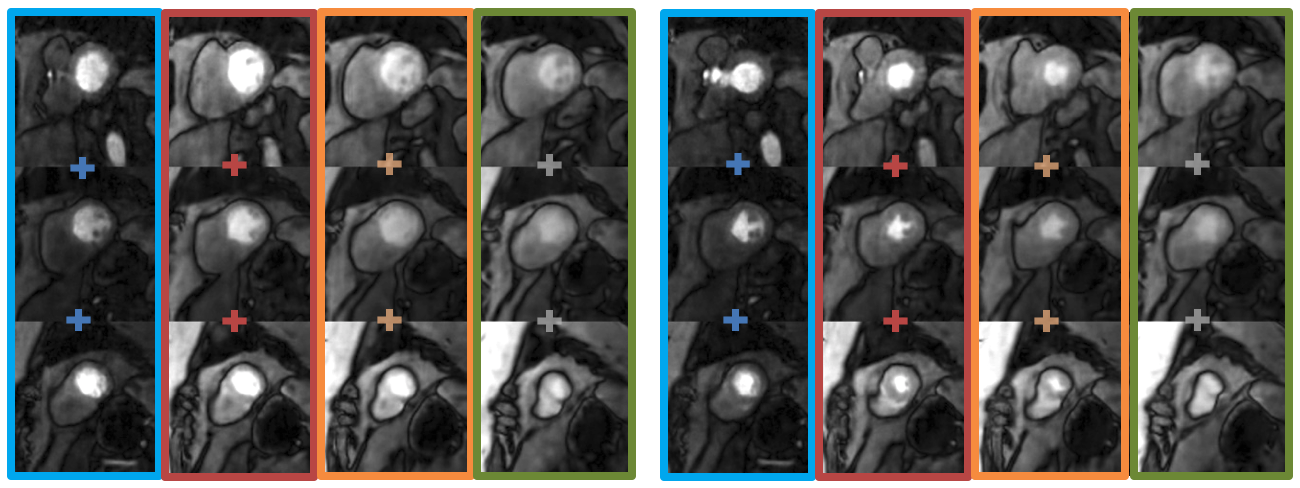
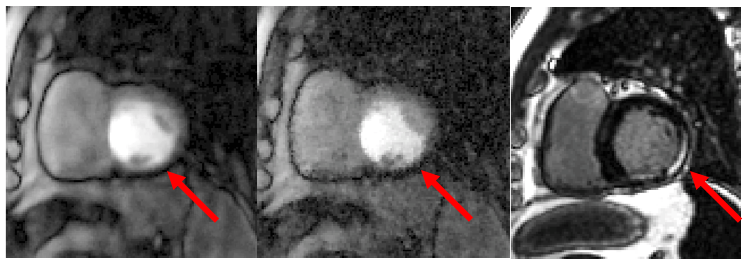
Figures 3 and 4 show the results of the ungated acquisition. One post-contrast time frame for all of the 12 slices at near systole and near diastole is shown in Figure 3. The plus signs between the images represent that they were acquired simultaneously. The color of each box encompassing the simultaneously acquired slices corresponds to the color of the SMS set shown in the schematic in Figure 1. Figure 4 shows results from a subject with myocardial infarction. A post-contrast time frame from one slice with a saturation recovery time of 40 msec at near systole is shown. The block matching reconstruction has improved delineation of the epicardial wall, the perfusion deficit region, and has less pixelation overall as compared to the TV reconstruction [6]. A late gadolinium enhancement image at a similar slice position confirms the region of infarction.
Conclusion
Undersampled radial SMS acquisition with a block matching constrained reconstruction allows for the acquisition of a short-axis slice in effectively ~21 msec including the delay time after the saturation pulse. The block matching constrained reconstruction gives good quality images even in the presence of large inter time frame motion. This approach is promising to obtain complete left ventricular coverage for ungated perfusion acquisitions and could be useful to accurately identify and quantify regions of perfusion deficit.
Acknowledgements
No acknowledgement found.References
[1] E.V.R. DiBella, L. Chen, M.C. Schabel, G. Adluru, C.J. McGann, Myocardial perfusion acquisition without magnetization preparation or gating, Magnetic Resonance in Medicine, 67 (2012) 609-613.
[2] A. Harrison, G. Adluru, K. Damal, A.M. Shaaban, B. Wilson, D. Kim, C. McGann, N.F. Marrouche, E.V. Dibella, Rapid ungated myocardial perfusion cardiovascular magnetic resonance: preliminary diagnostic accuracy, Journal of cardiovascular magnetic resonance : official journal of the Society for Cardiovascular Magnetic Resonance, 15 (2013) 26.
[3] B. Sharif, R. Dharmakumar, R. Arsanjani, L. Thomson, C.N. Bairey Merz, D.S. Berman, D. Li, Non–ECG-gated myocardial perfusion MRI using continuous magnetization-driven radial sampling, Magnetic Resonance in Medicine, 72 (2014) 1620-1628.
[4] D. Likhite, G. Adluru, N. Hu, C. McGann, E. DiBella, Quantification of myocardial perfusion with self-gated cardiovascular magnetic resonance, Journal of Cardiovascular Magnetic Resonance, 17 (2015) 1-15.
[5] D. Likhite, P. Suksaranjit, G. Adluru, N. Hu, C. Weng, E. Kholmovski, C. McGann, B. Wilson, E. DiBella, Interstudy repeatability of self-gated quantitative myocardial perfusion MRI, Journal of Magnetic Resonance Imaging, 43 (2016) 1369-1378.
[6] H. Wang, G. Adluru, L. Chen, E.G. Kholmovski, N.K. Bangerter, E.V.R. DiBella, Radial simultaneous multi-slice CAIPI for ungated myocardial perfusion, Magnetic resonance imaging, 34 (2016) 1329-1336.
[7] S.R. Yutzy, N. Seiberlich, J.L. Duerk, M.A. Griswold, Improvements in multislice parallel imaging using radial CAIPIRINHA, Magnetic Resonance in Medicine, 65 (2011) 1630-1637.
[8] M. Maggioni, G. Boracchi, A. Foi, K. Egiazarian, Video Denoising, Deblocking, and Enhancement Through Separable 4-D Nonlocal Spatiotemporal Transforms, Image Processing, IEEE Transactions on, 21 (2012) 3952-3966.
[9] A.A. Samsonov, E.G. Kholmovski, D.L. Parker, C.R. Johnson, POCSENSE: POCS-based reconstruction for sensitivity encoded magnetic resonance imaging, Magnetic Resonance in Medicine, 52 (2004) 1397-1406.
[10] M. Maggioni, V. Katkovnik, K. Egiazarian, A. Foi, Nonlocal Transform-Domain Filter for Volumetric Data Denoising and Reconstruction, Image Processing, IEEE Transactions on, 22 (2013) 119-133.
Figures