0539
Feasibility of Synthetic MRI of the spine – fast and quantitative imaging1Geneva University Hospitals, Geneva, Switzerland
Synopsis
Synthetic MRI was already validated in some cerebral applications. We adapted it to evaluate the spine and showed that it produces, in general, good image quality and diagnostic confidence. Efforts will still have to be made to increase image quality in the dorso-lumbar spine. However, the non-negligible time saving and the ability to obtain quantitative measurements as well as to generate several contrasts with a single acquisition should secure an interesting and useful future for synthetic MRI in clinical routine.
Introduction
Synthetic MR is a method that produces multiple contrasts as well as quantitative T1, T2 and PD images and that has already been validated in cerebral applications1,2. The goal of this study was to implement synthetic MR in the spine and to evaluate its diagnostic confidence compared to conventional sequences.Material and methods
Thirty-one patients underwent MRI for spine examination (cervical, lumbar or whole spine) on a Philips Ingenia 1.5T. Conventional T1 TSE, T2 TSE and STIR TSE sequences were performed as well as the syntac sequence. The syntac sequence is based on a TSE sequence with a saturation pulse (120°), 4 different inversion times and 2 echo times, which leads to 8 images with different contrasts. These images are then used by SyMRI v8 software (SyntheticMR AB, Linköping, Sweden) to generate T1, T2 and PD quantitative images and then synthetically create T1, T2 and STIR contrasts with user chosen TE/TR/TI. Sequence parameters were: sagittal orientation, FOV 200x321 mm, acquisition (reconstruction) voxel size 0.89x1.48 (0.71x0.72) mm, 15 slices of 4 mm thickness with no gap, TE 11 / 100 ms, TR 2485 ms, TSE factor 12, SENSE acceleration factor 2. The acquisition time of the synthetic sequence is 5min 40sec. Synthetic images were generated with matching TE/TR parameters and compared to the conventional sequences (T1, T2, STIR when available). The TI was chosen to suppress as much as possible the signal from fat. For each patient, two sets of images were created (conventional and synthetic sequences). Random analysis of the sets was performed by a blinded neuroradiologist who graded the image quality (non-diagnostic, medium, good), the presence of artifacts and identified the different pathologies.Results
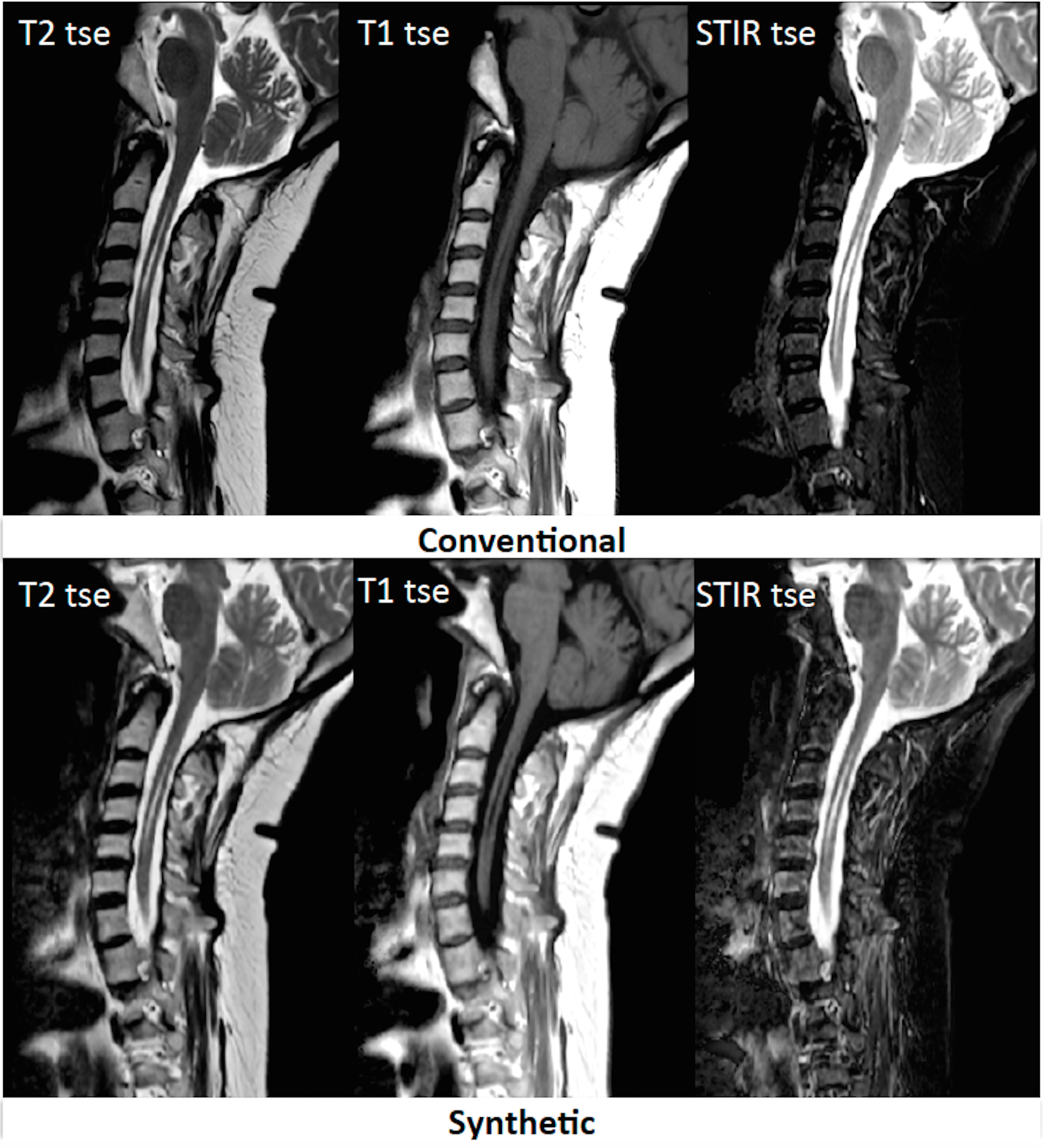
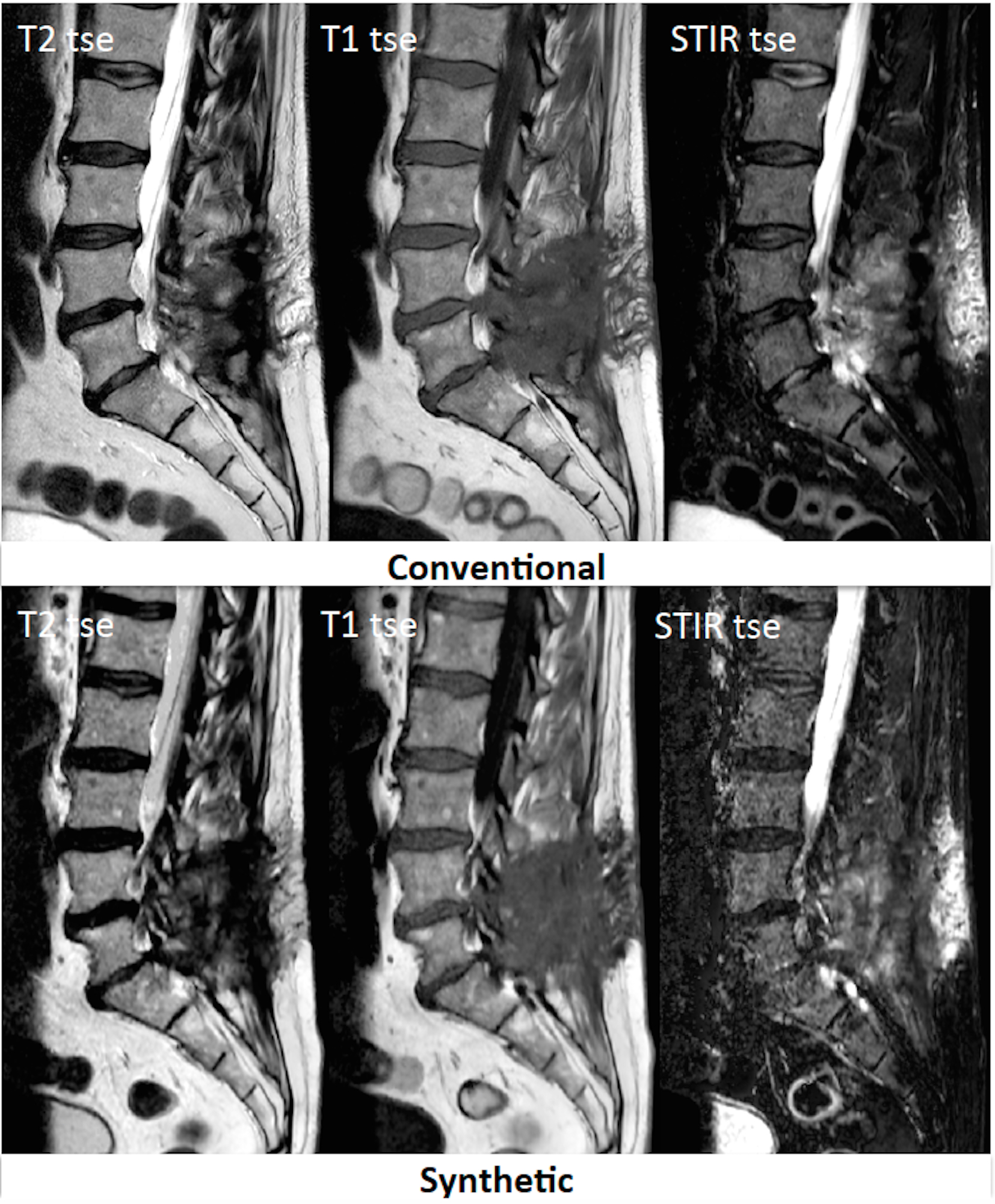
All synthetic images were graded as medium (6.5%) to good quality (93.5%), none was rated as non-diagnostic quality. Conventional images were all graded as good quality. The diagnosis was concordant in 87.1% of cases, which means the lesion was identified with the same confidence in Synthetic as in conventional images. Figure 1 shows an example of a syrinx that is clearly visible in synthetic images. The diagnosis was discordant in 3.2% (1/31) and uncertain in 9.7% (3/31) of cases. Concerning the presence of artifacts, a majority (84%) of synthetic STIR presented flow artifacts and / or noise compared to conventional images. In addition, 19.4% of T1 and T2 images demonstrated either flow artifacts or a noisy appearance. In general, the images were perceived as of better quality with a higher signal to noise ratio (SNR) in the cervical region due to the presence of the head-neck coil compared to dorsal or lumbar regions. Figure 2 shows an example of synthetic images in postoperative evaluation of the lumbar spine.Discussion
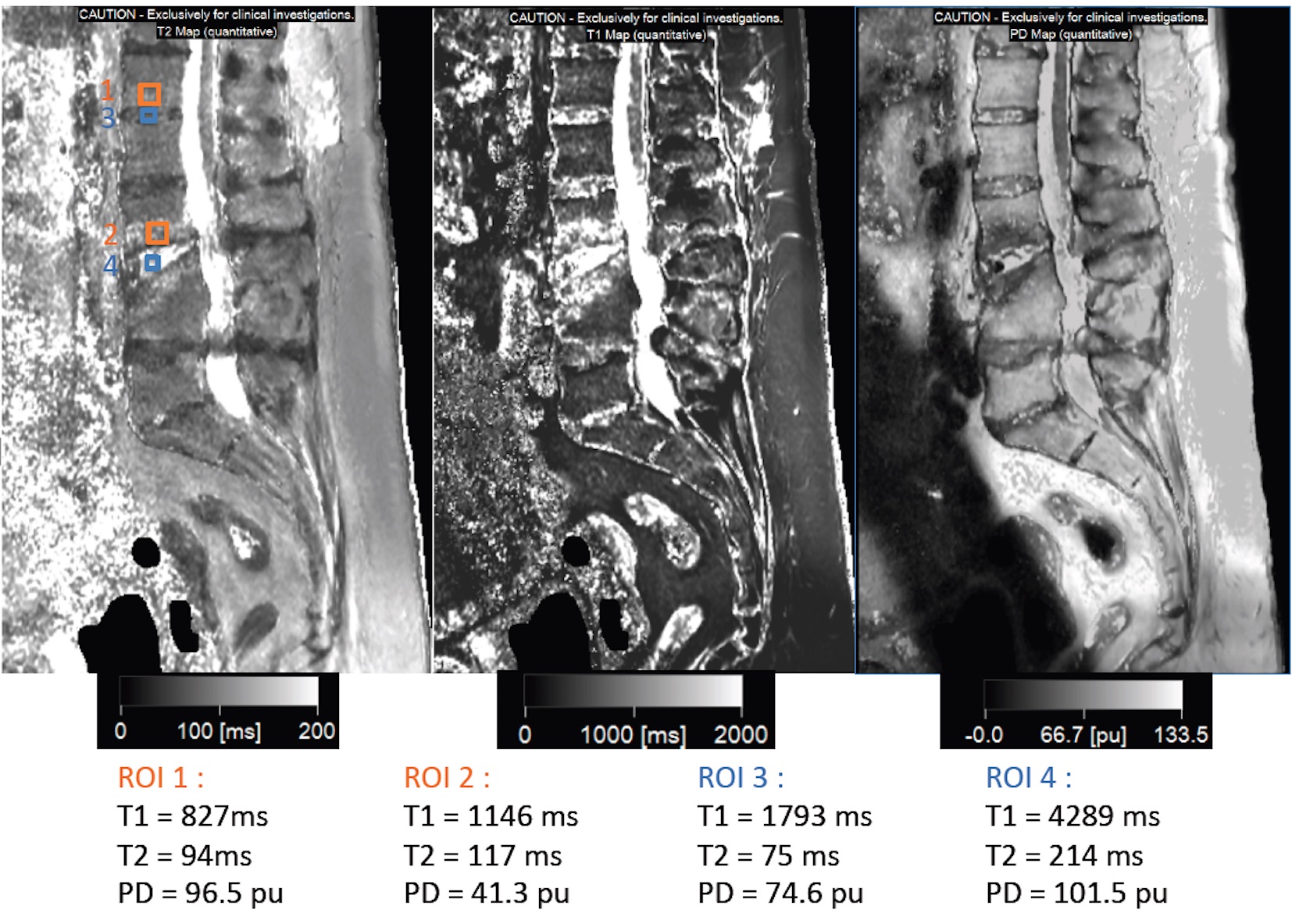
The syntac sequence was adapted to evaluate the spine and can replace at least 3 conventional sequences (T1, T2, STIR), that usually require 13min 30sec of acquisition time, and offers the possibility to generate other contrasts if required. The main current limitations of this sequence are a certain degree of SNR reduction in the dorso-lumbar spine and the presence of vascular flow artifacts, particularly in STIR images. In the cases where the diagnosis was not concordant, the images were affected by artifacts. A compromise still has to be found to increase the SNR while maintaining a reasonable acquisition time in the dorso-lumbar spine. However, in our study the image quality and diagnostic confidence are still very good, especially in the cervical region where the syntac sequence currently produces the best results. It also allows the generation of quantitative T1, T2 and PD images (Figure 3), which are of great interest since they are expected to produce more accurate and relevant results as suggested by a recent publication of the European society of radiology3. The next step of this study is to evaluate the added value of quantitative T1/T2 measurements in the interpretation of the lesions. We believe that our findings can help in the integration of quantitative MRI in clinical routine, notably in the context of development of new methods such as fingerprinting.Conclusion
Our study shows that Synthetic MRI is feasible for spinal imaging and produces, in general, good image quality and diagnostic confidence. Efforts will still have to be made to increase image quality in the dorso-lumbar spine. However, the non-negligible time saving and the ability to obtain quantitative measurements as well as to generate several contrasts with a single acquisition should secure an interesting future for synthetic MRI in clinical routine.Acknowledgements
No acknowledgement found.References
1. Blystad I, Warntjes JB, Smedby O, et al. Synthetic MRI of the brain in a clinical setting. Acta Radiol. 2012 Dec 1;53(10):1158-63.
2. Granberg, T, Uppman, M, Hashim, F, et al. Clinical Feasibility of Synthetic MRI in Multiple Sclerosis: A Diagnostic and Volumetric Validation Study. American Journal of Neuroradiology, 2016 ; 1–7.
3. European Society of Radiology (ESR). Magnetic Resonance Fingerprinting - a promising new approach to obtain standardized imaging biomarkers from MRI. Insights into Imaging, 2015, 6(2), 163–165.
Figures