0525
3D Whole-Heart Phase Sensitive Inversion Recovery (PSIR) for Simultaneous Bright Blood Coronary Angiography and Black Blood Late Gadolinium Enhancement (LGE)1Division of Imaging Sciences and Biomedical Engineering, King’s College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom
Synopsis
This study introduces a free-breathing 3D whole-heart sequence with image-based navigation for post-contrast phase sensitive inversion recovery (PSIR) allowing for simultaneous bright-blood coronary angiography and black-blood late gadolinium enhancement (LGE) imaging. Such approach was successfully tested in a cohort of 10 patients with cardiovascular disease. Data acquisition was performed in free-breathing with 100% scan efficiency, thus allowing for predictable scan time. The proposed sequence allowed for LGE visualization with high volumetric coverage and improved contrast (black-blood dataset) while simultaneously providing sharp visualization of the coronary arteries and heart anatomy (bright-blood dataset).
Introduction
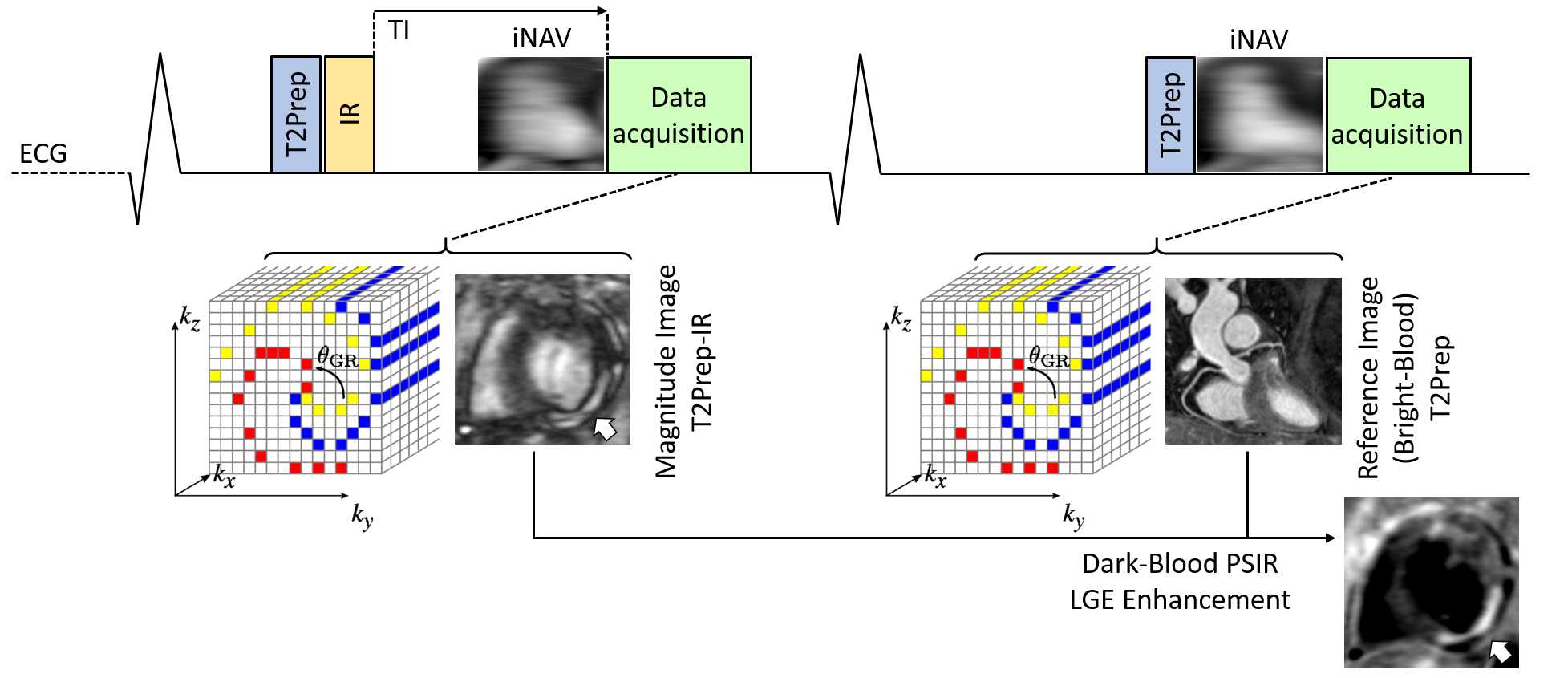
Late gadolinium enhancement (LGE) imaging allows for the assessment of various pathological conditions including myocardial infarction and myocarditis. Phase Sensitive Inversion Recovery (PSIR) applied to LGE imaging1 provides intrinsic robustness with respect to the choice of the inversion time (TI) when compared to inversion-recovery (IR) sequences with magnitude reconstruction. Conventional PSIR acquisitions are segmented over two consecutive heartbeats: in the first heartbeat, a T1-weighted image is acquired after the application of a non-selective IR pulse, while a low flip-angle reference image is acquired in the second heartbeat. The T1-weighted image and the reference image are then combined as described in1. As conventional PSIR might suffer from poor contrast between the enhanced tissue and adjacent blood pool, the use of a T2prep in combination with the IR pulse has been proposed2. Most of the LGE PSIR implementations are limited to 2D acquisitions and performed during a breath-hold to minimize respiratory motion artefacts. Here, we introduce a free-breathing 3D whole-heart PSIR sequence with image-based navigation3, which uses a T2Prep-IR module for black-blood LGE imaging, allowing for volumetric coverage and visualization of scar tissue with improved contrast. Furthermore, the acquisition of the reference volume is performed at higher flip-angle and it is preceded by a T2prep (Fig1). Therefore, the proposed framework provides a 3D whole-heart, black-blood PSIR volume for the detection of LGE, enables the acquisition of a complimentary bright-blood volume for the visualization of heart anatomy and coronary lumen (T2prep dataset), and ensures 100% scan efficiency and predictable scan time.Methods
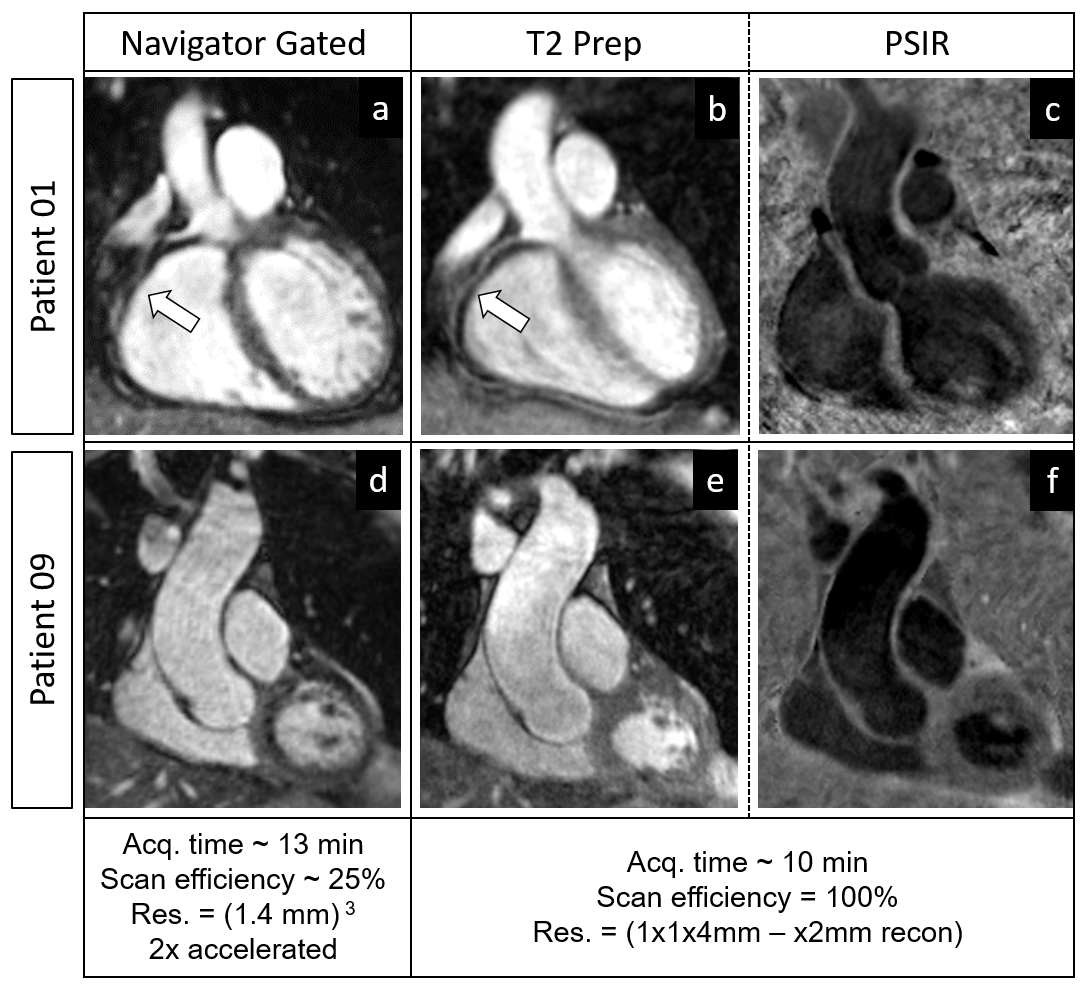
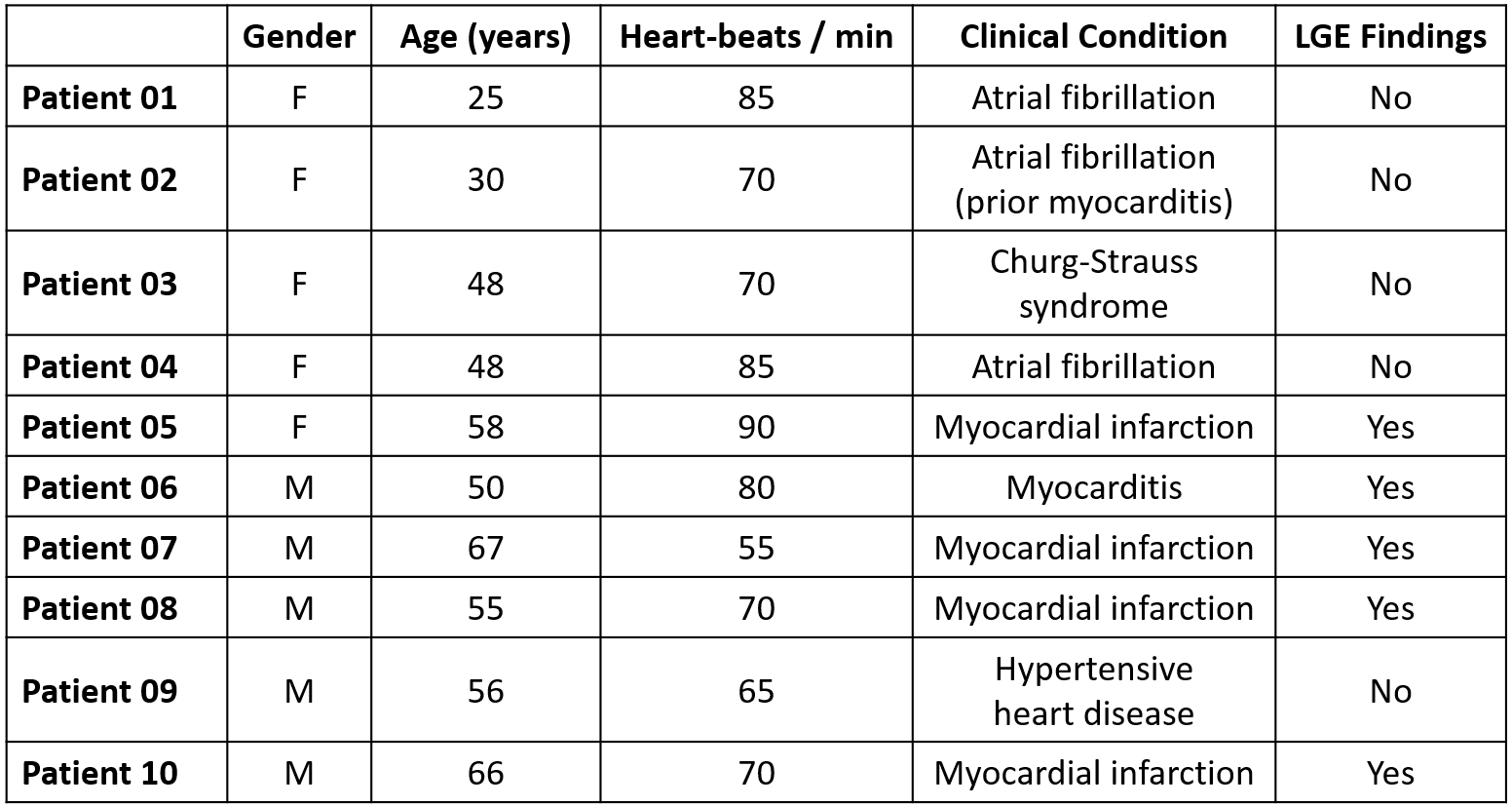
Sequence implementation: A whole-heart, ECG-triggered, bSSFP, Cartesian prototype sequence with spiral profile order4 was implemented and adapted to perform PSIR-like acquisitions as in Fig1. A low-resolution 2D image navigator (iNAV) is acquired in each heart beat to allow motion estimation and correction3. Data acquisition was performed on a 1.5T system (Siemens MAGNETOM Aera) in 10 patients (Table1) with cardiovascular disease (CVD). The clinical routine included the acquisition of a conventional, multi-slice and multi-breath hold, 2D-PSIR LGE sequence (resolution:1x1.5x8mm). In 2 individual cases, a conventional post-contrast whole-heart, diaphragmatic navigator-gated sequence was prescribed for clinical purposes (resolution: 1.4x1.4x1.4mm3, 5mm respiratory acceptance window). The 2D-PSIR LGE clinical sequence was acquired ~8 minutes after contrast injection (Gadobutrol, 0.02mmol/kg). Subsequently (~15-20 minutes after contrast injection) the proposed sequence was acquired with the following imaging parameters: 1x1x4mm resolution (reconstructed to 1x1x2mm), FOV 320x320x160-260mm, coronal orientation, TR/TE 3.6ms-1.56ms, flip-angle 90deg, fat-saturation, TI 90-250ms (selected after a dedicated TI scout-scan), T2Prep duration 40ms, data acquisition time ~10-14min in free-breathing. Image reconstruction: Translational motion along the superior-inferior and left-right direction was estimated and compensated for using the iNAVs that preceded the 3D bSSFP sequence. The two datasets (T2Prep-IR and T2Prep) were motion corrected separately and then co-registered before PSIR reconstruction. Data analysis: Coronary vessel length (VL) and percentage vessel sharpness (%VS) were computed in the T2Prep datasets before and after motion correction5. SNR of blood and CNR blood/myocardium were quantified in the motion corrected T2Prep dataset.Results
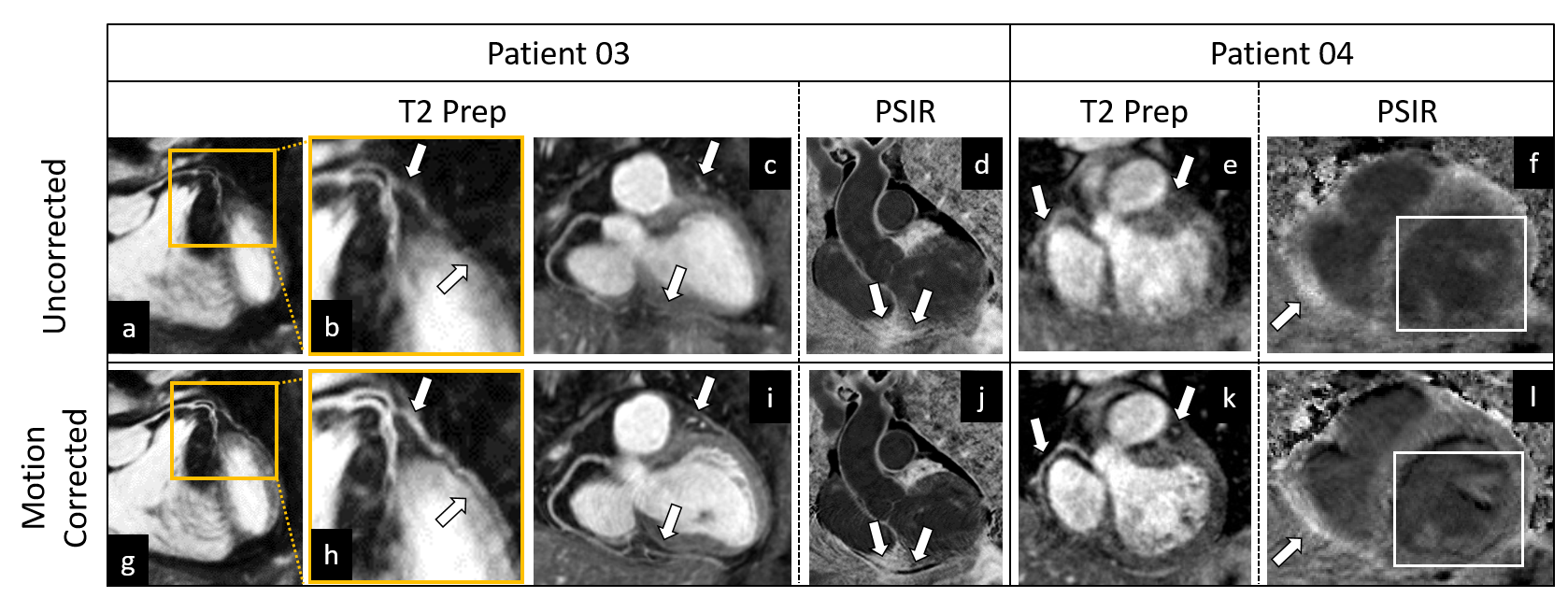
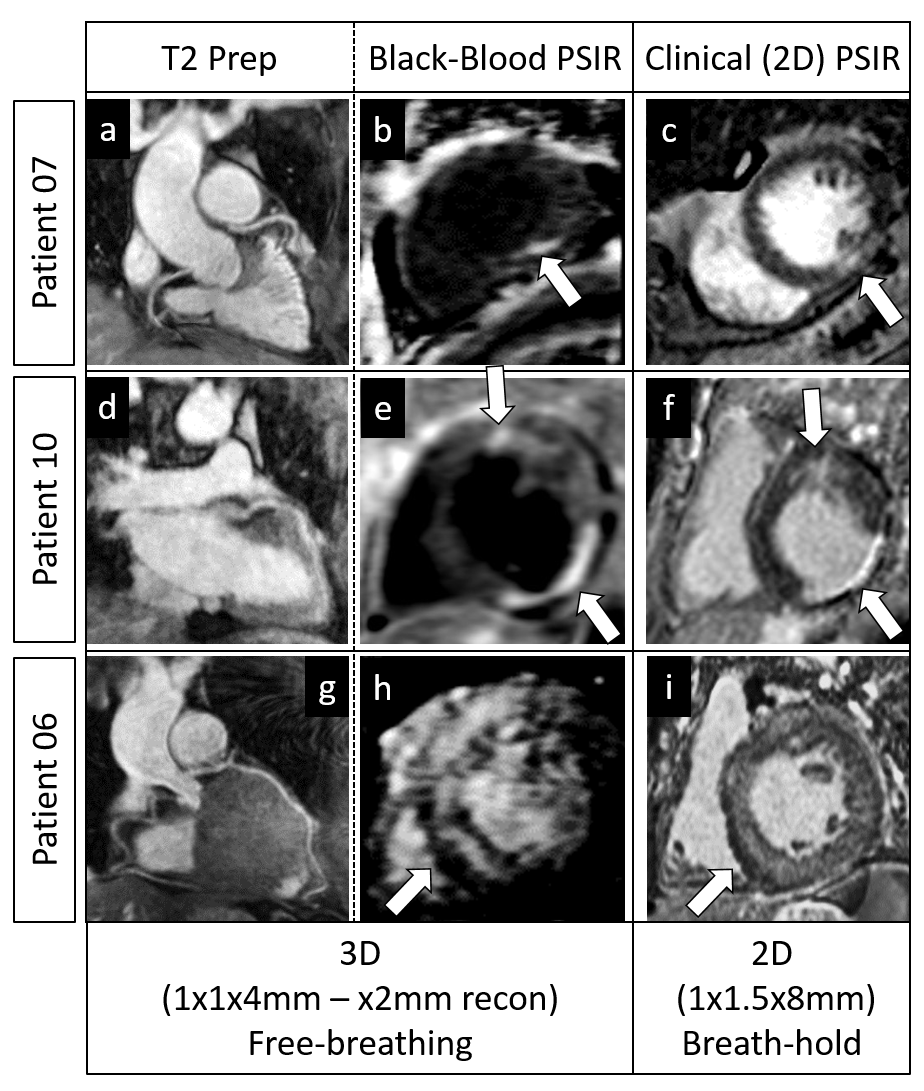
Translational motion correction showed effectiveness in reducing blurring artefacts in both the T2Prep (bright-blood heart anatomy and coronary lumen visualization) and the black-blood (LGE) datasets (Fig2). In particular, improved coronary depiction can be appreciated in the T2Prep datasets after motion correction. Quantitative analysis also confirmed the efficacy of motion correction (uncorrected vs motion corrected: VL-LAD; 3.6±3.4cm vs 6.8±3.9cm, VL-RCA; 2.3±3.2cm vs 7.3±6.8cm, %VS-LAD; 17.8±14.3% vs 30.3±8.5, %VS-RCA; 16.5±15.2 vs 27.2±13.7, all P<0.05). Quantified SNR of blood: 21.9±3.2, CNR blood/myocardium: 11.7±2.1. Image quality of the T2prep dataset (2nd heartbeat) was similar to that of the diaphragmatic navigator-gated acquisition (Fig3). Furthermore, the 3D dark-blood dataset obtained from the PSIR reconstruction enabled high contrast and well-delineated depiction of myocardial scar and was in good agreement with the clinical 2D-PSIR sequence (Fig4). The suppression of blood signal provided with the proposed approach lead to improved contrast between scar tissue and the adjacent blood pool in several cases (Fig4) when compared to the clinical 2D-PSIR images.Conclusions
A free-breathing 3D whole-heart motion corrected post-contrast PSIR sequence for simultaneous bright-blood and black-blood imaging has been introduced and successfully tested in 10 patients with CVD. The proposed sequence enables not only the identification of scar tissue (black-blood LGE) but it also provides a bright-blood dataset for whole heart anatomy and coronary MR angiography. This is achieved at no extra scan time and at 100% scan efficiency (shorter and predictable scan time). Future work will include the use of an accelerated non-rigid respiratory motion correction framework6 to achieve higher spatial resolution and account for more complex respiratory motion.Acknowledgements
This work was supported by EPSRC EP/N009258/1, EP/P001009/1, EP/P007619/1 and MRC MR/L009676/1.References
1) Kellman P, et al. Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magn Reson Med 2002; 47(2): 372-83.
2) Kellman P, et al. Dark blood Late Gadolinium Enhancement improves conspicuity of ablation lesions. Journal of Cardiovascular Magnetic Resonance 2016; 18(Suppl 1):P211 DOI: 10.1186/1532-429X-18-S1-P211.
3) Henningsson M, et al. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med 2012; 67: 437-45.
4) Prieto C, et al. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J. Magn. Reson. Imaging 2015; 41: 738-46.
5) Etienne A, et al. “Soap-Bubble”: Visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magn Reson Med 2002; 48:658-66.
6) Cruz G, et al. Highly efficient non rigid motion-corrected 3D whole heart coronary vessel wall imaging. Magn Reson Med 2016; DOI: 10.1002/mrm.26274.
Figures