0424
Reproducibility and Accuracy of 4D Flow Valve Tracking for Assessment of Mitral Regurgitation1Cardiology, UCSF, San Francisco, CA, United States, 2Department of Radiology and Biomedical Imaging, UCSF, San Francisco, CA, United States
Synopsis
Quantification of mitral regurgitation (MR) is challenging to accurately perform with echocardiography.1 Recent data suggest that MRI is more accurate than echocardiography, but the conventional approach used requires the combination of data from two different types of MRI sequences.2 This study investigated the direct measurement of mitral regurgitation with 4D Flow using a valve tracking approach. We used both mitral annulus tracking and mitral flow jet tracking, and compared measurements to the conventional MRI approach for calculating mitral regurgitation. Flow jet but not annulus tracking demonstrated good reproducibility of measurement and correlation with the conventional MRI approach.
Introduction
Quantification of mitral regurgitation (MR) can guide the optimal timing of valve replacement, but is challenging to accurately and reliably perform with echocardiography.1 MRI has been suggested to be a more accurate approach, using the combination of volumetric steady-state free procession (SSFP) and ascending aortic phase contrast data to calculate mitral regurgitation as the difference between left ventricular (LV) stroke volume and aortic forward flow (conventional MRI approach).2 This study investigated the direct measurement of mitral regurgitation with 4D Flow using a valve tracking approach. We aimed to evaluate the reproducibility of both mitral annulus tracking and mitral flow jet tracking, and to compare measurements to the conventional MRI approach.Methods
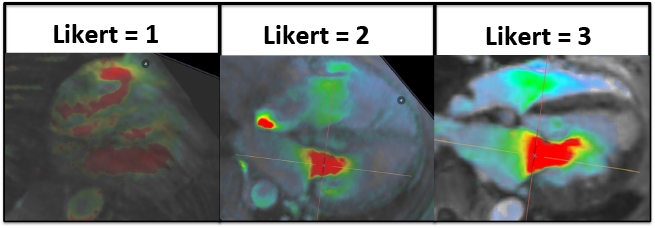
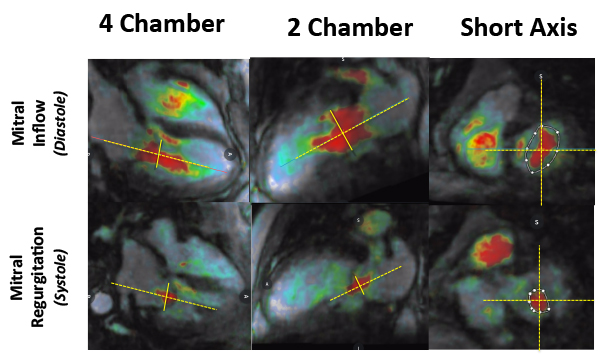
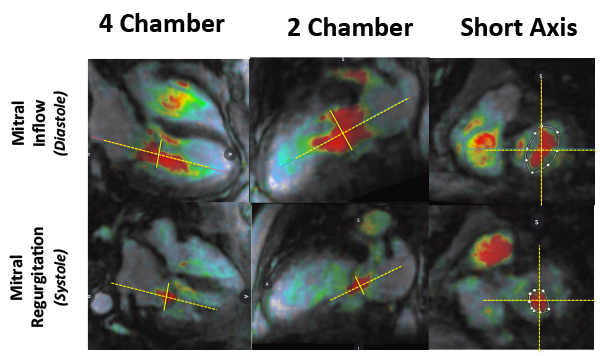
Adult patients (n=21, 14 males, 64+/-16 years) referred for clinically indicated CMR in sinus rhythm were prospectively and consecutively recruited for 4D Flow imaging performed after standard protocol for their primary diagnosis. The sequence and software visualization platform used has previous been described3. 4D Flow image quality was assessed with a 3-point Likert scale based on artifact severity (1=poor flow signal; 2=partially distorted flow signal; 3=flow signal visible throughout the cardiac cycle) (Figure 1). Likert score ≥ 2 was considered acceptable image quality for inclusion. Two methods of valve tracking were performed: 1) annulus tracking where the quantification of mitral flow was performed on a plane that tracked with the valve annulus throughout the cardiac cycle (Figure 2); and 2) flow jet tracking where the quantification plane was placed perpendicular to forward and reverse flow jets across the mitral valve (Figure 3). Reproducibility analysis with intra-class correlation (ICC) was performed on independent measurements of forward flow, reverse flow, and regurgitant fraction (RF) using both 4D flow valve tracking approaches performed by two blinded operators. A subset of patients (n=11, 5 males, 64+/-14 years) underwent conventional MRI assessment of mitral regurgitation: 1) LV stroke volume (LVSV) from volumetric SSFP; 2) aortic forward flow (AoFF) from 2D phase contrast; and 3) calculation of mitral regurgitation using the formula (LVSV-AoFF)/LVSV. For these patients, the 4D Flow-derived data and conventional MRI calculation of mitral regurgitation was compared.Results
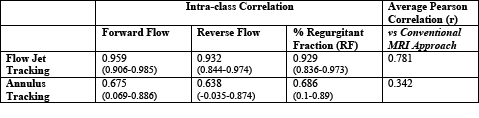
A total of 16 patients (11 males, 65 +/-15 years) with a mean Likert score of 2.3+/=0.6 were included in the study; 5 patients were excluded due to flow artifact (motion=4, mitral annular ring=1). Flow jet tracking demonstrated excellent reproducibility: ICC forward flow=0.959 (0.906-0.985); ICC reverse flow=0.932 (0.844-0.974); ICC RF=0.929 (0.836-0.973). Annulus tracking was less reproducible: ICC forward flow=0.675 (0.069-0.886); ICC reverse flow=0.638 (-0.035-0.874); ICC RF=0.686 (0.1-0.89). Mitral regurgitation severity by conventional MRI was as follows: mild (n=5), mild to moderate (n=2), and moderate-severe (n=4) with a %RF of 29+/-22. Flow jet tracking exhibited stronger correlation with the conventional MRI calculation of mitral regurgitant fraction than annulus tracking (average Pearson correlation coefficient (r) of 0.34 versus 0.78).Discussion
Flow jet tracking is a reproducible and accurate means of performing mitral valve tracking to calculate mitral regurgitation from 4D Flow data. Annulus tracking is a previously reported approach for this calculation, but is both less reproducible and less accurate.4 As MRI evolves as a clinical imaging option for the management of mitral regurgitation, flow jet tracking using 4D Flow data should be further studied as a direct means of quantifying mitral flow. While we have shown good correlation between this approach and the conventional MRI approach, larger studies that include correlation with surgical outcomes are needed to demonstrate the clinical value of 4D Flow in this context.Conclusions
Flow jet tracking is the preferred 4D Flow approach for determining mitral regurgitation fraction, exhibiting good reproducibility and strong correlation with the conventional MRI measurement.Acknowledgements
The authors would like to thank Christopher B. Williams (technologist) and Benjamin Mow (chief technologist) for their technical guidance and steadfast support.References
1. Biner, S. et al. Reproducibility of proximal isovelocity surface area, vena contracta, and regurgitant jet area for assessment of mitral regurgitation severity. JACC. 2010. 3(3): 235-243.
2. Uretsky, S. et al. Discordance between echocardiography and MRI in the assessment of mitral regurgitation severity. A prospective multicenter trial. JACC. 2015. 65(11): 1078-88.
3. Hanneman, K. et al. Assessment of the precision and reproducibility of ventricular volume, function, and mass measurements with ferumoxytol-enhanced 4D flow MRI. J Magn Reson Imaging. 2016. 44(2): 383-92.
4. Westenberg J. Mitral valve and tricuspid valve blood flow: accurate quantification with 3D velocity-encoded MR imaging with retrospective valve tracking. Radiology. 2008. 249(3): 792-800.
Figures