0396
Association of vascular risk factors with cerebral metabolic rate1Huntington Medical Research Institutes, Pasadena, CA, United States, 2Advanced Imaging Research Center, UT Southwestern Medical Center, Dallas, TX, United States, 3Radiology, Johns Hopkins University School of Medicine, Baltimore, MD, 4Radiology, UT Southwestern Medical Center, Dallas, TX, 5Geriatrics, UT Southwestern Medical Center, Dallas, TX, United States, 6Radiology, Internal Medicine, UT Southwestern Medical Center, Dallas, TX, United States, 7Radiology, UT Southwestern Medical Center, Dallas, TX, United States, 8Radiology, Johns Hopkins University School of Medicine, Baltimore, MD, United States
Synopsis
Vascular risk factors that confer a susceptibility for dementia are thought to result in silent brain changes decades before disease onset. We hypothesized that vascular risk factors would be associated decreased Cerebral Metabolic Rate of Oxygen consumption (CMRO2). CMRO2 was derived from Arterial Spin Labelling cerebral blood flow (CBF) and oxygen extraction fraction (OEF) from TRUST MRI in this IRB approved study with informed consent on 70 participants. In stepwise linear regression higher diastolic blood pressure was correlated with decreased CMRO2 but was not associated with CBF, suggesting mechanisms other than insufficient blood flow underlie the association with metabolic rate.
Purpose
Cerebral metabolic rate of oxygen consumption (CMRO2) is an index of neural activity which is decreased in cognitive impairment.1 Vascular risk factors confer a susceptibility for dementia and may result in brain changes decades before disease onset.2 We hypothesized that vascular risk factors would be associated with differences in CMRO2. Secondary analysis evaluated the link between vascular risk factors and MRI cerebral blood flow (CBF) and oxygen extraction fraction (OEF) which were used to derive CMRO2.Methods
In this IRB approved study with informed consent, 3T brain MRI (Achieva, Philips Medical Systems, The Netherlands) was obtained on 70 participants from a community based cohort 6 years after vascular risk assessment. Systolic and diastolic blood pressure (mmHg) were measured by an automated oscillometric device with reported value the mean of the 3rd-5th recordings. The following risk factors were binary indicator variables operationalized as the presence or absence of the condition (with “absence of the condition” being the reference group). Elevated serum triglycerides (fasting triglycerides ≥150 mg/dL or treatment) and low serum HDL (Men <40 mg/dL and Women <50 mg/dL or treatment) were calculated according to National Institutes of Health Cholesterol Education Program ATP III Guidelines.3 Diabetes mellitus was defined by either self-report accompanied by use of anti-hyperglycemic medication; or by elevated serum glucose (fasting > 126 mg/dL [7.0 mmol/L]; or by non-fasting glucose > 200 mg/dL [11.1 mmol/L]).4
Our MRI technique for measuring CMRO2 has been previously described5,6 and is based on the Fick principle of arteriovenous oxygen difference: CMRO2= CBF × (Ya – Yv) × Ca 7 where CBF is total cerebral blood flow adjusted for brain volume with units of ml/100g/min, Ya−Yv gives the difference in % oxygen saturation between the arterial input and venous outflow and Ca is the oxygen carrying capacity of blood. Yv was determined using a validated MRI technique of T2 Relaxation Under Spin Tagging (TRUST).8,9 A stepwise linear regression model using Akaike information criterion was performed to identify the optimal predictive model.
Results
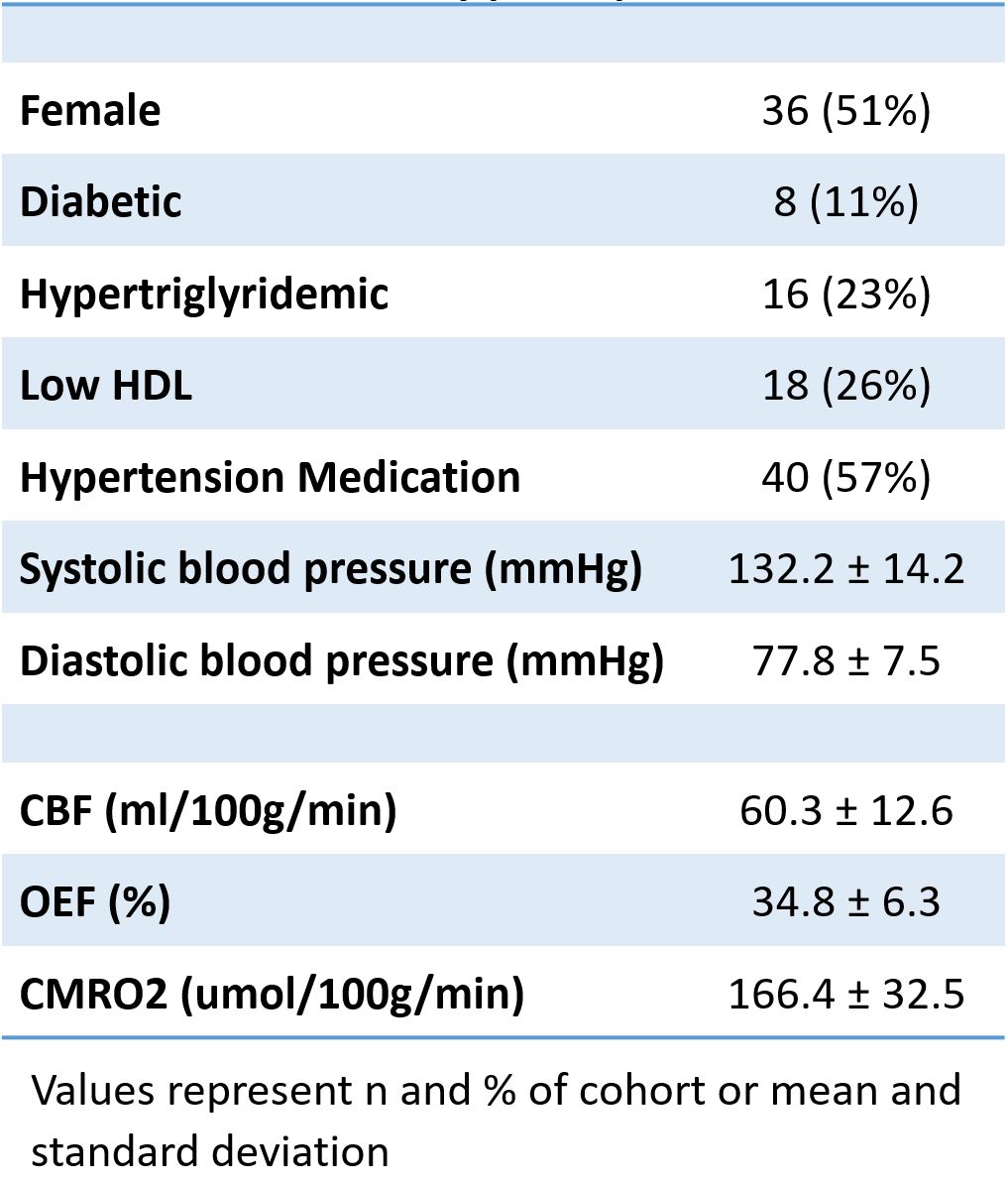
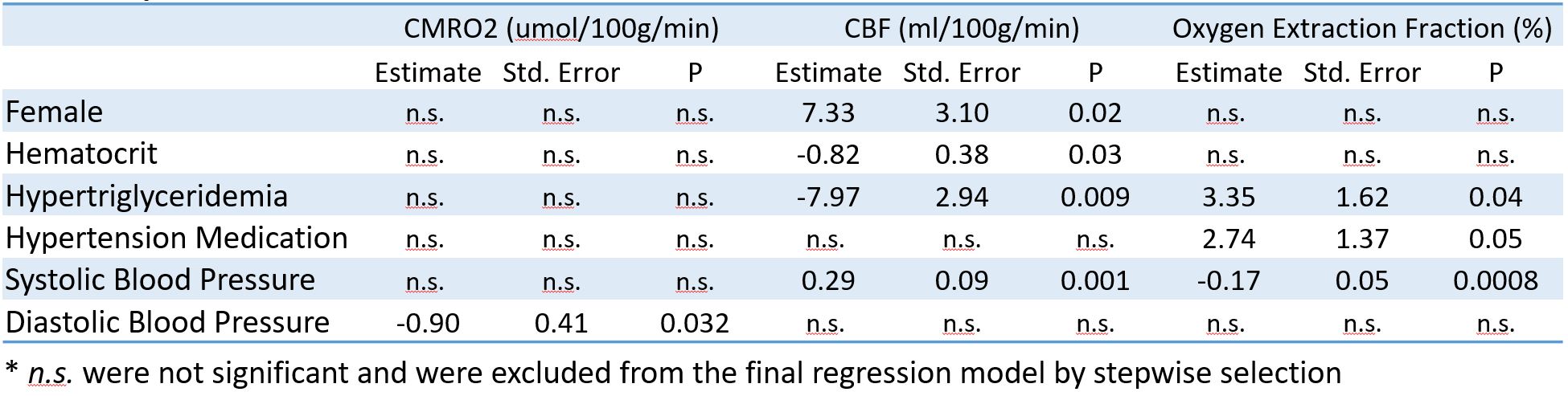
At vascular risk assessment participants were 61.2 ± 5 years of age and at MRI age was 67.5 ± 5.1 years. Additional characteristics of study participants used in linear regression modelling are given in Table 1. Results of stepwise linear regression are shown in Table 2.Discussion
Higher diastolic blood pressure correlated with decreased CMRO2 suggesting that diastolic hypertension may be associated with decreased brain metabolism. Surprisingly, diastolic blood pressure was not associated with differences in CBF, suggesting other mechanisms are involved in its association with metabolic rate. CBF was significantly associated with other factors that did not correlate with CMRO2 suggesting they are related by vascular mechanisms. Systolic blood pressure was associated with greater CBF which may indicate that cerebral autoregulation did not adequately increase resistance to maintain constant flow. This may expose the microvasculature to excess pulsatility, leading to microvascular disease and potential for impaired blood flow in the future10. Hypertriglyceridemia was associated with lower CBF which may be related to increased microvascular disease or to elevated blood viscosity.11 Hypertriglyceridemia was also associated with greater OEF which preserved CMRO2 but may confer a susceptibility for ischemic insult by lowering reserves as lower oxygen pressures in the tissues are needed for greater extraction from the blood. Age, diabetes and low HDL did not significantly contribute to prediction of any of our outcome imaging measures. The age range of our sample was relatively narrow, which may likely account for this lack of association with age.Conclusion
This study suggests that diastolic blood pressure may play a unique role in the cerebral metabolic rate compared to other vascular risk factors. Vascular risk factors had distinct associations between CMRO2, CBF and OEF. This supports the importance of evaluating both metabolic rate and cerebral blood flow to assess the impact of vascular risk factors on the brain.Acknowledgements
Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health" under award Number UL1TR001105. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.References
1. Thomas BP, Sheng M, Tseng BY, et al. Reduced global brain metabolism but maintained vascular function in amnestic mild cognitive impairment. J Cereb Blood Flow Metab 2016.
2. Kloppenborg RP, van den Berg E, Kappelle LJ, Biessels GJ. Diabetes and other vascular risk factors for dementia: which factor matters most? A systematic review. Eur J Pharmacol 2008;585(1):97-108.
3. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001;285(19):2486-2497.
4. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997;20(7):1183-1197.
5. Xu F, Ge Y, Lu H. Noninvasive quantification of whole-brain cerebral metabolic rate of oxygen (CMRO2) by MRI. Magn Reson Med 2009;62(1):141-148.
6. Liu P, Xu F, Lu H. Test-retest reproducibility of a rapid method to measure brain oxygen metabolism. Magn Reson Med 2013;69(3):675-681.
7. Kety SS, Schmidt CF. Measurement of cerebral blood flow and cerebral oxygen consumption in man. Fed Proc 1946;5:264.
8. Lu H, Ge Y. Quantitative evaluation of oxygenation in venous vessels using T2-Relaxation-Under-Spin-Tagging MRI. Magn Reson Med 2008;60(2):357-363.
9. Lu H, Xu F, Grgac K, Liu P, Qin Q, van Zijl P. Calibration and validation of TRUST MRI for the estimation of cerebral blood oxygenation. Magn Reson Med 2012;67(1):42-49.
10. Mitchell GF, van Buchem MA, Sigurdsson S, et al. Arterial stiffness, pressure and flow pulsatility and brain structure and function: the Age, Gene/Environment Susceptibility - Reykjavik Study. Brain 2011;134(Pt 11):3398-3407.
11. Rosenson RS, Shott S, Tangney CC. Hypertriglyceridemia is associated with an elevated blood viscosity Rosenson: triglycerides and blood viscosity. Atherosclerosis 2002;161(2):433-439.
Figures