0383
Multi-Contrast EPI for use as a Neuro MR Scout and ScreeningMathias Engström1, Enrico Avventi2,3, Ola Norbeck2,3, Henric Rydén2,3, and Stefan Skare2,3
1Applied Science Laboratory, GE Healthcare, Uppsala, Sweden, 2Dept. of Neuroradiology, Karolinska University Hospital, Stockholm, Sweden, 3Dept. of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden
Synopsis
This work describes a new sub-minute EPI-based sequence that produce T2*, T2, T2-FLAIR, T1-FLAIR, DWI, and ADC images as well as a 3-plane localizer as an alternative to the conventional scout, enabling a clinical screening at the beginning of the exam.
Purpose
The long examination times in MRI calls for reducing the number of image series in the clinical routine. When the patient medical history is well known, the number of image series can be reduced and prioritized. This reduces the risk for motion artifacts, and, if the patient wants to abort the examination early due to e.g. pain or claustrophobia, the radiologist may still be able to answer the question. By contrast, when the cause of the patient’s symptom is unclear, scan order and necessary series is less obvious, which may result in long examination times. In this work we propose a new sub-minute EPI-based sequence that produce T2*, T2, T2-FLAIR, T1-FLAIR, DWI, and ADC images in addition to a 3-plane localizer as a starting point for the examination.Methods
The sequence was built as a collection of sequence modules that can be played out in any order, one being the EPI readout and the rest performing various magnetization preparations, prepended to the EPI readout module during the scan process as shown in Fig. 1 to produce the desired contrasts. Volunteer scans were performed on a 3T system (DV750, GE Healthcare, Milwaukee, WI) and patient scans on a 1.5T system (DV450, GE Healthcare, Milwaukee, WI) using an 8-channel (Invivo Hi-Res Head Coil, Gainesville, FL) and 32-channel receive coil (Nova Medical, Wilmington, MA). The study was approved by the local ethics committee and informed consent was given. Relevant scan parameters included: FOV=240×240 mm, matrix=144×144 and 180×180, R=2/3 (8-ch/32-ch), slice thickness=5 mm and 30 slices over the brain. The inversion time for T2-FLAIR was TR dependent, set to null T1 species of 4500 ms (CSF). The TE was 130 ms for T2-FLAIR. During the deadtime following each IR pulse in the T2-FLAIR, a GE-EPI sequence played out on another slice using TE=40 ms and FA of 20° with a negated RF excitation pulse added after to minimize spin-history effects. Hence, in less than 15 s, T2* and T2-FLAIR data was obtained. The scan then continues to acquire two b0 (i.e. T2-w) and three orthogonal diffusion directions (b=1000 s/mm2). The second b0 set was acquired with negated EPI blips to allow for the geometric distortions for all data. The first b0 data was acquired in R shots (i.e. fully sampled) to enable entropy driven Nyquist ghost correction1 and parallel imaging calibration. For the DW data, TE was 70 ms and TR=3400 ms. Following the diffusion section, ~20 seconds, the sequence continued to acquire T1-FLAIR EPI data with a yet shorter TR. The TI for the T1-FLAIR was 700 ms. To eliminate dead-time due to this TI, the inversion block was only 10 ms long, but played out 11 slices ahead of the T1-FLAIR EPI read-out. All EPI readouts used an ETL of 144/R2=72 or 180/R3=60. For the last section in the scan (used to produce three orthogonal, distortion free, scout images) the Spectral-Spatial RF pulse was replaced with a conventional RF excitation SLR pulse followed by a single-lobe EPI readout. Using ETL=1 and sequential slice ordering (ax/sag/cor) the 3-plane scout was acquired in about 4 seconds. The total scan time was 52 seconds. Image reconstruction was performed using MATLAB (The MathWorks Inc., Natick, MA), followed by distortion correction using TOPUP2,3 and 3D rigid body motion correction based on mutual information (SPM, FIL, London, UK).Results
The effect of the distortion correction can be seen in Fig. 2 where Fig. 2a is the blip-up data, Fig. 2b the blip-down and Fig. 2c the final distortion corrected image. All reconstructed contrasts, including 3-plane scout, are presented in Fig. 3. Fig. 4 shows data acquired at a higher resolution. Fig. 5 a comparison to standard clinical data at 1.5T.Discussion/Conclusion
By combining the scan efficiency of the EPI readout with a modularized way of doing magnetization-preparation we demonstrate that it is possible to acquire a radiological baseline set with full brain coverage consisting of 6 image contrasts plus a distortion free 3-plane scout under a minute. This could replace the conventional scout, in order to choose and prioritise series based on where lesions are found on the multi-contrast EPI data. In addition to this informative scout application, the sub-minute multi-contrast scan may for some patient groups be sufficient as a screening method that could replace some CT scans in an acute clinical care setting. Moreover, by spending an additional 1-2 minutes, each MR contrast can be acquired in also sagittal and coronal planes, leading to about 20 or more image series in about three minutes of total scan time.Acknowledgements
No acknowledgement found.References
[1] Skare S, et al., In: Proceedings of the 14th Annual Meeting of ISMRM, Seattle (2006). p. 2349[2] Anderson et al., NeuroImag (2003) 20:870-88[3] Smith et al., NeuroImag (2004) 23:208-19Figures
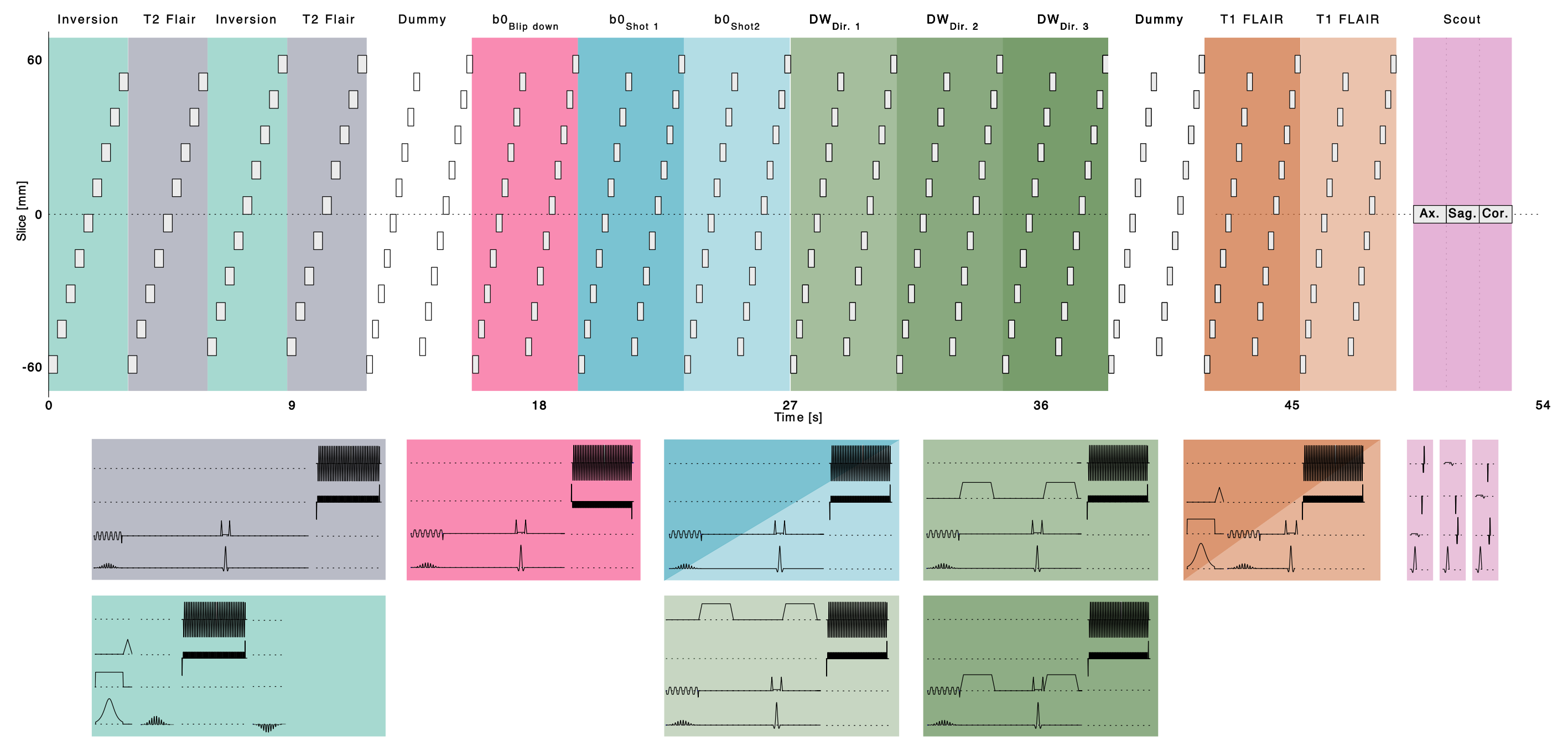
Figure 1. Schematic representation of the multi-contrast EPI acquisition. The color coded blocks represent the different modules used, which in turn are created by freely combining from a set of psd building blocks (e.g. EPI readout, inversion, SpSp excitation, Spin-Echo excitation, Diffusion preparation).
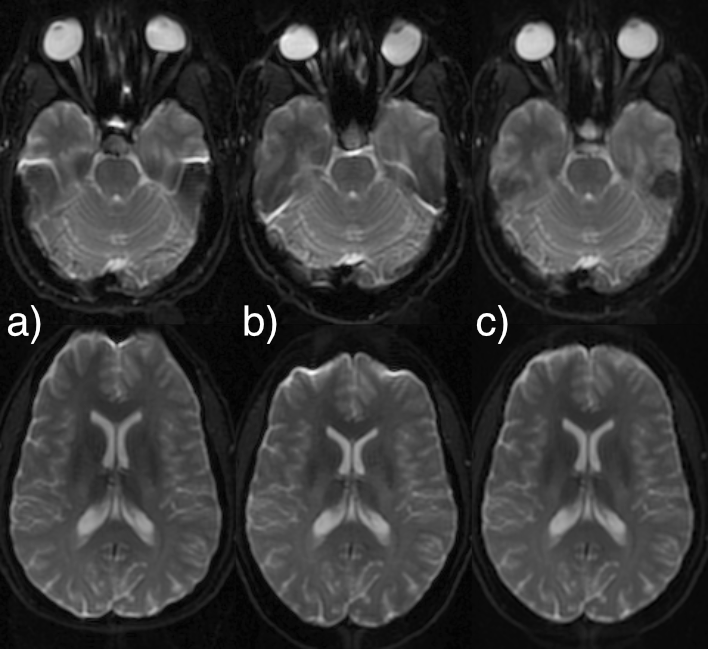
Figure 2. b0 data with a) blip-up, b) blip-down, and c) the resulting distortion corrected image.
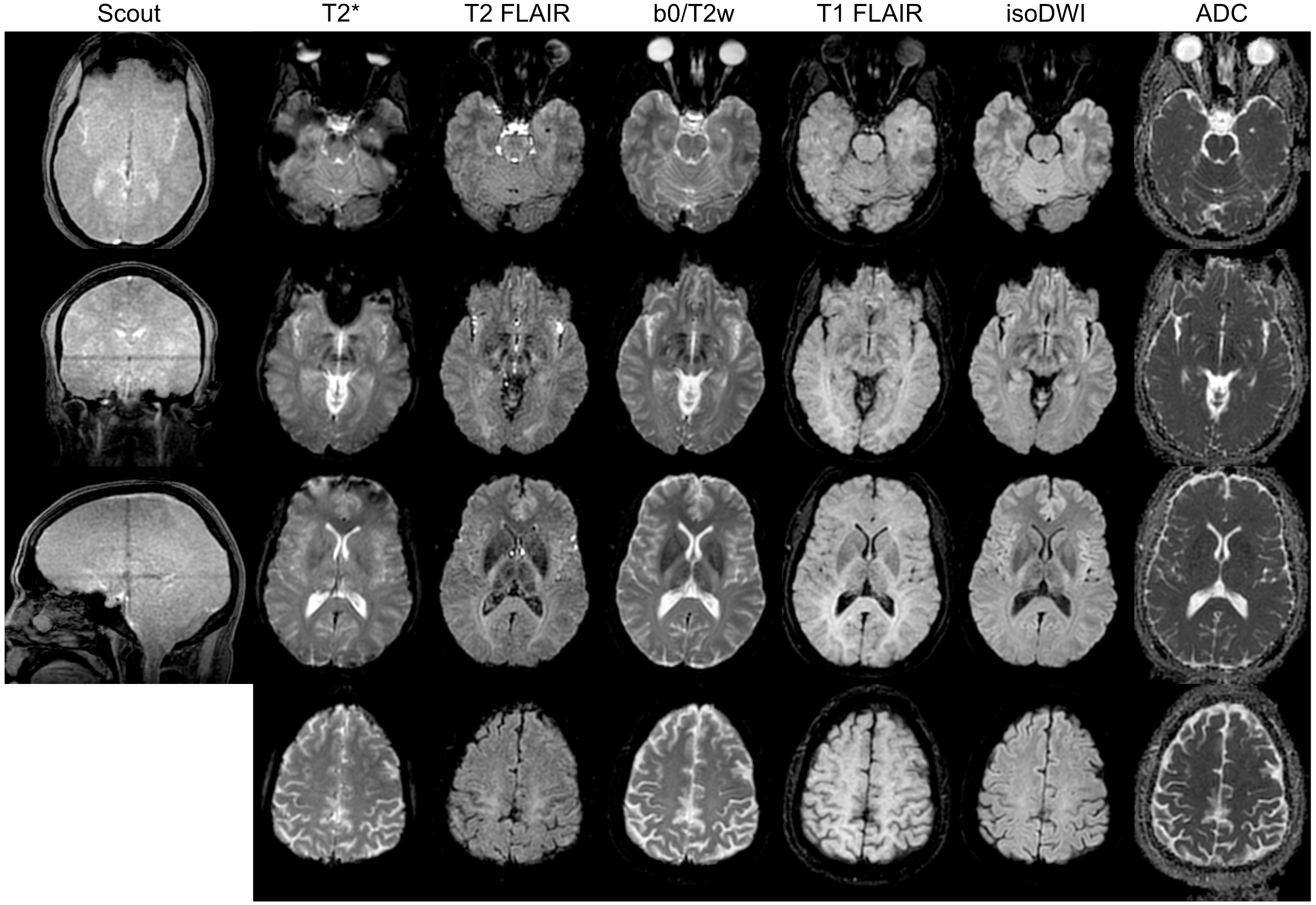
Figure 3. Reconstructed multi-contrast EPI data (distortion, and motion corrected) at 1.6×1.6 mm2 including a 3-plane scout, T2*, T2 FLAIR, b0/T2w, T1 FLAIR, isoDWI, and ADC respectively. The total scan time was 52 seconds
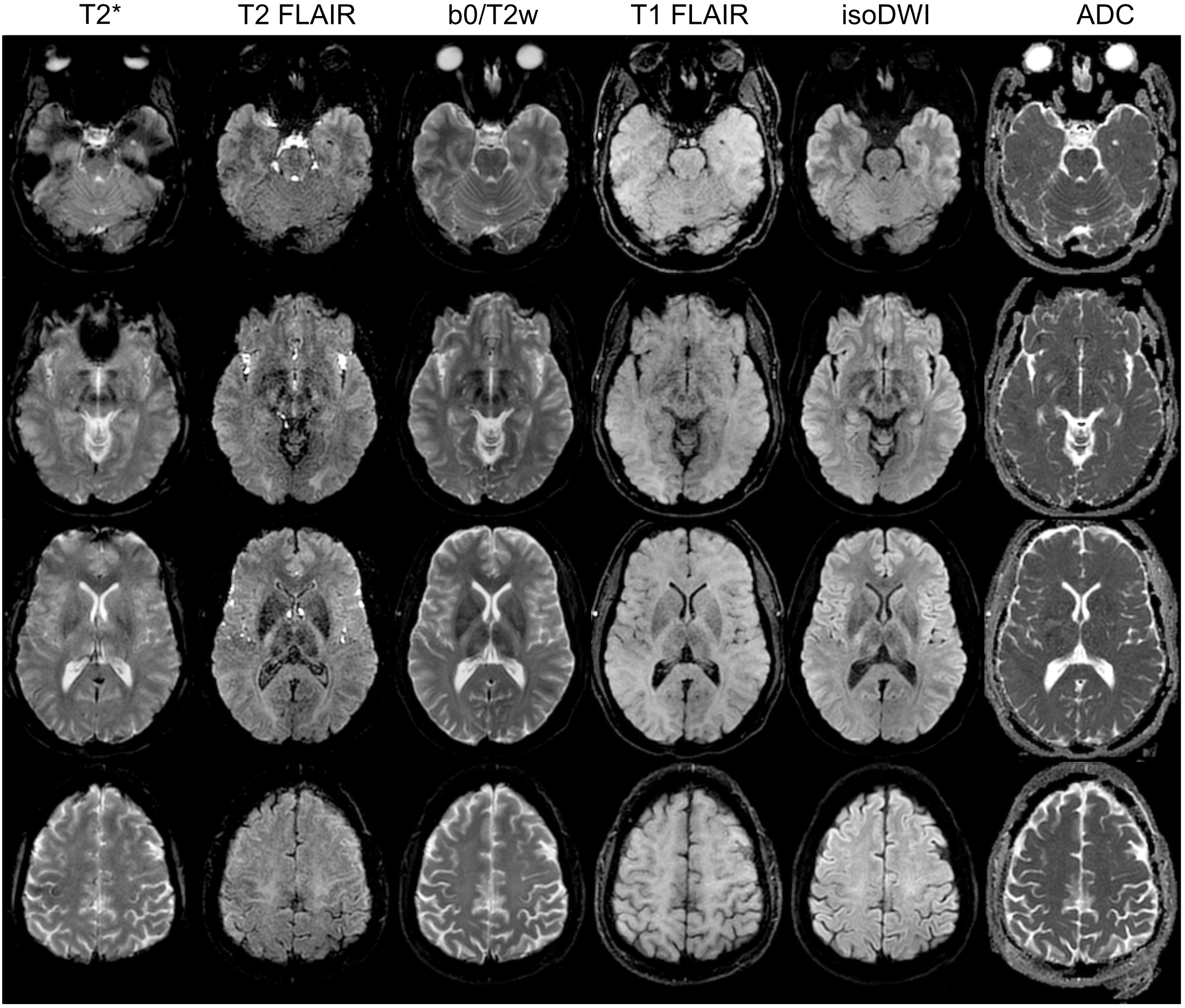
Figure 4. Reconstructed multi-contrast EPI data at 1.3×1.3 mm2 with R=3.
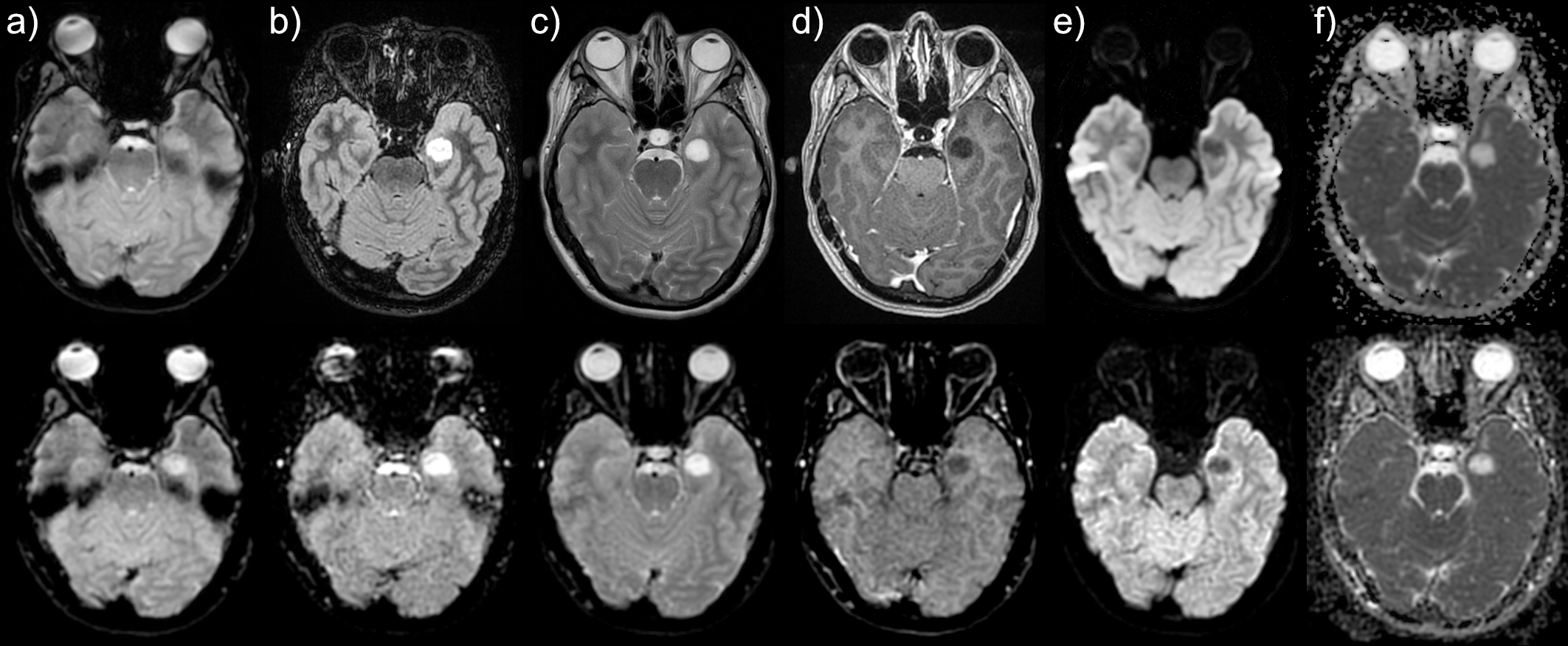
Figure 5. Comparison to standard clinical images as a) GRE EPI, b) axial reformat from Sag CUBE T2 FLAIR, c) axial T2 PROPELLER, d) axial BRAVO, e) 15 dir DWI, and corresponding ADC in f).