0369
Flexible and Efficient 2D Radial TSE T2 Mapping with Tiered Echo Sharing and with “Pseudo” Golden Angle Ratio Reordering1Siemens Healthcare, Los Angeles, CA, United States, 2Electrical and Computer Engineering, University of Arizona, Tucson, AZ, United States, 3Biomedical Engineering, University of Arizona, Tucson, AZ, United States, 4Siemens Healthcare, Salt Lake City, UT, United States, 5Siemens Healthcare, Tucson, AZ, United States, 6Siemens Helathcare, San Francisco, CA, 7Medical Imaging, University of Arizona, Tucson, AZ, United States
Synopsis
There has been recent increased interest in quantitative T2 mapping for accurate diagnosis of many pathological disorders. 2D radial TSE with tiered echo sharing and bit-reverse view ordering acquires TE data for T2 mapping in an efficient and motion robust fashion, but imposes limits on the choice of Echo Train Length (ETL). The current work introduces a novel view ordering algorithm with “pseudo” Golden Angle ratio (pGA) that removes restrictions in the ETL. With this algorithm, the scan time of 2D radial TSE is reduced (by18% in this study) without a compromise in image quality or in T2 mapping accuracy.
Introduction
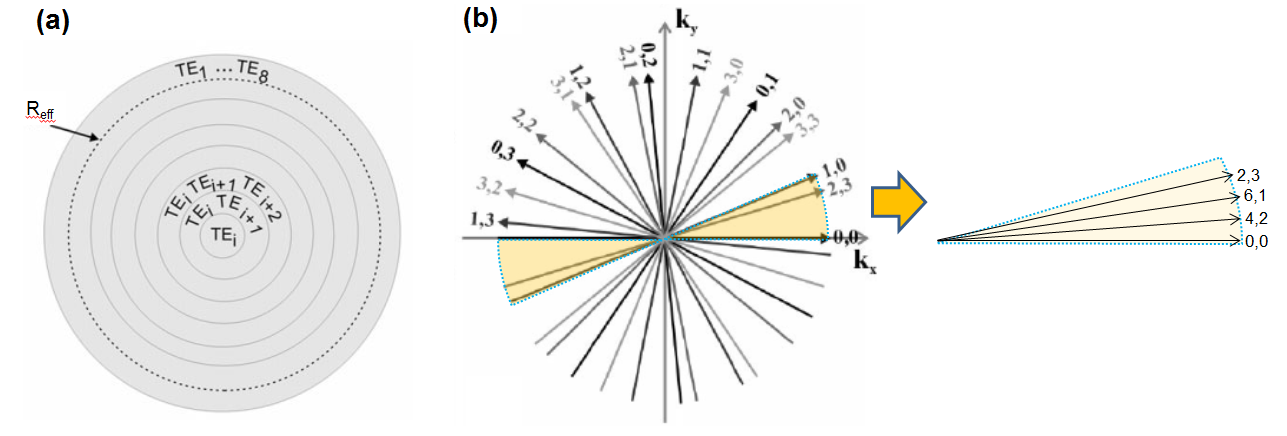
T2-weighted imaging has been widely used in the clinic routinely for the diagnosis of many pathological disorders, including focal liver disease [1-3]. A more accurate method is to obtain quantitative T2 measurement (via T2 mapping), but its clinical application is limited by the long scan time and respiratory motion sensitivity of the multi-echo SE- or TSE-based techniques typically employed. The 2D radial TSE with tiered echo sharing (Fig.1(a) [4]) and bit-reverse (BR) reordering (Fig.1(b) [5]) was introduced to address these shortcoming (Fig.1) [1-5]. However, due to the construction of BR, the acquired ETL must be power of 2. Since longer ETL>8 are scan time efficient, this ETL limitation prohibits further scan time optimization to make this technique widely acceptable in the clinical settings. The current work introduces a novel view ordering algorithm with “pseudo” Golden Angle ratio (pGA). The pGA is designed to generate random ordering of ordinal integers with no maximum integer restrictions. With this algorithm, the current 2D radial TSE can be further generalized to support any ETL and affording scan time reduction without a compromise in T2 mapping quality.Methods
For the 2D Radial TSE sequence with tiered echo sharing and with BR reordering, the angular sequence of the views, θ, is calculated from the following equation:
$$\ \theta=\left\{\left[(m_{i}-1)+(i-1)ET_{N}+(n-1)ETL \right]\triangle\theta\right\}\bmod\pi$$ ,
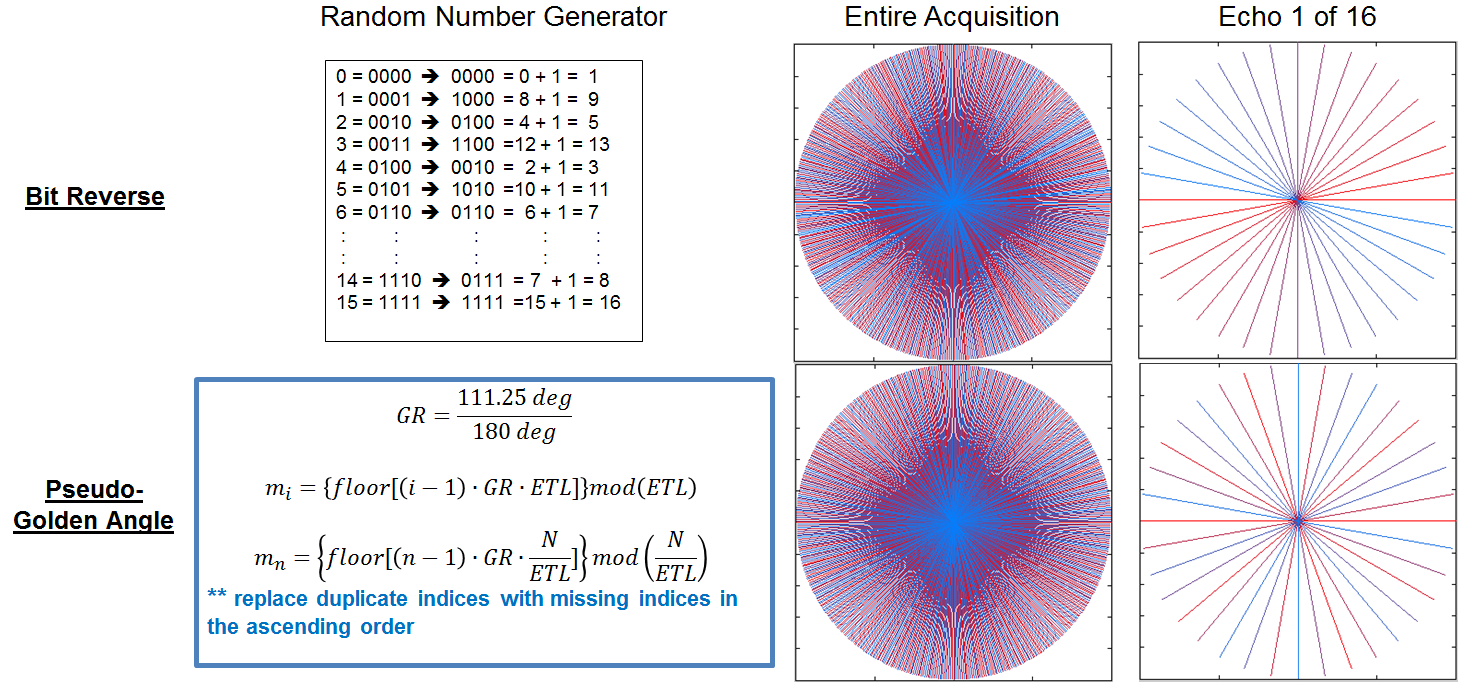
where i is the index for the echo number within an ETL, n is the index for the echo trains (TRs), ETN is total number of echo trains rounded up to the nearest multiples of ETL, N is the total number of views, and Δθ = π/N. mi represents a corresponding i-th random integers in the range [1 ETL], in this case generated by BR (Fig.2).
We propose to replace the BR with the pGA and redefine the first random integer term mi in the range of [0 ETL-1]. The third term (n-1) is also replaced with pGA randomized number mn in the range of [0 (N/ETL) -1] to promote the Golden Angle view order for each echo, potentially reducing streaking artifacts in synthetic echo images.
The sequence prototype was implemented on a 3T scanner (MAGNETOM Skyra, Siemens Healthcare, Germany). The technique was validated with 10 healthy volunteers under a local IRB approved protocol. Radial TSE liver MRI data was acquired with (a) free-breathing (FOV 400mm2, 240 base res, 400 radial views, 21 slices, ETL=16; in-plane res 1.7mm2, 8mm slice; FA180°; TR/TE 8.48ms/4500ms, Average 2; BW=496 Hz/pixel; total scan time 3:51 min) and with (b) breath-hold (FOV 400mm2, 256 base res, 192 radial views, 7 slices, ETL=16; in-plane res 1.6mm2, 8mm slice; FA 180°, TR/TE 8.58ms/1600ms; BW 501 Hz/pixel; total scan time 21 sec). For free-breathing protocol, BR and pGA are acquired with the identical protocol to compare the two reordering schemes. For the breath-hold protocol, ETL=22 was used for pGA, and this altered the protocol slightly (198 radial views, TR=1650ms, total scan time 17 sec). The resulting liver data sets were compared for overall image quality in M0 composite and synthetic TE images, and for T2 quantitative values.
Results
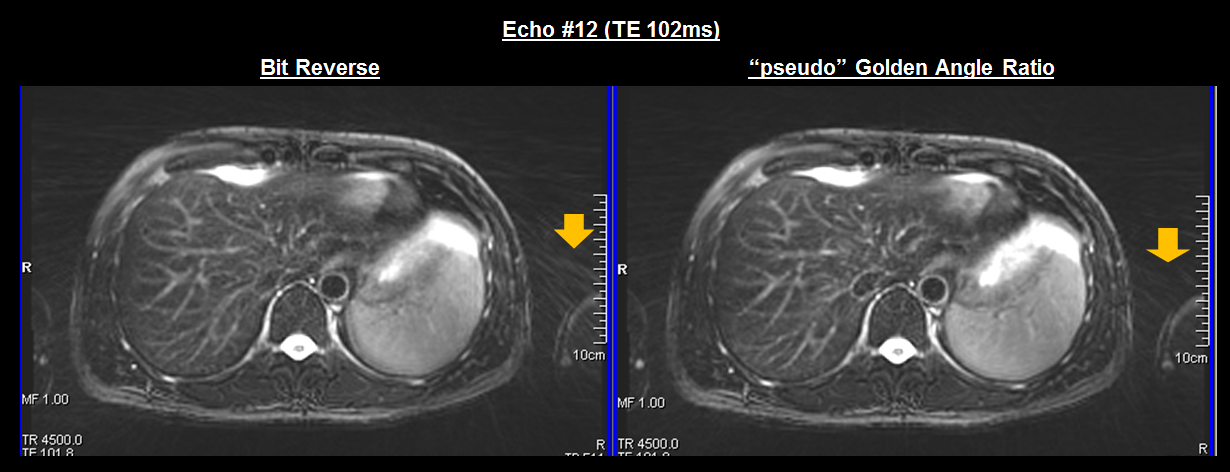
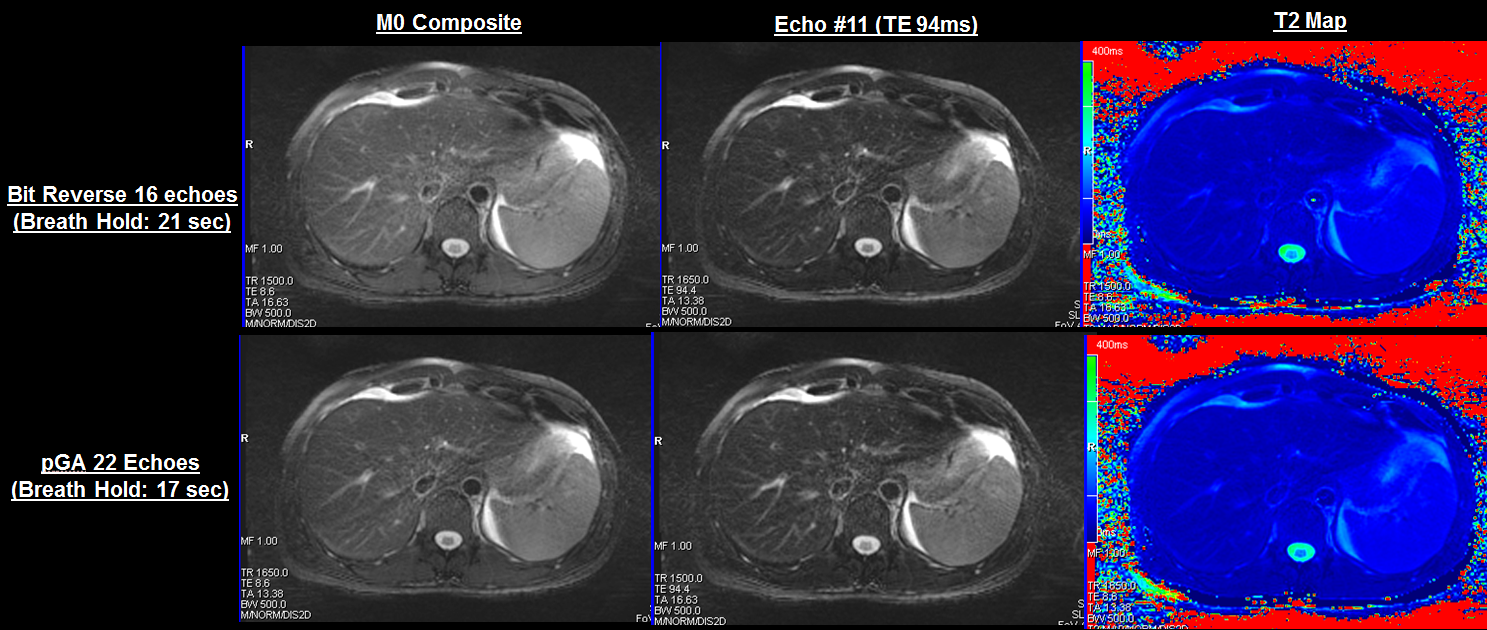
All scans and reconstructions were performed successfully (Fig.3, 4). The free-breathing protocol has shown subtle (if any) streaking artifacts reduction with pGA compared to BR in synthetic TE images. Composites are closely matched qualitatively and mean liver ROI T2 values compared well matched (38.3±5.7ms with BR vs 38.0±5.6ms with pGA). In breath-hold case, pGA with ETL=22 allowed an 18% reduction in scantime as compared to BR with ETL=16, while causing no degradation in image quality in the composite or synthetic TE images. Further, mean liver ROI T2 map values were essentially identical (37.5±5.4ms and 37.3±5.8ms for pGA and BR respectively).
Discussion
With potential extra time savings from flexible ETL, protocol optimization using the maximum applicable ETL is more efficient. To take full advantage of the time reduction introduced by the pGA ordering for flexible ETLs, it is also important to consider the SAR limitations when using long ETLs and refocusing FA of 180° (particularly when imaging at 3T). This can be achieved by combining lower refocusing FA with a T2 mapping approach which takes into account indirect echoes [3,6].Conclusion
Liver T2 mapping with motion robust and highly efficient 2D radial TSE technique has shown a great potential in the MR evaluation of liver and the abdomen in general, and has the added benefit of providing quantitative T2 information. The pGA ordering scheme presented here provides the necessary flexibility to bring the technique to routine clinical use.Acknowledgements
No acknowledgement found.References
[1] Altbach MI, Outwater EK, Trouard TP, Krupinski EA, Theilmann RJ, Stopeck AT, Kono M, Gmitro AF. Radial Fast Spin-Echo Method for T2-Weighted Imaging and T2 Mapping of the Liver. J Magn Reson Ima 16:179–189, 2002.
[2] Altbach MI. A radial magnetic resonance imaging method for imaging abdominal neoplasms. Methods of Cancer Diagnosis, Therapy, and Prognosis. Volume 3, 2009 edited by M.A. Hayat and published by Springer.
[3] Keerthivasan MB, Jeffries L, Blew D, Galons JP, Sharma P, Bilgin A, Martin DR, and Altbach MI. Fast reconstruction of T2 maps with indirect echo compensation using highly undersampled radial Fast Spin Echo data. Proceedings of Annual Meeting of the ISMRM, 24: 1534, 2016.
[4] Altbach MI, Bilgin A, Li Z, Clarkson EW, Gmitro AF. Processing of Radial Fast-spin Echo Data for Obtaining T2 Estimates from a Single K-Space Data Set. Magn Reson Med 54:549–559, 2005.
[5] Theilmann RJ, Gmitro AF, Altbach MI, Trouard TP. View Ordering in Radial Fast Spin-Echo Imaging. Magn Reson Med, 51, 768-774, 2004.
[6] Huang C, Bilgin A, Barr T, and Altbach MI. T2 Relaxometry with Indirect Echo Compensation from Highly Undersampled Data. Magn Reson Med, 70: 1026-1037, 2013.
Figures