0345
Distribution of Intraluminal Thrombus Composition in Abdominal Aortic Aneurysms by Diameter: a High Resolution MRI study1Radiology, University of California, San Francisco, San Francisco, CA, United States, 2Radiology, Changhai Hospital, Shanghai, People's Republic of China
Synopsis
Intraluminal thrombus (ILT) composition as identified by MRI has been suggested to be a marker of likely abdominal aortic aneurysm (AAA) progression. However, little is known about the distribution of ILT composition across different sizes of AAAs. This study investigated the ILT composition by AAA diameter in 62 patients from two centers. We found ILT distributed differentially by size, with an increasing mix of fresh and old ILT in larger AAAs. ILT composition is a potential indicator of AAA progression. Larger, prospective studies are needed to clarify its prognostic value in managing AAA patients.
Purpose
The rupture risk of abdominal aortic aneurysm (AAA) increases with maximal. Clinically, patients with AAAs >5.5 cm are selected for intervention because this is the threshold when rupture risk is higher than the surgery risk. Although diameter is useful and easy to use clinically, it has limitations: a considerable number of small AAAs do rupture. A previous study suggested that AAAs with fresh intraluminal thrombus (ILT), as identified by high signal on T1-weighted MRI, grow as much as 2 times faster than AAAs without fresh ILT, despite similar initial diameters1. The distribution of ILT composition in different sizes of AAA, however, has rarely been studied. In this study we aims to evaluate 1) the distribution of ILT composition across AAA diameters and 2) the relationship between ILT composition and traditional risk factors.Methods
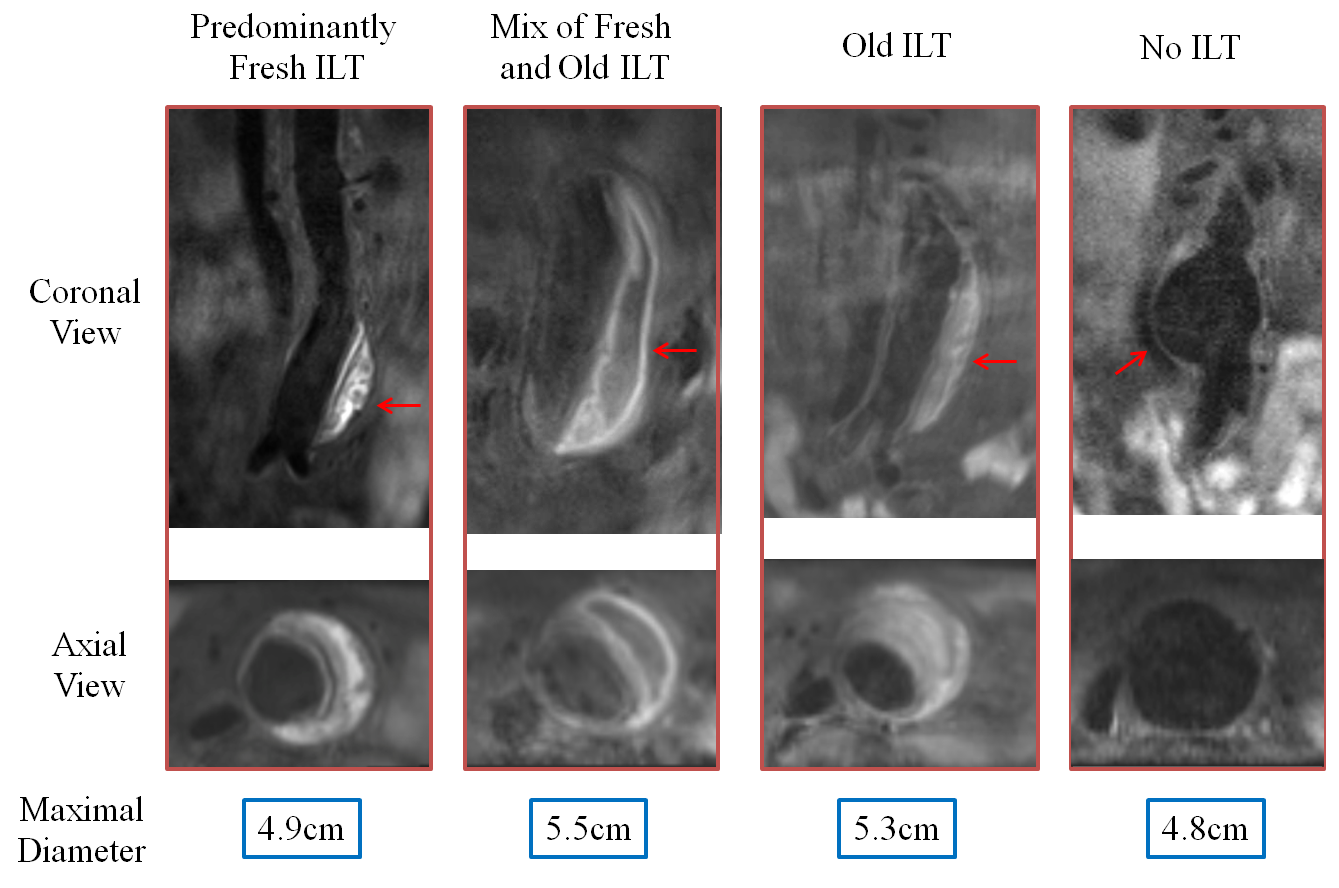
Study population: 62 patients (58 male, age 72.7±7.8 years) with AAA disease were recruited in two centres (UCSF and Shanghai). Scanning protocols: MRI scans were performed on Siemens Skyra 3T scanners. A previous developed and validated 3D black blood MRI sequence (blood suppressed T1-weighted fast-spin-echo with variable flip angle train, DANTE-SPACE 2 3) was used to image the 3D geometry of AAA and the ILT composition: TR/TE: 800ms/20ms, 1.3mm isotropic resolution, echo train length 60. Image analysis: Maximal AAA diameter was measured using multi-planar reconstruction (MPR) on black blood MRI images. Patients were divided into 5 groups based on diameter: <4cm; 4-4.5cm; 4.5-5cm; 5-5.5cm; >5.5cm. ILT was determined as fresh if its signal on black blood MRI was higher than 1.2 times of adjacent psoas muscles 1, and old ILT was determined when the ratio is lower than 1.2. Four ILT types were analysed based on a previous defined criteria 3: 1) Predominately fresh 2) Mixture of fresh and old ILT; 3) Old; and 4) No ILT. Patient clinical information including age, sex, hypertension, smoking, diabetes, coronary artery disease were also recorded. The relationship between ILT types and diameters/traditional risk factors were analysed.Results
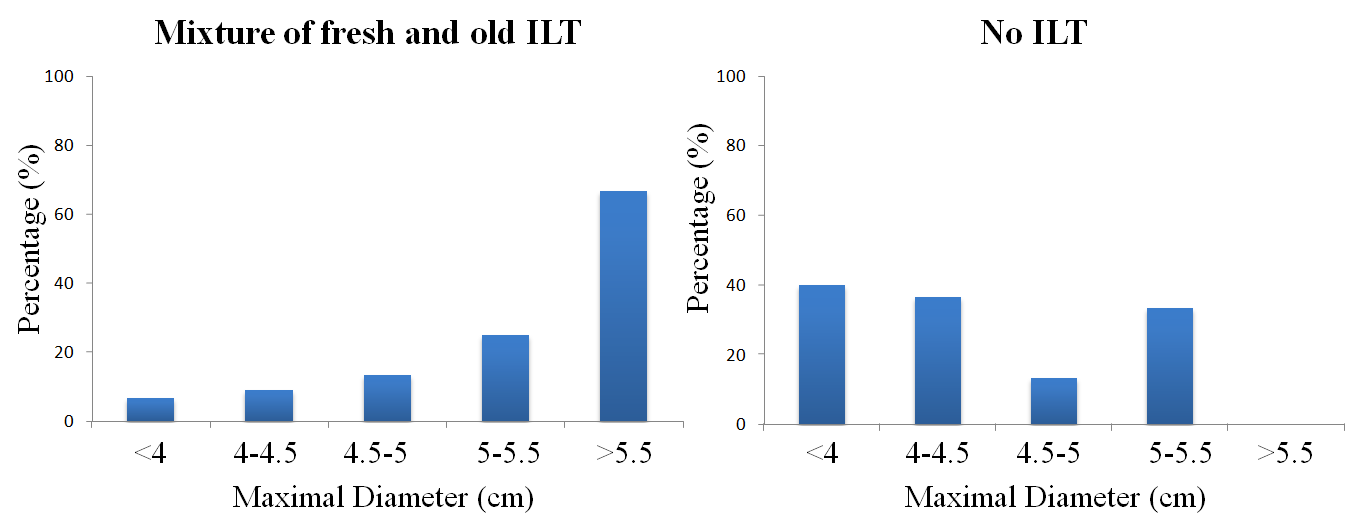
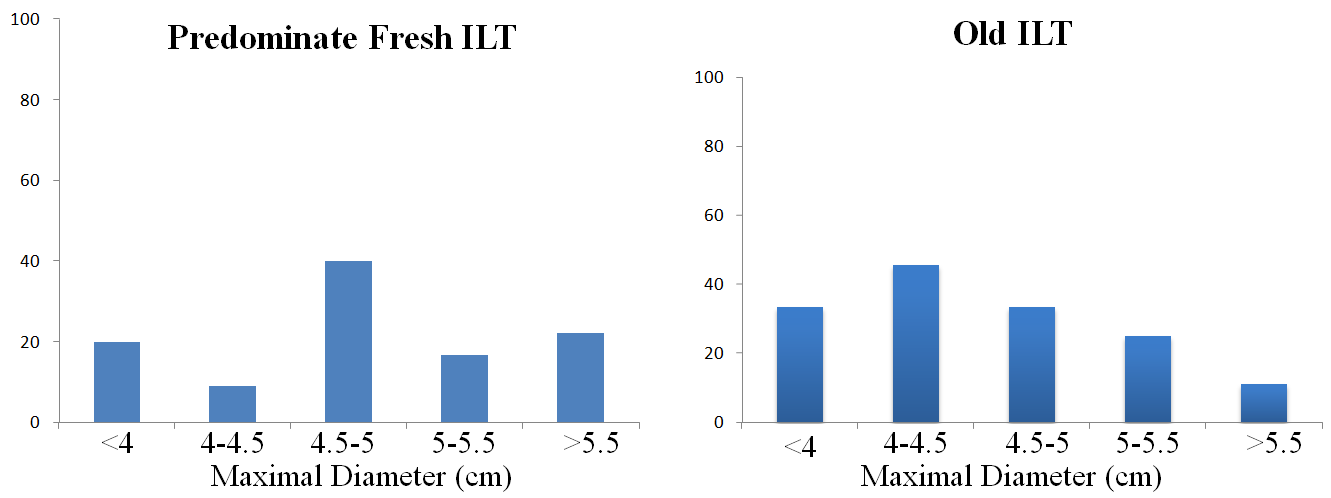
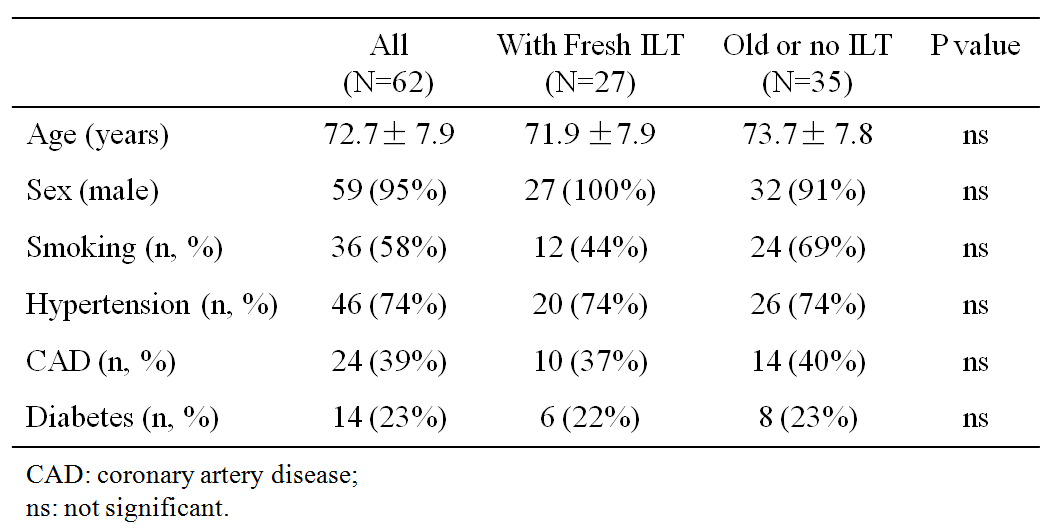
The number of AAAs by size group is as follows: <4cm (n=15); 4-4.5cm (n=11); 4.5-5cm (n=15); 5-5.5cm (n=12); and >5.5cm (n=9). Examples of black blood MRI of AAAs with four types of ILT are shown in Figure 1. AAAs with similar diameters can have distinct ILT compositions as identified by MRI. The distribution of four types of ILT is shown in Figure 2 and 3. There is a trend of an increasing fraction of mixed ILT and decreasing fraction of those that are ILT-free as the AAA diameter increases. However, both predominantly fresh ILT and old ILT subtypes are most prevalent in intermediate sizes (4-5 cm). Large AAAs (>5.5cm) have significantly more fresh ILT compared to small AAAs (<5.5cm) (8/9 vs. 19/53, p=0.008). There is no relation between traditional risk factors and ILT composition (Table 1).Discussion
To our knowledge, this is the first study of the distribution of ILT composition as a function of diameter. We found ILT subtypes had distinct distributions depending on AAA size. An increasing mixture of ILT in larger AAAs may indicate that mixed ILT is a potential risk factor, whereas a decrease in ILT-free presentation in larger AAAs may indicate that being ILT-free is a low risk factor. Interestingly, predominantly fresh ILT and old ILT were most prevalent in intermediate size AAAs (4-5cm), suggesting that AAAs with 4-5cm diameters have one of two fates: 1) continued growth with evolution of ILT to the mixed subtype common in larger AAAs, or stability with ILT becoming old over time. Whether ILT composition is related to progressive disease needs to be investigated in larger, longitudinal studies. The unique 3D assessment of ILT composition provided by high resolution black blood MRI can also improve the biomechanical modeling of AAAs, given that fresh versus old ILT have different material properties. We did not observe a relationship between ILT composition and traditional risk factors, which may be due to the limited sample size in this study.Conclusion
Subtypes of ILT composition can be uniquely identified by MRI and are distributed differently across AAA diameters. We found that a mixture of fresh and old ILT is associated with larger AAA diameters. Larger, prospective studies are needed to address the potential of using ILT composition to improve risk stratification of AAA disease.Acknowledgements
This study is supported by NIH grants R01HL114118 and R01HL123759References
1. Nguyen VL, Leiner T, Hellenthal FA, Backes WH, Wishaupt MC, van der Geest RJ, et al. Abdominal aortic aneurysms with high thrombus signal intensity on magnetic resonance imaging are associated with high growth rate. Eur J Vasc Endovasc Surg. 2014;48:676-684
2. Zhu C, Haraldsson H, Faraji F, Owens C, Gasper W, Ahn S, et al. Isotropic 3d black blood mri of abdominal aortic aneurysm wall and intraluminal thrombus. Magn Reson Imaging. 2016;34:18-25
3. Zhu C, Tian B, Leach JR, Liu Q, Lu J, Chen L, et al. Non-contrast 3d black blood mri for abdominal aortic aneurysm surveillance: Comparison with ct angiography. Eur Radiol. 2016
Figures