Bo Li1,2, Hao Li3, Guofu Huang1, Xia Qian1, Wei Wang1, and Li Dong4
1Center Laboratory, The First Hospital of Nanchang City, Nanchang, People's Republic of China, 2Department of Radiology, The Third Affiliated Hospital of Nanchang University, Nanchang, People's Republic of China, 3Department of Radiology, University of Cambridge, Cambridge, United Kingdom, 4Department of Radiology, Beijing Anzhen Hospital, Beijing, People's Republic of China
Synopsis
We sought to achieve high-quality simultaneous black- and gray-blood MR imaging using the CS based dual contrast imaging technique proposed on 2015. The performances on the blood suppression efficiency, image quality and morphological measurements for the CS based dual-contrast imaging technique were investigated. Seven healthy volunteers and five patients with carotid artery stenosis were recruited in this study. STR, CTR were calculated. LA and WA were measured. The comparisons for the black- and gray-blood image quality and the presence of plaque calcifications were implemented. This technique provides spatially matched black- and gray- images and excellent visualization for vessel wall imaging.
Purpose
The simultaneous black- and gray-blood MR imaging technique not only can provide the depictions of the plaque and its constituents with the black-blood contrast but also has the ability to visualize the vascular calcifications on the plaque with the gray-blood contrast. The first dual-blood contrast technique was proposed in 20121. However, this technique provides a significant lower image quality than the corresponding single-contrast data set because of the reduced k-space sampling and the use of homodyne reconstruction. In this study, we sought to achieve high-quality simultaneous black- and gray-blood MR imaging by the compressed sensing (CS) based black- and gray-blood simultaneous imaging technique2. The performances on the blood suppression efficiency, image quality and morphological measurements for the CS based dual-contrast imaging technique were investigated.Materials and Methods
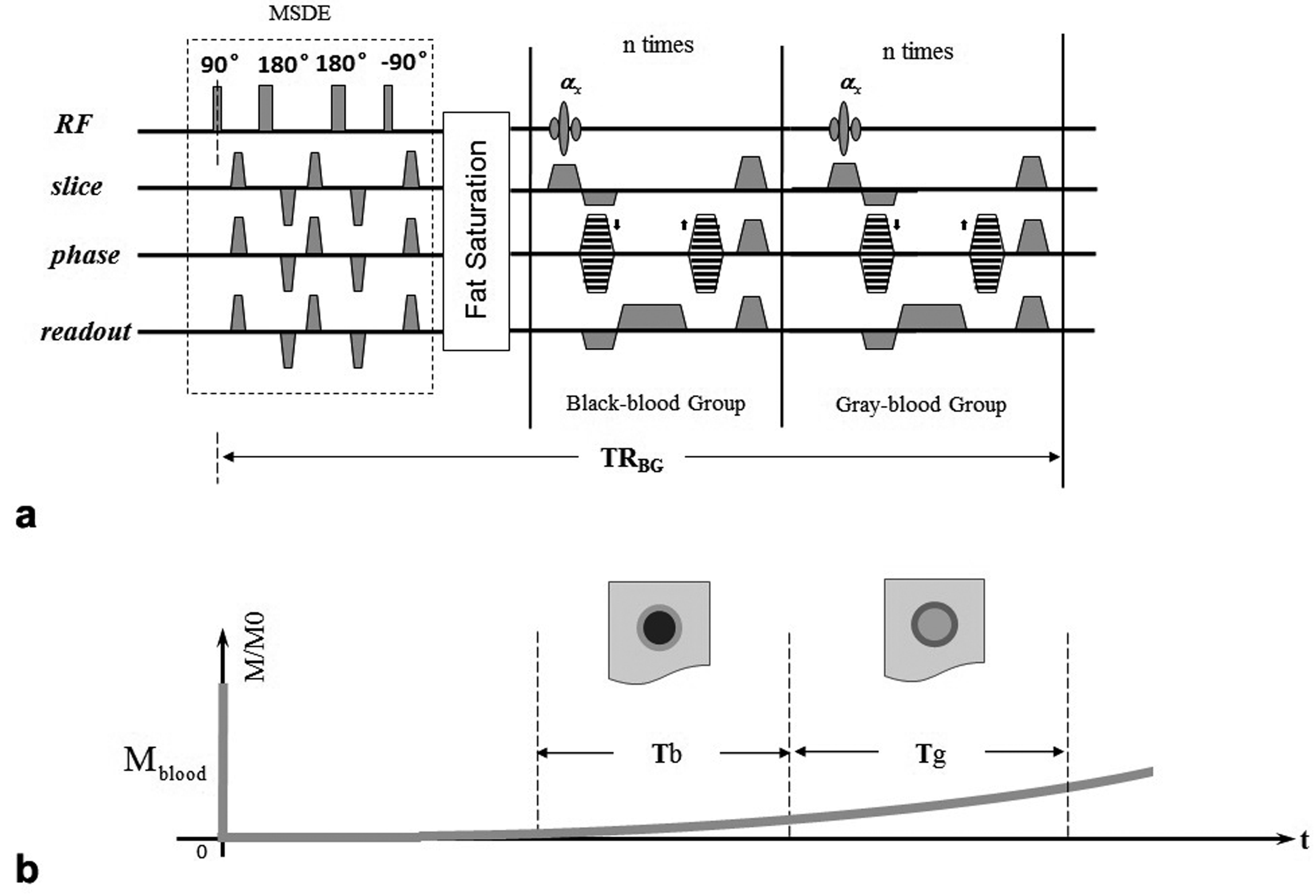
The CS based simultaneous black- and gray-blood (CS-siBLAG) sequence consists of a MSDE preparation module for the suppression of blood signal, a fat saturation module for optimal outer vessel wall definition, an n-times repeated 3D spoiled FLASH sequence for filling black-blood k-space, and another n-times repeated 3D FLASH acquisitions for filling gray-blood, as shown in Fig. 1. As the technique has two k-spaces to fill up, its scan time is much longer than that of one single-contrast scan. Thus, the CS under-sampling strategy3 and L1-norm algorithm4 were therefore employed to shorten the acquisition time and recover images from the under-sampled 3D k-space dataset.
After institutional review board approval and written informed consent, seven healthy volunteers and five patients with carotid artery stenosis were recruited in this study. The study was performed on a clinical 3T whole-body MR imaging system (Signa TM; GE Medical Systems, Milwaukee, WI). An eight-channel phased-array bilateral carotid coil was used for signal reception. For healthy subjects imaging, it had five sequential CS-siBLAG scans with 1, 2, 3, 4 and 5-fold acceleration factors, and then a 2D QIR-FSE was implemented; for patients imaging, 1, 3 and 5-fold accelerated CS-siBLAG scans and fully sampled 3D TOF sequence were implemented. All images were acquired in the axial plane.
The image analysis for healthy subjects imaging is: a. the signal-to-tissue ratio (STR) and the contrast-to-tissue ratio (CTR)3 were calculated for the measures of flowing signal suppression performance and imaging quality for the black-blood imaging of the CS-siBLAG technique; b. vessel lumen area (LA) and wall area (WA) were measured for morphological comparisons. P value less than 0.05 was considered significant.
The image analysis for patients imaging is: a. the comparison of the black- and gray-blood image quality between the fully sampled and the under-sampled CS-siBLAG images; b. the comparison of the presence of plaque calcification between the gray-blood images of CS-siBLAG at 1x, 3x and 5x and the bright-blood images of 3D TOF.
Results
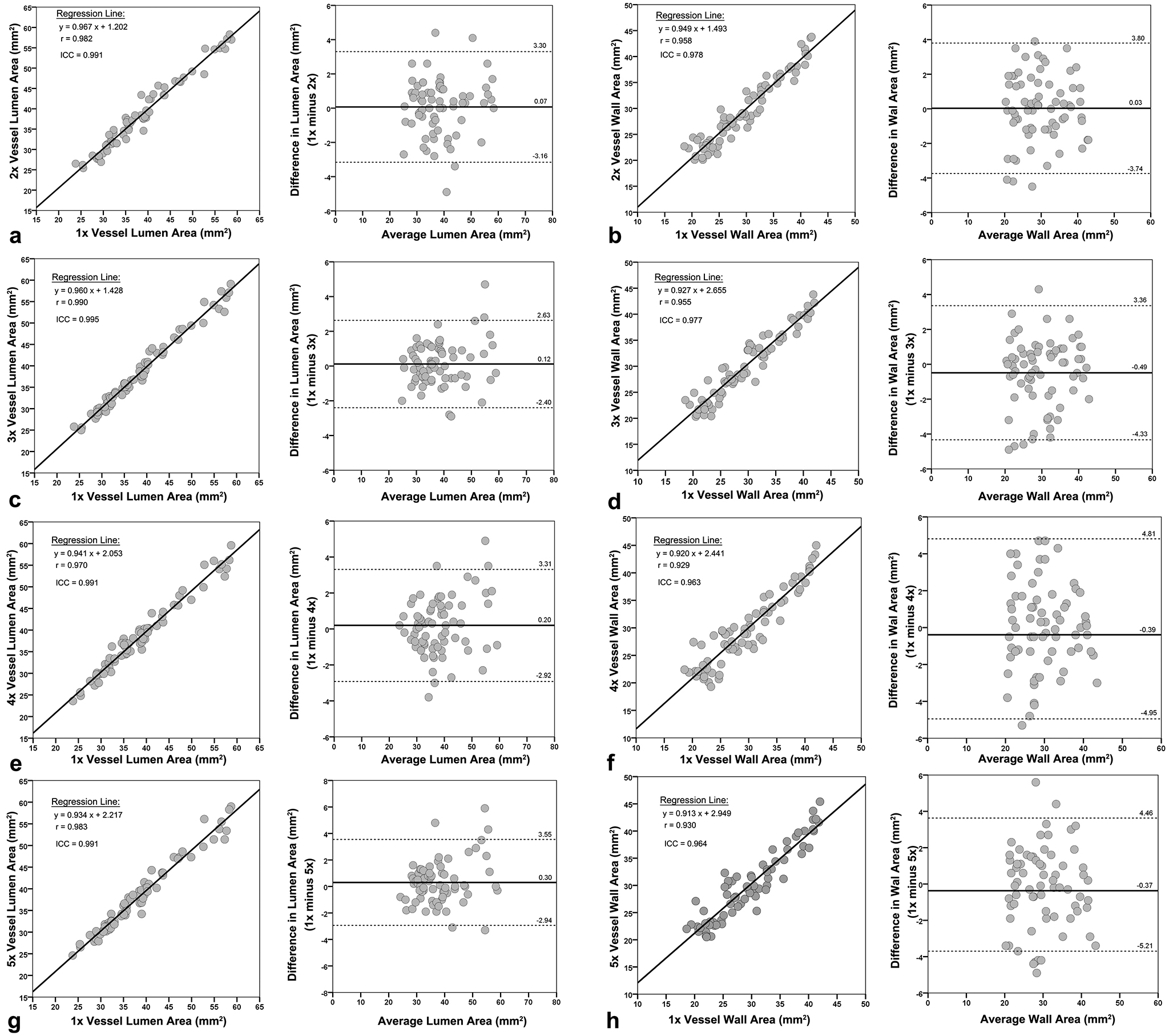
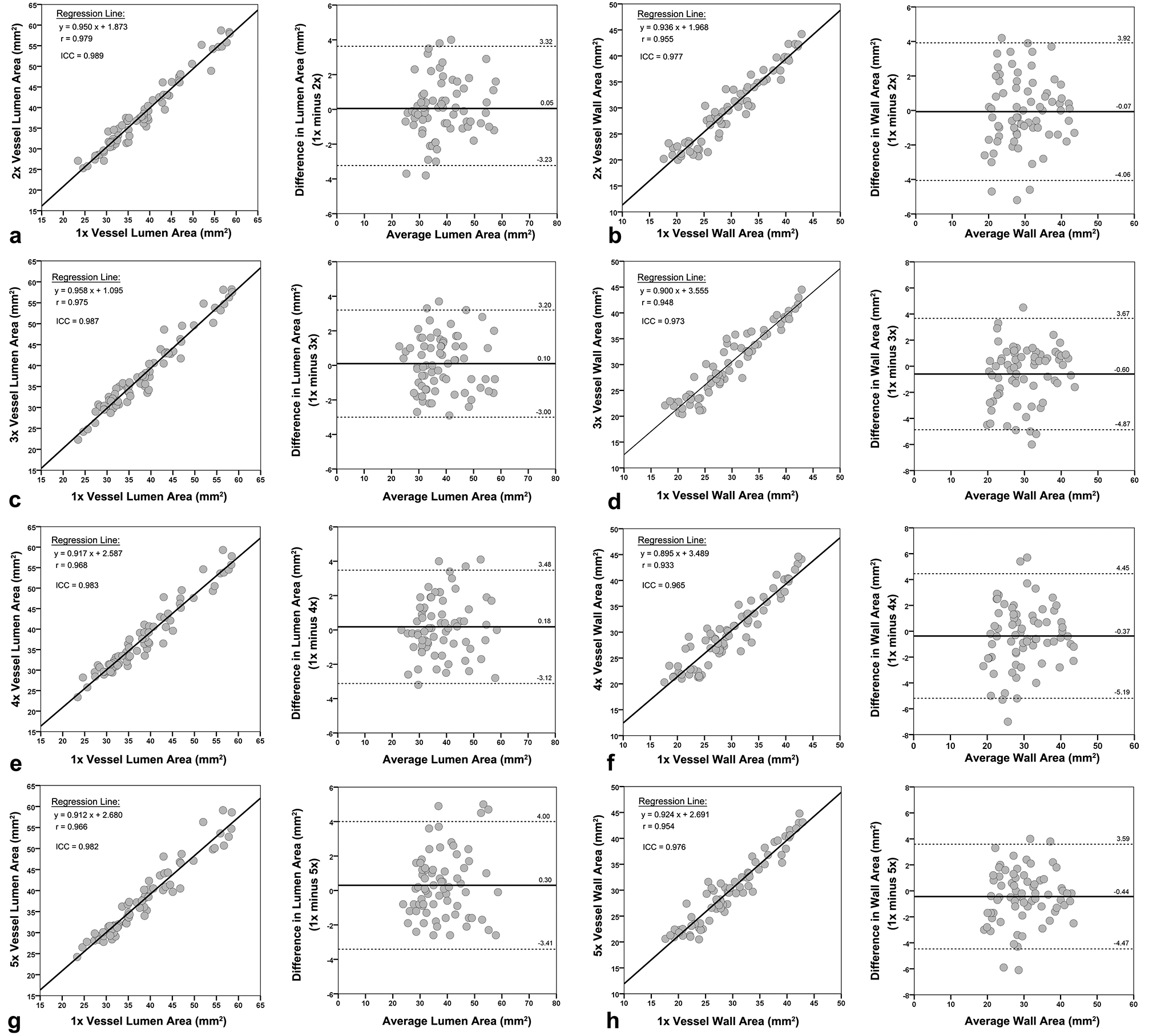
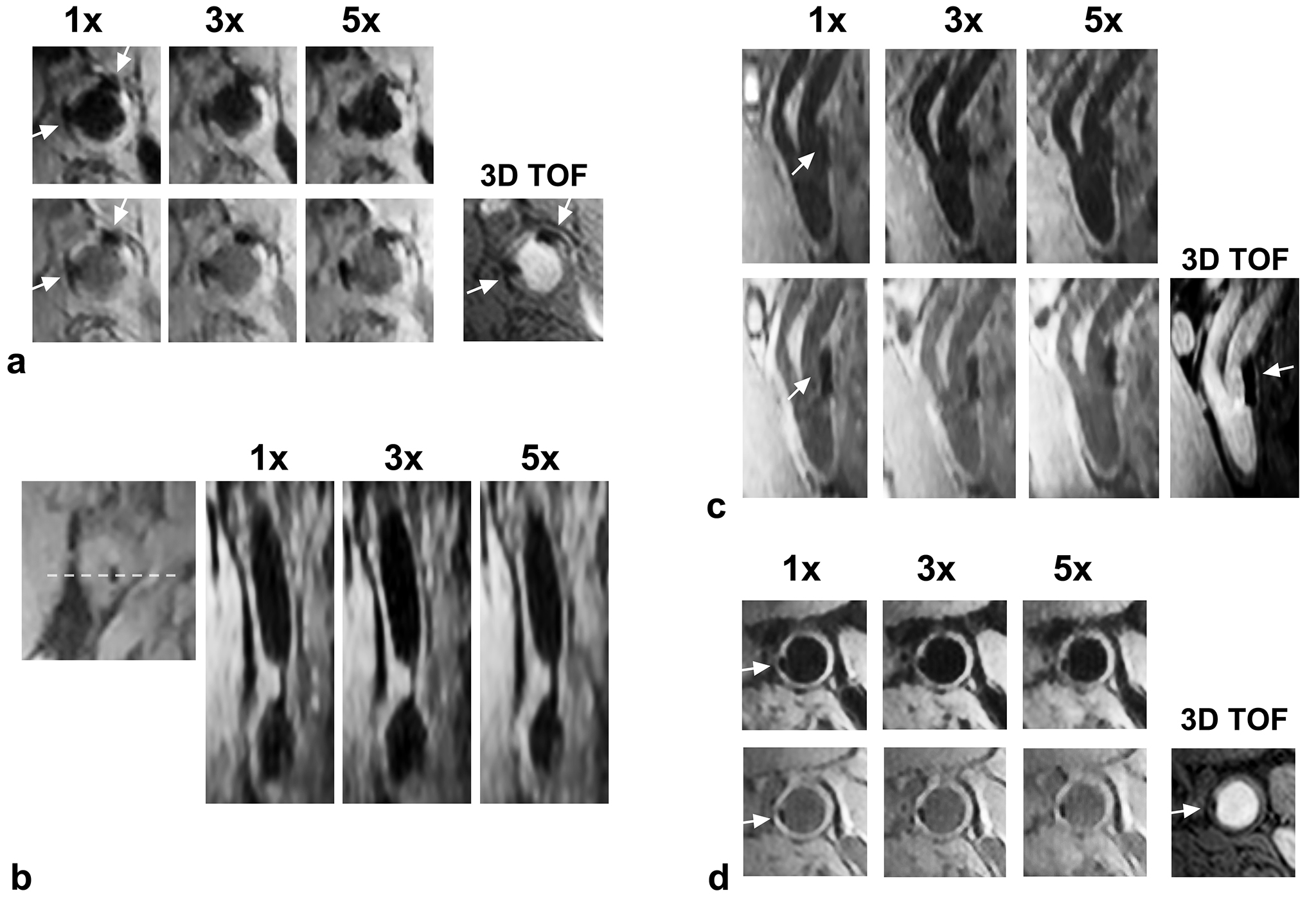
For healthy subjects imaging, STR and CTR values obtained with 2 to 5-fold accelerations were not significantly different from those with full acquisition. There were no statistically significant differences in LA and WA for 2D QIR-FSE and each CS-siBLAG sequence in both black- and gray-blood contrast, and LA and WA measured at 2x, 3x, 4x and 5x were all highly correlated to the corresponding values at 1x. Scatter and Bland-Altman plots for black-blood and gray-blood WAs and LAs are shown in Fig. 2 and Fig. 3. Representative axial images and oblique reformatted images obtained with CS-siBLAG at 1x, 2x, 3x, 4x and 5x accelerations in a volunteer are shown in Fig. 4. For patients imaging, two radiologists both found that the dual-contrast images at 3x acceleration exhibited comparable image quality to that of the fully sampled acquisition, and that the images at 5x exhibited slightly blurred vessel wall and outer vessel wall boundaries. Figure 5 depicts the images from CS-siBLAG in patients with carotid artery stenosis. The number of plaque calcifications detected by the gray-blood imaging at 1x and 3x were similar to that of 3D TOF, but 5x showed fewer calcifications than that at 1x and 3x in each patient.Discussion
The image blurring at 5x is the reason of the
missed calcifications detection. Fewer measurements for CS
reconstruction will lead to the insufficient removal of the incoherent artifacts,
which may hinder the delineation of calcifications and lead to fewer calcifications detection.
Adding
a gray-blood acquisition and appending a time delay (TD) can generate a T1
relaxation for all tissues. According to Bloch simulation, the signal
improvement ratios are 44%, 56%, 42% and 44% for lipid core, fibrotic tissue, arterial
wall and intraplaque hemorrhage, respectively, compared to signals from single-contrast
black-blood imaging without TD.
Acknowledgements
No acknowledgement found.References
1. Koktzoglou I. Gray Blood Magnetic
Resonance for Carotid Wall Imaging and Visualization of Deep-Seated and
Superficial Vascular Calcifications. Magnetic Resonance in Medicine.
2013;70:75-85.
2. Li H, Li B, Huang W, Dong L, Zhang J.
Flow Artifact Removal in Carotid Wall Imaging Based on Black and Gray-Blood
Dual-Contrast Images Subtraction. Magn Reson Med. 2016;doi: 10.1002/mrm.26218.
3. Li B, Dong L, Chen B, Ji S, Cai W, Wang
Y, et al. Turbo fast three-dimensional carotid artery black-blood MRI by
combining three-dimensional MERGE sequence with compressed sensing. Magn Reson
Med 2013;70:1347–52.
4. Lustig M, Donoho D, Pauly JM. Sparse MRI:
The application of compressed sensing for rapid MR imaging. Magn Reson Med.
2007;58:1182-1195.