0295
4D Flow MRI during Exercise in Prematurely Born Adults and Children1Medical Physics, University of Wisconsin - Madison, Madison, WI, United States, 2Pediatrics, University of Wisconsin - Madison, Madison, WI, United States, 3Radiology, University of Wisconsin - Madison, Madison, WI, United States
Synopsis
Preterm birth can result in impaired development of lung airways and vasculature, but the long term implications are unclear. With this in mind, we performed 4D flow imaging in the aorta and pulmonary artery during exercise at 70% maximal power in both children and adults who had been born prematurely to identify any differences in flow characteristics relative to healthy controls. Although no statistically significant differences were identified between our groups, some preterm cohorts showed increased cardiac output and mean velocity. The significance of these trends should become apparent as we continue to recruit subjects and increase our statistical power.
Purpose
Preterm birth is a significant healthcare problem, accounting for roughly 1 in 10 births. Prematurely born infants may require mechanical ventilation and oxygen therapy, which has been shown to impair the development of lung airways and vasculature. Little is known about the long-term implications of these therapies on cardiac function and pulmonary circulation, however. Exercise stress tests are a useful tool for discerning differences in cardiac function between control and patient groups that may not be apparent at rest. Previously we have demonstrated the feasibility of 4D flow MRI during exercise1. In this work, we present initial findings from 4D flow measures of aortic and pulmonary flow at rest and during exercise in a small cohort of preterm adults and children at 70% of their maximal power.Methods
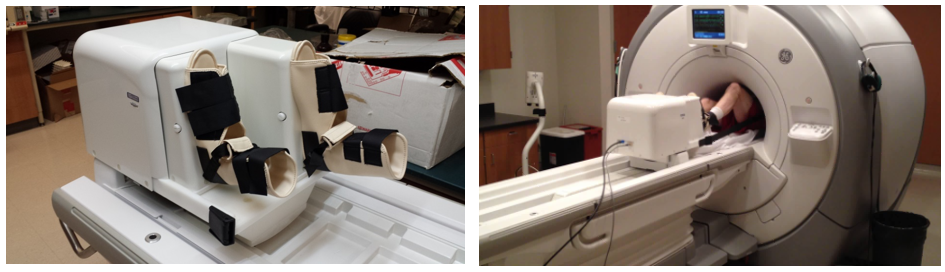
Twenty-one subjects were imaged on a clinical 3.0 T scanner (Discovery MR750, GE Healthcare) with an 8-channel phased-array cardiac coil. These subjects were divided into four cohorts: 5 preterm adults (25±1 years; 3M, 2F) with 6 age-matched controls (26±1 years; 2M, 4F) and 4 preterm children (13±1 years; 2M, 2F) with 6 age-matched controls (13±1 years; 1M, 5F). 4D flow imaging was performed with a radially-undersampled PC-VIPR sequence2 (TR/TE=6.2/2.0ms; FA=10°; VENC=200cm/s; FOV=32x32x32cm; resolution=1.25mm isotropic; scan time=9.25min; temporal resolution=58ms; retrospective respiratory and ECG-gating) at rest and during exercise with an MR-compatible exercise device (Ergospect) (Fig.1). Subjects exercised at 70% of their maximal power, as previously determined from a maximum power test on an exercise bike. Continuous tracking of stepping cadence was used to automatically adjust the resistance to maintain the targeted workload. Exercise imaging began when the subject reached a steady-state heart rate. Flow and velocity measurements were made in the ascending aorta and main pulmonary artery (PA) using a customized MATLAB tool3. A paired student’s t-test was used to assess statistically significant changes (p<0.05) between rest and stress. To quantify changes in SNR between rest and stress, approximate SNR measurements were made in the adult controls by comparing mean signal in the aorta against the standard deviation of the background signal.Results
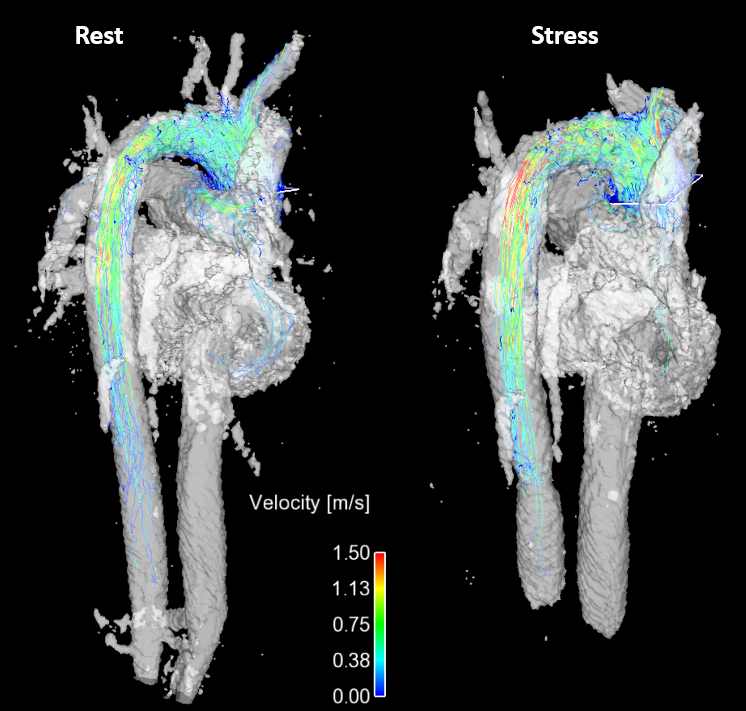
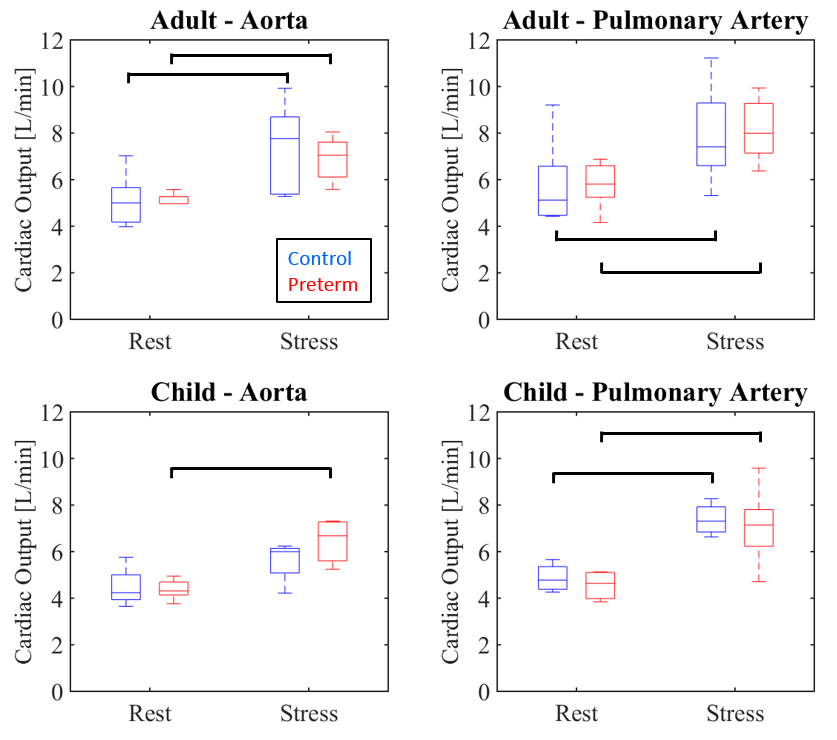
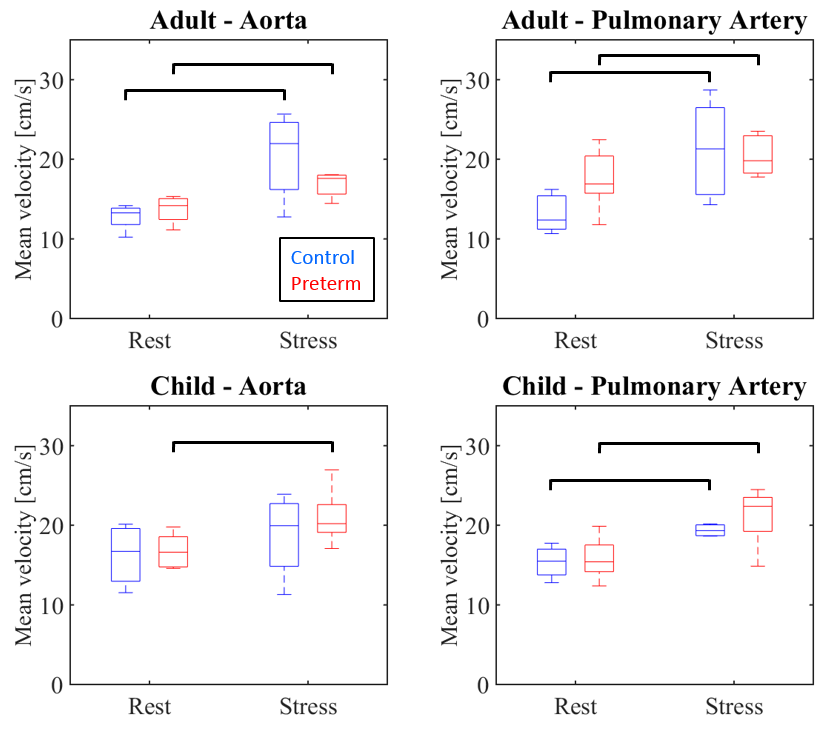
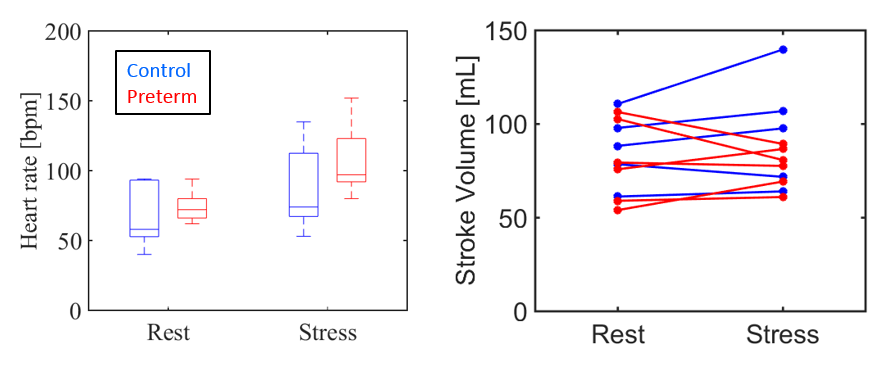
We successfully performed resting and exercise stress 4D flow MRI in 20/21 subjects. We observed a decrease in ECG consistency during exercise where approximately 85% of recorded heart beats were within the expected RR interval for most subjects compared to 99% at rest. One preterm child was excluded from analysis due to unreliable ECG triggering during exercise. Fig. 2 shows a comparison of flow visualization in an adult control at both rest and during exercise. The adult controls demonstrated decreased SNR during exercise imaging, with an average decrease of 11%. The increase in image noise during exercise did not prohibit vessel segmentation or flow measurements. Fig. 3 and 4 show the responses of cardiac output and mean velocity to exercise in the aorta and PA for each cohort. In both vessels, all cohorts showed statistically significant increases in these parameters between rest and exercise. However, differences between the control groups and preterm subjects were less apparent with no intergroup measurements showing statistical significance. Interestingly, while the adult controls and preterm subjects showed similar measures for cardiac output, it was achieved through different mechanisms. With exercise, the preterm subjects showed a larger increase in heart rate than the controls, but a reduced response in stroke volume (Fig. 5).Discussion
Movement of ECG leads likely caused the decreased consistency in gating, as R wave detection was less reliable during exercise. While no statistically significant differences were found in flow between the preterm subjects and healthy controls at rest or stress, this may be a result of the relative lack of statistical power with the small sample size. The preterm population showed consistently higher mean values for cardiac output in the PA in the adults and higher mean velocities in the PA during stress in the children. This could be indicative of increased cardiac work load as a result of increased pulmonary resistance. Improved statistical power with continued subject recruitment should discern if observed trends are representative of physiologic differences.Conclusion
We used 4D flow MRI during an exercise challenge to investigate if impaired pulmonary development as a result of preterm birth had long-term implications on cardiac function. Imaging during exercise resulted in a small decrease in SNR. This work is the first step towards a comprehensive, non-invasive, hemodynamic assessment of exercise-induced changes to cardiopulmonary interactions using 4D flow. In future work, we will use the 4D flow data to compare flow-field characteristics between subject groups.Acknowledgements
We gratefully acknowledge research support from GE Healthcare.References
1. Macdonald J, Beshish A, Haraldsdottir K, Eldridge M, et al. 4D Flow Cardiovascular during Exercise. Society for Cardiovascular Magnetic Resonance 20th Annual Scientific Sessions. 2017.
2. Johnson KM, Lum DP, Turski PA, Block WF, et al. Improved 3D phase contrast MRI with off-resonance corrected dual echo VIPR. MRM. 2008;60(6):1329-1336.
3. Stalder AF, Russe MF, Frydrychowicz A, Bock J, et al. Quantitative 2D and 3D phase contrast MRI: Optimized analysis of blood flow and vessel wall parameters. MRM. 2008; 60(5): 1218-1231
Figures