0292
4D flow MRI based quantification of regional stiffness in the thoracic aorta in stroke patients compared to transesophageal echocardiography1Department of Neurology and Neurophysiology, University Medical Center Freiburg, Freiburg, Germany, 2Department of Cardiology and Angiology, University Medical Center Freiburg, Freiburg, Germany, 3Fraunhofer MEVIS, Bremen, Germany
Synopsis
Our purpose was to quantify regional stiffness in the aorta in stroke patients using 4D flow MRI based pulse-wave-velocity quantification in comparison with stiffness quantification using parameters based on transesophageal echocardiography (TEE). MRI and TEE based stiffness parameters were highly correlated and increased stiffness as measured using 4D flow MRI and TEE was associated with presence of atherosclerosis. Accordingly, we were able to predict the presence of atherosclerotic lesions with high sensitivity and specificity using both, 4D flow MRI and TEE. Hence, especially non-invasive 4D flow MRI can be used in future longitudinal studies investigating early development of atherosclerotic lesions.
INTRODUCTION
Atherosclerosis is the leading cause of cardiovascular disease and the most important driving force of morbidity and mortality in the Western world1. It begins in childhood and remains subclinical for decades2 until symptomatic cardiovascular disease (i.e. coronary heart disease, stroke, peripheral artery disease) develops in mid-age. Arterial stiffness has been suggested as a parameter of early and subclinical atherosclerotic disease. Accordingly, quantification of arterial stiffness may be used as a screening tool to identify subjects at risk of clinical atherosclerosis in which profound lifestyle changes and/or medical therapy can be initiated to hinder disease progression. We sought to evaluate non-invasive 4D flow MRI based calculation of regional pulse wave velocity (PWV) in comparison with transesophageal echocardiography (TEE) based parameters of vascular stiffness (distensibility coefficient, stiffness index, strain) to evaluate its potential to predict the presence of early atherosclerosis.METHODS
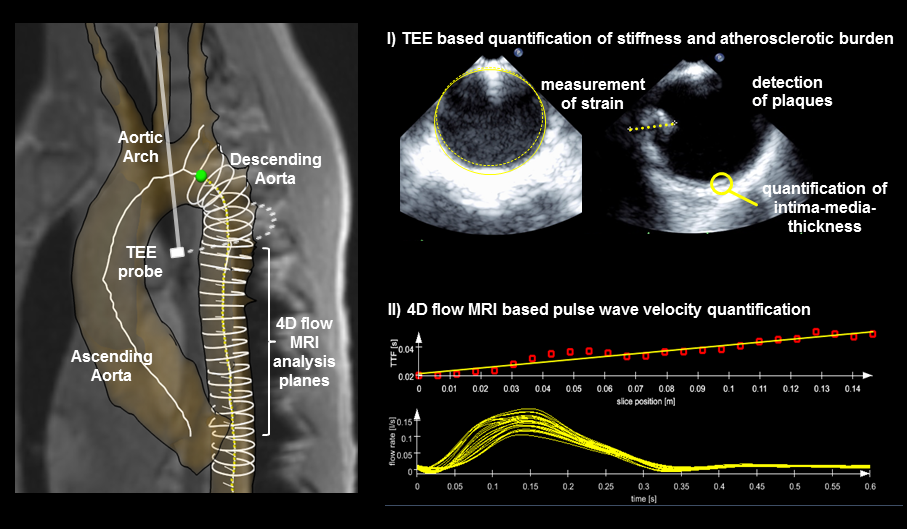
Forty-eight patients undergoing TEE as part of the diagnostic workup of acute ischemic stroke were included in our study. All patients underwent additional 4D flow MRI of the aorta. Intima-media-thickness (IMT) was measured in the descending aorta and the aorta was scrutinized for atherosclerotic plaques using TEE. The degree of atherosclerotic burden was classified as follows: I) no sign of atherosclerosis, II) IMT-thickening and/or plaques <4mm, and III) plaques ≥4mm. The following parameters of vascular stiffness were calculated in the descending aorta using TEE: arterial strain, stiffness index, and distensibility coefficient. Using 4D flow MRI, 25 emitter planes were positioned in the descending aorta and pulse wave velocity was quantified by assessing the temporal evolution of blood flow for each analysis plane using dedicated software (MEVISFlow, Fraunhofer MEVIS, Bremen, Germany). To guarantee comparability of the results between different subjects, an initial plane #0 was positioned directly distal to the outlet of the left subclavian artery. PWV was derived from the data by automatically identifying the time to foot (TTF) of the flow waveform. Pearson correlation analysis was performed to quantify the association between parameters of stiffness and IMT. Analysis of variance (ANOVA) was used to quantify differences in stiffness between different degrees of atherosclerotic burden. Furthermore, multivariate regression based on predefined models was used to predict the presence of atherosclerosis and Receiver-Operator-Characteristic (ROC) curves were calculated to determine a cutoff-value for detection of atherosclerosis using MRI-based PWV and TEE-based stiffness index.RESULTS
Mean IMT was 1.43 ±1.75, 7 (14.6%) subjects had no sign of atherosclerosis, 10 (20.8%) had IMT-thickening or plaques <4mm, and 31 (66.7%) had at least one large and/or complex plaque in the aorta as a sign of advanced atherosclerosis. IMT correlated with increased pulse-wave-velocity (r=0.66; p<0.001), decreased distensibility coefficient (r=0.57, p<0.001), increased stiffness index (r=0.64; p<0.001) and decreased strain (r=0.57; p<0.001). When comparing parameters of stiffness in patients with different degree of atherosclerosis we detected a significant difference between patients with no sign of atherosclerosis and patients with presence of atherosclerosis. However, there was no difference between patients with IMT-thickening and/or plaques <4mm and patients with plaques ≥4mm. A multivariate regression model based solely on TEE parameters of stiffness was able to account for 45% (adjusted R²=0.45) of the variance in intima media thickness, which is the same magnitude as a regression model based on 4D flow MRI derived PWV (adjusted R²=0.44). A Receiver-Operator-Characteristic (ROC) curve analysis was performed using stiffness index and PWV values and revealed an area under the curve of 0.89 (p<0.001) and 0.91 (p<0.001), respectively. Accordingly, cutoff values were determined for stiffness index (cutoff=6.58, sensitivity=0.83, specificity=0.80, positive predictive value (PPV)=0.83, negative predictive value (NPV)=0.80) and PWV (cutoff value=7.09, sensitivity=0.90, specificity=0.80, PPV=0.94, NPV=0.71).DISCUSSION
We have shown that parameters of aortic stiffness can be equally assessed using non-invasive 4D flow MRI and semi-invasive TEE. Increased stiffness as measured using 4D flow MRI and TEE was associated with presence of atherosclerosis, but subgroup analysis revealed no difference between early and advanced atherosclerosis. Furthermore, we were able to predict presence of atherosclerotic lesions with high sensitivity and specificity using both, 4D flow MRI and TEE.CONCLUSION
Non-invasive 4D flow MRI can be used in future longitudinal studies investigating early development of atherosclerotic lesions which may guide early intervention and hinder progression to symptomatic atherosclerotic disease.Acknowledgements
No acknowledgement found.References
1. Mozaffarian D., Benjamin EJ., Go AS., et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation 2016;133(4):e38–360.
2. Strong JP., Malcom GT., McMahan CA., et al. Prevalence and extent of atherosclerosis in adolescents and young adults: implications for prevention from the Pathobiological Determinants of Atherosclerosis in Youth Study. JAMA 1999;281(8):727–35.
Figures