0276
Characteristics of Morphology, Compositions and Distribution of Carotid Artery Atherosclerotic Plaques in Asymptomatic Elderly Population: A Three-Dimensional, Multicontrast Magnetic Resonance Vessel Wall Imaging Study1Department of Radiology, Yangzhou First People’s Hospital, Yangzhou, People's Republic of China, 2Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University, Beijing, People's Republic of China, 3Department of Radiology, University of Washington, Seattle, United States, 4Department of Radiology, Zhongda Hospital, Medical School of Southeast University, Nanjing, People's Republic of China
Synopsis
This study investigated the morphology, compositions and distribution of carotid artery atherosclerotic plaques in asymptomatic elderly population using 3D multicontrast MR vessel wall imaging. The atherosclerotic plaques were found to be prevalent (62.1%) and more than 12% subjects had high risk plaques (HRP) in this study population. Among carotid arteries without luminal stenosis, the prevalence of plaque and HRP was 43.2% and 8.3%, respectively. Benefiting from the 3D vessel wall imaging with large longitudinal coverage, near 14% of subjects had plaques in either distal ICA or proximal CCA segment which cannot be captured by traditional 2D vessel wall imaging.
Introduction
It is well established that carotid high risk atherosclerotic plaque (HRP) is one of the major causes of ischemic stroke [1]. Ultrasound studies revealed that subclinical atherosclerosis can be frequently seen in the elderly subjects [2]. However, the prevalence and distribution of high risk plaques in extracranial carotid arteries are less evidenced in the elderly population. Previous studies have shown that 2D MR vessel wall imaging is capable of assessing carotid HRP accurately [3]. Apparently, due to limited longitudinal coverage (32 mm), 2D MR vessel wall imaging cannot capture the plaques occurring in more distal segment of internal carotid artery (ICA) or more proximal segment of common carotid artery (CCA). Recently, three dimensional (3D) MRI techniques, such as motion sensitized driven equilibrium prepared rapid gradient echo (MERGE) and simultaneous non-contrast angiography and intraplaque hemorrhage (SNAP) sequences, have been proposed for characterization of atherosclerotic plaques with large longitudinal coverage (>150 mm) [4].Purpose
This study sought to evaluate the morphology, compositions and distribution of carotid plaques in asymptomatic elderly population using 3D multicontrast MR vessel wall imaging.Methods
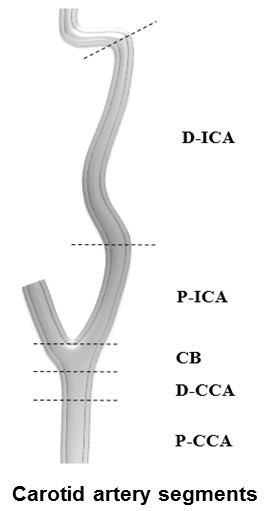
Study sample: Asymptomatic elderly subjects (≥60 years) were recruited from a pilot community study of Cardiovascular Risk of Older Population (CROP). MR imaging: All the carotid arteries were scanned coronally on a 3.0T MR scanner with custom-designed 36-channel neurovascular coil [4]. The MR imaging sequences were acquired using the following parameters: 3D MERGE: fast field echo (FFE), TR/TE 9/4.2 ms, flip angle 6°; 3D SNAP: FFE, TR/TE 10/4.8 ms, flip angle 11°/5°; 3D TOF: FFE, TR/TE 20/4.9 ms, flip angle 20°. All three sequences were acquired with the same field of view of 16x16x4 cm3. The spatial resolution was 0.8x0.8x0.8 mm3 for MERGE and SNAP and 0.6x0.6x2 mm3 for TOF, respectively. Image interpretation and statistical analysis: All MR images were reviewed by two experienced radiologists using custom-designed software with consensus. The morphology of carotid artery including lumen area (LA), wall area (WA), total vessel area (TVA), mean wall thickness (MWT), and normalized wall index (NWI=WA / [LA + WA] x 100%), and stenosis was measured. The presence or absence of plaque, calcification (CA), lipid-rich necrotic core (LRNC), intraplaque hemorrhage (IPH), and HRP (plaques with IPH and/or large LRNC (LRNC area/WA ≥40%) was determined. The plaque distribution was evaluated in the following carotid segments: distal ICA (D-ICA); proximal ICA (P-ICA); carotid bulb (CB); distal CCA (D-CCA); proximal CCA (P-CCA) (Figure 1). The measurements of plaque morphology and compositions between left and right carotid arteries were compared.Results
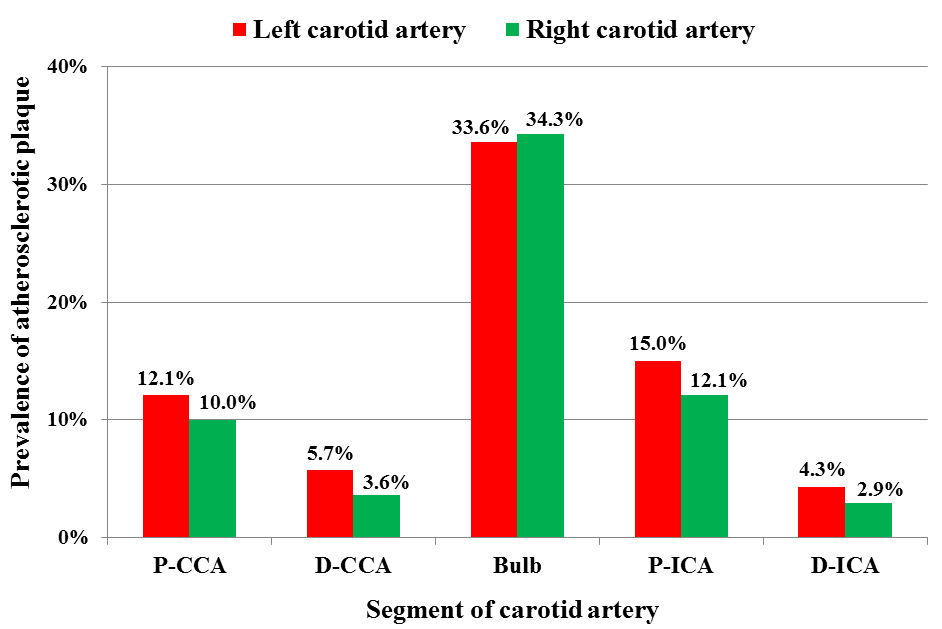
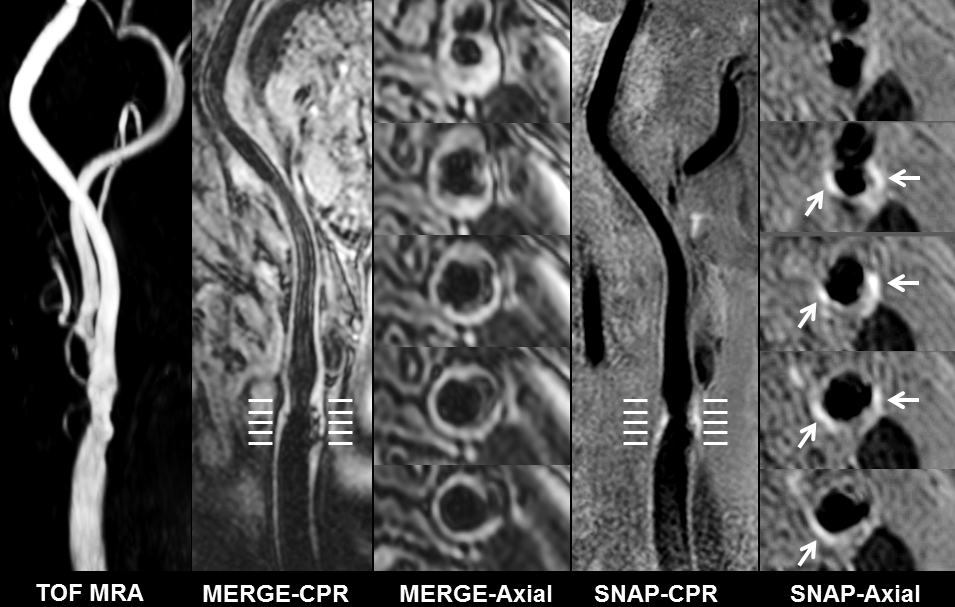
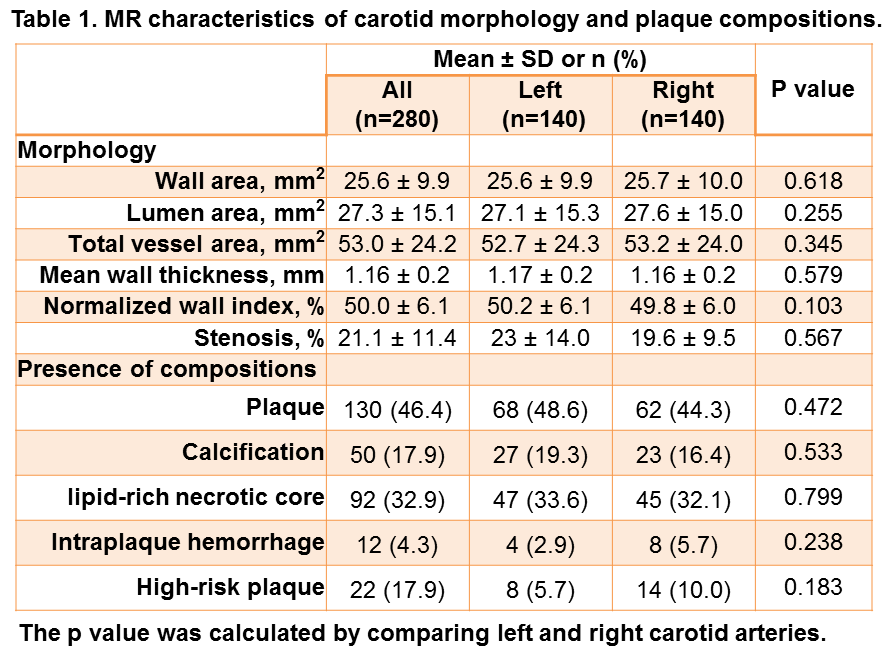
In total, 140 subjects (mean age: 72.1±5.7 years, 63 males) with 280 carotid arteries were recruited and eligible for analysis. Of 140 subjects, 87 (62.1%) had carotid plaques and the prevalence of CA, LRNC, IPH and HRP was 26.4%, 45.0%, 7.9%, and 12.1%, respectively. Of all 280 carotid arteries, 130 (46.4%) had plaques. Carotid plaques were mostly found in the CB segment (33.9%), followed by P-ICA (13.6%), P-CCA (11.1%), D-CCA (4.6%) and D-ICA (3.6%) (Figure 2). There were no statistically differences in all morphological and compositional characteristics of atherosclerotic plaques between left and right carotid arteries (all P>0.05, Table 1). Among carotid arteries without luminal stenosis, the prevalence of plaque and HRP was 43.2% and 8.3%, respectively. Figure 3 is an example of HRP detected by 3D vessel wall imaging in carotid artery with mild stenosis.Discussion
This study investigated the characteristics of morphology, compositions and distribution of carotid artery atherosclerotic plaques in asymptomatic elderly population using 3D multicontrast MR vessel wall imaging. We found the atherosclerotic plaques were prevalent (>60%) and more than 12% subjects had HRPs in this study population. Interestingly, most of detected carotid plaques did not lead to luminal stenosis. Benefiting from the use of 3D vessel wall imaging with large longitudinal coverage, we found that atherosclerotic plaques most likely involved in CB segment and near 14% of subjects had plaques in either distal ICA or proximal CCA segment which cannot be captured by traditional 2D vessel wall imaging techniques. Our findings suggest the necessity of detection of carotid atherosclerotic plaques, particularly the high risk plaques, in asymptomatic elderly population regardless of carotid artery stenosis using 3D vessel wall imaging with large coverage.Conclusion
Carotid artery atherosclerotic plaques are prevalent and a substantial number of high risk plaques can be found in the asymptomatic elderly subjects. The findings of most of detected carotid plaques without luminal stenosis and association between age and multiple carotid plaques suggest the necessity of characterizing atherosclerotic disease regardless of arterial stenosis using MR vessel wall imaging in the elderly.Acknowledgements
None.References
1. Gupta A, Baradaran H, Schweitzer AD, et al. Carotid plaque MRI and stroke risk: a systematic review and meta-analysis. Stroke. 2013;44:3071-7.
2. Sillesen H, Muntendam P, Adourian A, et al. Carotid plaque burden as a measure of subclinical atherosclerosis: comparison with other tests for subclinical arterial disease in the High Risk Plaque BioImage study. JACC Cardiovasc Imaging 2012;5:681-9.
3. Cai JM, Hatsukami TS, Ferguson MS, et al. Classification of human carotid atherosclerotic lesions with in vivo multicontrast magnetic resonance imaging. Circulation. 2002;106:1368-73.
4. Zhou Z, Li R, Zhao X, et al. Evaluation of 3D multi-contrast joint intra- and extracranial vessel wall cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2015;17:41.
Figures