0267
Alterations in brain structural connectivity in comatose cardiac arrest patients1Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Charlestown, MA, United States, 2Department of Neurology, Massachusetts General Hospital, Boston, MA, United States, 3Department of Cardiac Anesthesiology and Critical Care Medicine, Massachusetts General Hospital, Boston, MA, United States, 4Department of Physical Medicine and Rehabilitation, Spaulding Rehabilitation Hospital, Charlestown, MA, United States, 5Department of Medicine, Cardiology Division, Massachusetts General Hospital, Boston, MA, United States, 6Department of Radiology, Massachusetts General Hospital, Boston, MA, United States, 7Department of Neurology, Yale School of Medicine, New Haven, CT, United States
Synopsis
Cardiac arrest patients in coma after restoration of spontaneous circulation were prospectively studied to determine whether variability in structural connectivity can discriminate patients likely to recover consciousness from those who will not. Compared to healthy controls, cardiac arrest patients overall had significantly lower values in the following structural connectivity parameters: global efficiency, clustering coefficient, and degree. Cardiac arrest patients who failed to recover alertness had a significantly lower global clustering coefficient compared to patients who woke up. Alterations in structural connectivity may play an important role in predicting recovery and guiding patient management decisions in comatose cardiac arrest patients.
Introduction
For cardiac arrest (CA) survivors initially comatose after restoration of spontaneous circulation (ROSC), the extent of brain injury and expected neurologic outcome are crucial for patient management decisions.1 Critical knowledge gaps persist in neuroprognostication of comatose post-CA survivors.2 Early prognostication remains difficult except in extreme cases: patients rapidly awakening do well, and those with minimal brain function do poorly. Most CA patients, however, fall between these extremes. Because hypoxic-ischemic injury is typically diffuse, damage to a network of brain regions is likely involved in the patient’s disorder of consciousness. To quantify these complex brain network changes, we applied graph theoretical methods3 that are increasingly being used to understand human brain connectivity in both health and disease.4 Specifically, we investigated global efficiency, degree, and clustering coefficient as a function of arousal recovery (defined here as eye-opening either spontaneously or in response to stimulation).Methods
Cardiac arrest patients who remained comatose after ROSC were prospectively enrolled. Coma was defined as Glasgow Coma Scale (GCS) <=8. Five healthy controls were also enrolled. All subjects underwent 3T MRI scans. High-spatial resolution 3D T1-weighted anatomical images were acquired for registration purposes with FOV=256x256 mm2, acquisition matrix=256x256, 176 sagittal slices (thickness 1 mm). Multiple shell diffusion imaging was acquired using 30 directions with b-values=1000 s/mm2, and 2000 s/mm2 (3x3x3 mm3), and 10 b-value=0 s/mm2 images acquired using blipped simultaneous multi-slice5 echo planar imaging (EPI). Structural probabilistic connectivity maps were calculated using a modification of the FSL probabilistic fiber-tracking algorithm.6, 7 The output was modified such that each voxel represented the probability of diffusion streamlines projecting from any voxel in the seed region-of-interest (ROI) to the voxel of interest rather than number of streamlines. Structural connectivity with respect to each ROI was measured using the average probability of streamlines emanating from the source to target ROIs. Network nodes were defined using the Automated Anatomical Labels atlas.8 Adjacency matrices were computed with a threshold of 10%. Network topology measures were calculated using the Brain Connectivity Toolbox (BCT)9 and compared (one-way analysis of variance, followed by post-hoc Student t-tests). To minimize potential confounding effects from early withdrawal of life sustaining therapy (WLST), we excluded subjects who had WLST before 10 days without arousal recovery.Results
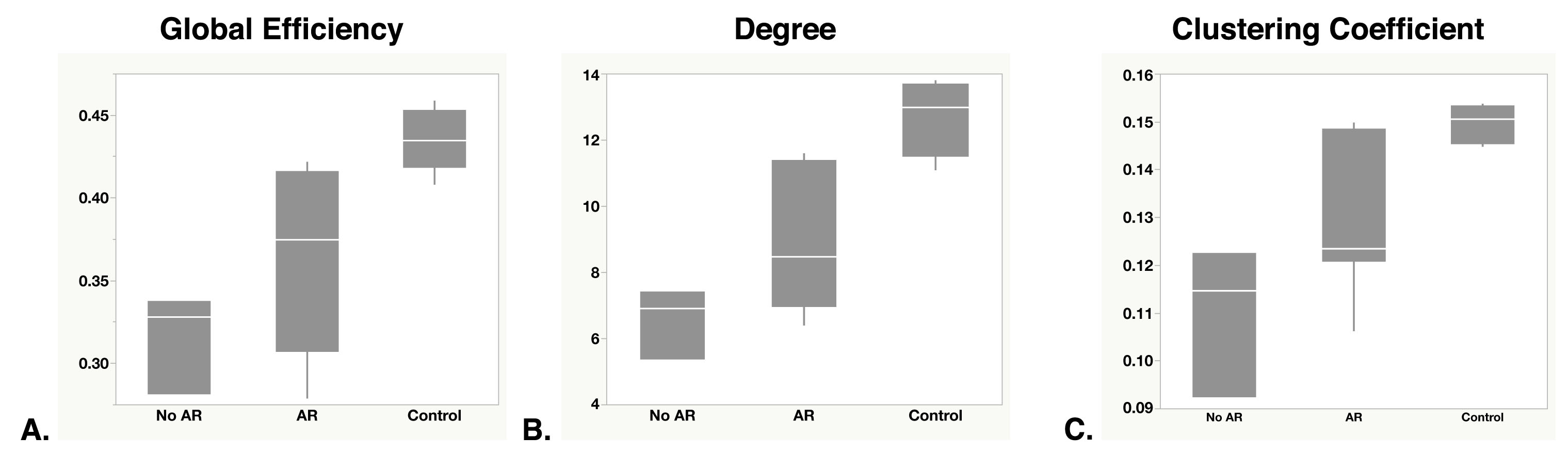
Ten patients (46±26 years old, 40% male) and five controls (37±19 years old, 40% male) were analyzed. Seven patients exhibited arousal recovery (AR), three did not (No AR). Four were alive at discharge, one died from brain death and five died due to WLST. GCS (median [IQR]) was 3 [3-3.75] at admission, and 6.5 [4.5-9] at the time of the research MRI, performed 5.5 [4-8.75] days after initial arrest. Global efficiency, degree, and clustering coefficient (mean±SD) among healthy controls were 0.44±0.02, 12.7±1.16 and 0.15±0.00, respectively, and were lower among patients (AR: 0.36±0.06, 9.1±2.3, 0.13±0.02; No AR: 0.32±0.03, 6.6±1.06, 0.11±0.02). The Figure shows box-plots of the different metrics across the 3 groups. One-way ANOVA found significant differences across the 3 groups for global efficiency (P=0.0061), degree (P=0.0015), and clustering coefficient (P=0.0059). Post-hoc analysis demonstrated the patient group had significantly lower metrics compared to healthy controls (P<0.05), suggesting loss of brain complexity. Compared to patients with AR, found No AR patients demonstrated statistically significantly lower clustering coefficients (P=0.033) and non-statistically significantly lower efficiency (P=0.15) and degree (P=0.066) values.Discussion
Patients who failed to exhibit arousal recovery demonstrated greater disturbances in structural connectivity compared to patients who recovered arousal. These findings suggest that structural connectivity network measures may have utility in identifying patients who may achieve good outcomes, despite presenting with poor initical GCS scores. Differences in timing of MRI acquisition, potential bias from unblinding of clinical MRI sequences to treating clinicians, and small sample sizes are diagnostic limitations of our findings. Although connectivity findings were not available to the clinical team, unblinding of clinical MRI sequences to clinicians was mitigated by excluding patients with early WLST. Future prospective studies will benefit from enrolling subjects whose legally authorized representatives plan to defer WLST decisions for at least two weeks post-arrest in order to more accurately characterize these patients’ likelihood for recovery.Conclusion
Alterations in structural connectivity measured with diffusion MRI show promise in predicting recovery and guiding patient management decisions in comatose cardiac arrest patients.Acknowledgements
We thank Drs. Himanshu Bhat, Dylan Tisdall, Andre van der Kouwe, Kawin Setsompop and Steven Cauley for providing pulse sequences that were used in this study.References
1. Dragancea I, Rundgren M, Englund E, Friberg H, Cronberg T. The influence of induced hypothermia and delayed prognostication on the mode of death after cardiac arrest. Resuscitation. 2013;84:337-342
2. Neumar RW, Shuster M, Callaway CW, Gent LM, Atkins DL, Bhanji F, et al. Part 1: Executive summary: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132:S315-367
3. Albert R, Barabasi AL. Statistical mechanics of complex networks. Rev Mod Phys. 2002;74:47-97
4. Bullmore E, Sporns O. Complex brain networks: Graph theoretical analysis of structural and functional systems. Nature reviews Neuroscience. 2009;10:186-198
5. Setsompop K, Gagoski BA, Polimeni JR, Witzel T, Wedeen VJ, Wald LL. Blipped-controlled aliasing in parallel imaging for simultaneous multislice echo planar imaging with reduced g-factor penalty. Magn Reson Med. 2012;67:1210-1224
6. Behrens TE, Berg HJ, Jbabdi S, Rushworth MF, Woolrich MW. Probabilistic diffusion tractography with multiple fibre orientations: What can we gain? Neuroimage. 2007;34:144-155
7. Jbabdi S, Sotiropoulos SN, Savio AM, Grana M, Behrens TE. Model-based analysis of multishell diffusion MR data for tractography: How to get over fitting problems. Magn Reson Med. 2012;68:1846-1855
8. Tzourio-Mazoyer N, Landeau B, Papathanassiou D, Crivello F, Etard O, Delcroix N, et al. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage. 2002;15:273-289
9. Rubinov M, Sporns O. Complex network measures of brain connectivity: Uses and interpretations. Neuroimage. 2010;52:1059-1069
Figures