0234
High-Resolution, Echo Planar Imaging on a Compact MRI Scanner: Applications in Stroke and Neuroimaging1GE Global Research, Niskayuna, NY, United States, 2Radiology, Mayo Clinic, Rochester, MN, United States
Synopsis
Rapid (six minutes and under) neuroimaging protocols can improve patient throughput and scanner utilization, especially when accelerated using the relatively fast EPI readout. However, susceptibility-related image distortion in EPI has limited its useful spatial resolution (2-2.5mm) conventional, whole-body 3T MRI. A 3.5-fold faster slew-rate head-only gradient on a novel low-cryogen compact 3T scanner can provide an effective platform for twofold-faster EPI that achieves higher spatial resolution (1mm). The utility of rapid (under one minute) single- and multi-shot T2-weighted EPI on the compact 3T is evaluated and compared to routine T2-FSE imaging in patients with brain tumors and stroke.
Clinical Question
Can faster, 1 mm-resolution EPI on a dedicated, high-performance compact 3T MRI scanner provide clinical utility in stroke and neuroimaging in general?Impact
Rapid (≤six minutes) neuroimaging protocols have been proposed1-3, motivated by the large potential impact of increasing patient throughput and scanner utilization. Replacing fast-spin-echo (FSE/TSE) readout with the even faster readout of echo-planar-imaging (EPI) has been one key technique employed in such protocols, especially in stroke imaging2. However, severe susceptibility-induced image distortion in EPI has limited its useful resolution (2-2.5mm) at 3T. EPI distortion in part results from its long echo spacing (ESP), which can be shortened with improved gradient performance, which is determined by gradient system design and peripheral nerve stimulation (PNS) limits. The goal is to improve the clinical feasibility of fast (<one minute), high-resolution (1mm) EPI acquisition for neuroimaging applications (including stroke) at 3T.Approach
As compared to conventional whole-body MRI (Gmax≤80mT/m, SR≤200T/m/s), a compact 3T MRI4 with dedicated, high-performance head-only gradient has 3.5-fold higher gradient slew-rate (Gmax=80mT/m, SR=700T/m/s), allowing twofold reduction in ESP5 without encountering PNS limits6. This in turn provides twofold lower distortion and shorter EPI echotrains that allow more slices per TR interval. The compact 3T uses a conduction-cooled, low-cryogen magnet weighing less than 2,000 kg, has a 0.5mT fringe field (24m2 footprint), requires no vent-stack, and can be transported via forklift and standard freight elevator. Its shorter bore, lower table height and dedicated application for neuroimaging may provide substantial time-savings for patient setup.
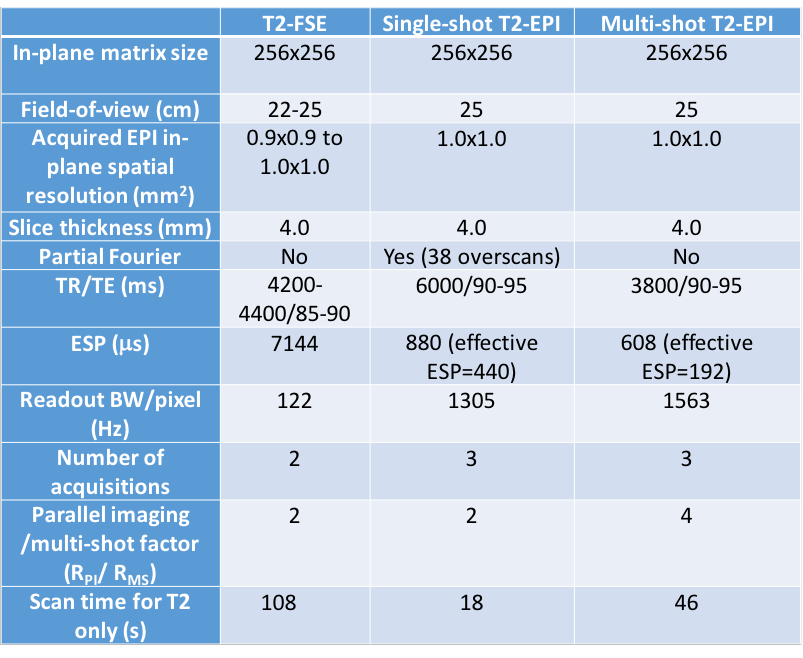
Seven patient subjects (recruited under an IRB-approved protocol) gave informed consent to be imaged on the compact 3T using an 8-channel brain coil. Conventional, fat-saturated, 2D T2-weighted FSE was compared to single-shot T2-EPI as acquired using diffusion-weighted EPI (DW-EPI). Both scans have comparable spatial resolution and contrast (listed in Table 1), but T2-EPI uses 6-fold less time (excluding pre-scan, calibration and diffusion-encoded scans). Parallel imaging (PI) factor of two (RPI=2) was applied to reduce effective ESP by two. A multi-shot (MS) DW-EPI (RMS=4) was also acquired, its T2-EPI requiring 2.3-fold less time than T2-FSE. EPI distortion was corrected with the reversed-polarity-gradient (RPG) method7.
Gains and Losses
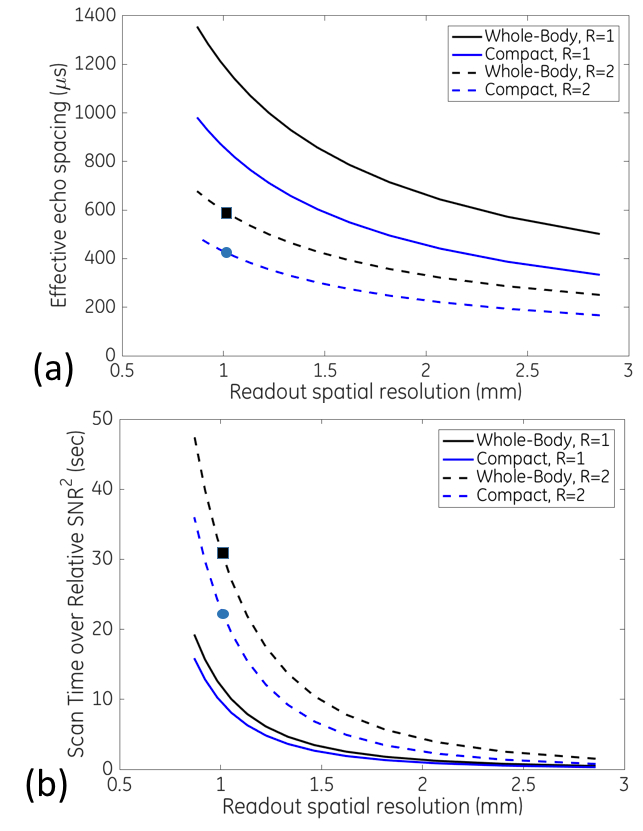
With RPI=2, 2mm-spatial resolution single-shot T2-EPI on whole-body MRI (Gmax=50mT/m, SR=200T/m/s) as a reference for acceptable image quality (distortion and SNR), EPI parameters were generated for imaging at various spatial resolutions on both whole-body and compact scanners (Figure 1). The ESP on the compact 3T was increased to optimize for SNR, keeping effective ESP<450ms at RPI=2. At 1mm, the compact 3T provides both shorter ESP and scan time by 26% and 33% respectively, as compared to whole-body MRI (for the same SNR), excluding gradient heating considerations. The shorter EPI train on the compact 3T explains its higher SNR efficiency. Scanning at RPI=1 at 1mm resolution has twofold higher distortion than RPI=2, but is ~3-fold more SNR-efficient. RPI/RMS=4 has half the distortion of RPI=2, and is~3-fold less efficient than RPI=2 (not shown).
Imaging on the compact 3T is limited to a maximum FOV of 26cm, has increased gradient nonlinearity effects8-9 and requires correction for additional concomitant field terms associated with its asymmetric gradient design10. However, these corrections have now been demonstrated and implemented in routine use, with an additional gradient nonlinearity correction for DWI11.
Preliminary Data
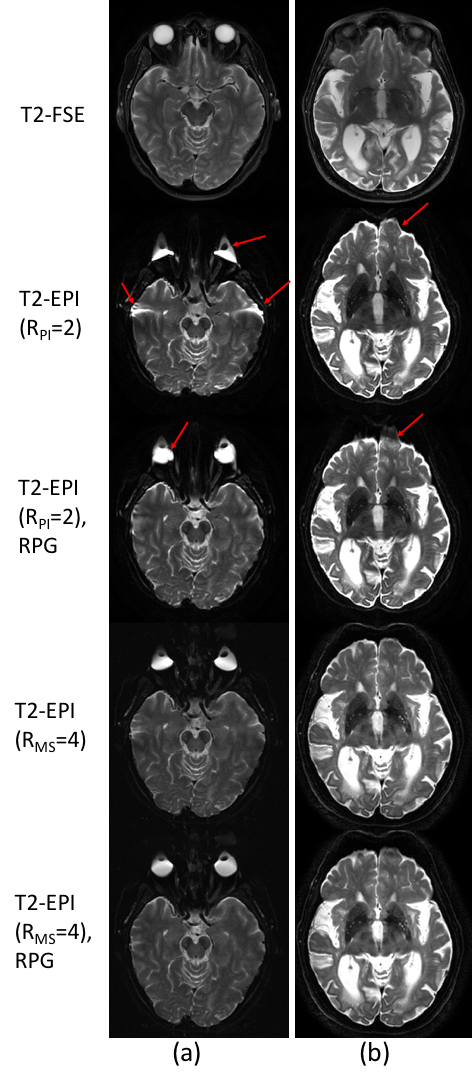
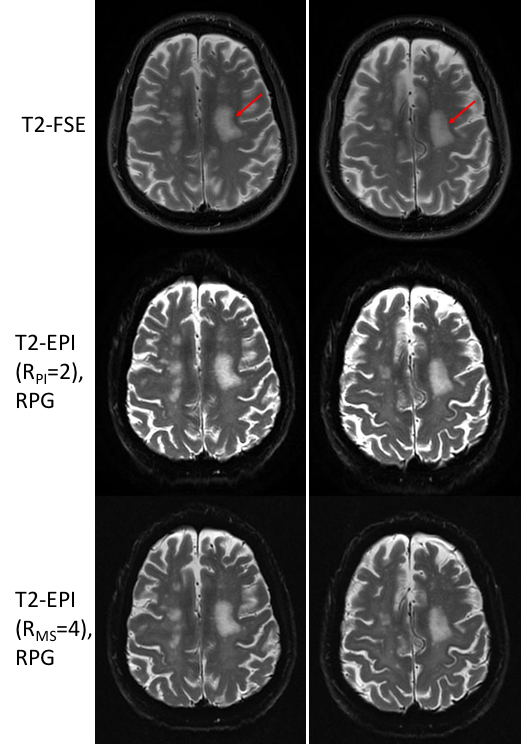
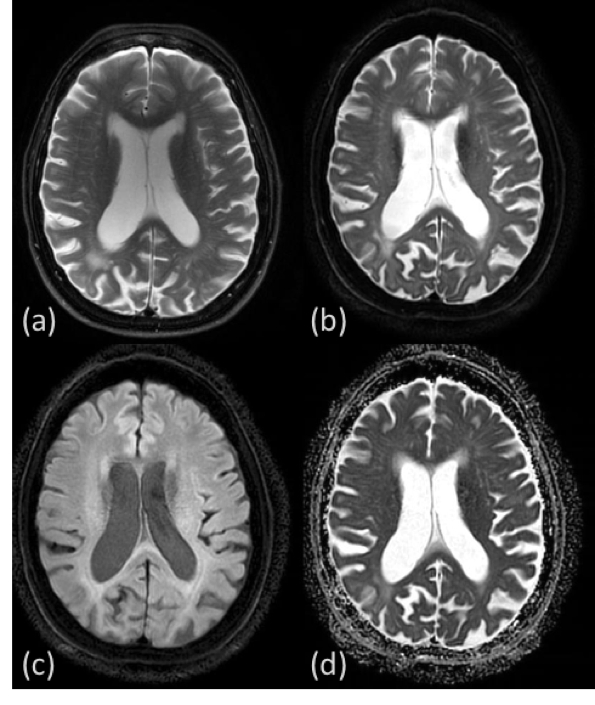
The RPG-measured image distortion in the brain was low in all subjects (95% C.I.=[-5.2, 5.4] pixels). Figure 2 compares T2-FSE images against the T2-EPI scans that still have minor residual distortion and signal dropout in the frontal sinus and skull-base regions, which are reduced with either RPG-correction or multi-shot acquisition. Figure 3 illustrates another comparison showing equivalent conspicuity of the previous stroke between T2-FSE and multi-shot T2-EPI, with some blurring demonstrated in single-shot T2-EPI. Figure 4 shows that multi-shot DWI provides the T2-EPI, as well as trace and ADC maps for an additional minute of scan time compared to that of T2-FSE.
This work compares single-shot (6-fold faster) and multi-shot (2.3-fold faster) T2-EPI to T2-FSE on the compact 3T scanner. Its faster gradients provide EPI acquisition with reduced distortion and higher scan time efficiency. A full clinical comparison is still required to determine the diagnostic value of T2-EPI vs T2-FSE. As compared to T2-FSE, T2-EPI still has minor residual distortion and signal dropout, and require phase-correction in multi-shot EPI. However, the incorporation of iterative multi-shot reconstruction12 and acceleration techniques via simultaneous multi-slice13 may provide further improvements in distortion and scan efficiency. In particular, stroke imaging can benefit from 1mm-resolution DWI, which on its own14 or in combination with very fast EPI-FLAIR2 could potentially improve the efficiency and image quality of stroke imaging.
Acknowledgements
This work was supported in part by NIH R01EB010065. The views herein do not necessarily represent those of NIH. The authors will like to thank Joshua Trzasko, Shengzhen Tao, Giang-Chau Ngo, Arnaud Guidon, Jonathan Sperl and Dominic Graziani for useful discussion.References
1. Boulter DJ, et al. ASNR 2014. Montreal, Canada.
2. Nael K, et al. Stroke, 2014. 45(7)1985-91.
3. Nael K. ISMRM Sunrise Educational Session, ISMRM 2016.
4. Foo TKF, et al. ISMRM 2016. 3629.
5. Tan ET, et al. JMRI 2016. 44(3)653-664.
6. Lee SK, et al. Magn Reson Med 2016. doi: 10.1002/mrm.26044
7. Holland D, et al. Neuroimage 2010. 50(1):175-183.
8. Tan ET, et al. ISMRM 2013. 3216.
9. Tao S, et al. Med Phys 2016;43(6)3725.
10. Tao S, et al. MRM 2016. DOI: 10.1002/mrm.26315
11. Tan ET, et al. JMRI 2012;38(2):448-53.
12. Chu, ML et al. MRM 2015;74(5)1336-48.
13. Setsompop K et al. MRM 2011;67(5)1210-24.
14. Geraldo AF, et al. Stroke 2016. 47(3)877-881.
Figures