0229
Combined 3D Cine/4D Flow Accelerated Cardiac Imaging with Cloud Computing. Toward Streamlined and Fast Comprehensive Cardiac MRI ExamHaonan Wang1, Peng Lai2, Piero Ghedin1, Shreyas S Vasanawala3, Anja C.S Brau2, and El-Sayed Ibrahim1
1GE Healthcare, Waukesha, WI, United States, 2GE Healthcare, Menlo Park, CA, United States, 3Radiology, Stanford University, CA, United States
Synopsis
Currently, cine MRI is the gold standard for evaluating cardiac function. Nevertheless, in today’s practice, slices need to be acquired at different oblique, and 12-16 short-axis slices needs to be acquired for sufficient ventricular coverage. The same limits apply to hemodynamics-related assessment of valvular and vascular performance, for which multiple 2D oblique flow measurements need to be acquired. In this abstract, we present a combined 3D Cine/4D Flow accelerated cardiac imaging technique with cloud computing, which significantly reduces the scan and processing time, reduces the scan’s complexity, alleviates misregistration problems, and increases productivity.
Clinical Question
MRI cine imaging is the gold standard for evaluating cardiac function. Nevertheless, conventional cardiac MRI suffers from limited patient access due to its need of advanced operator skills, breathholding and lengthy scans. In today’s practice, 2D slices needs to be acquired at different oblique views (e.g. short axis, two-and four-chamber long axis, etc) and 12-16 short-axis slices need to be collected with whole ventricular coverage for assessment of functional parameters, e.g. motion and ejection fraction. The associated complicated slice orientation, long scan time and multiple breath-holds compromise the efficiency of the whole cardiac MRI exam. The same limits apply to hemodynamics-related assessment of valvular and vascular performance, for which multiple 2D oblique flow measurements need to be acquired. In addition to the complex scan workflow, a significant amount of time is required for image postprocessing and flow quantification. In this abstract, we present a combined 3D Cine/4D Flow accelerated cardiac imaging technique with cloud computing, a step toward streamlined and fast comprehensive cardiac MRI.Impact
Currently, the cardiac MRI exam protocol takes about 60 minutes to acquire sufficient anatomy and functional images to evaluate the cardiac function. 1 Even with such long acquisition, whole heart coverage is still hard to achieve, resulting in potential overlook of certain pathologies. The combined 3D cine/4D flow MRI workflow could potentially shorten this complex workflow to a 10-minute acquisition with axial whole chest coverage. Based on this single acquisition, anatomy, function, and flow information could be obtained simultaneously with whole volume coverage and capability of arbitrary offline reformatting. This efficient workflow could be applied on a wide spectrum of cardiac diseases, including ischemic heart disease, cardiomyopathies, congenital heart disease, and valvular diseases.Approach
The importance of the developed technique resides in its simplicity, short scan time, and fast inline post-processing. To achieve these goals, innovative techniques are implemented during acquisition, reconstruction, and post-processing. First, conventional 2D cine and PC acquisitions at multiple oblique planes are replaced by a single axial 3D velocity-encoding acquisition that covers the whole heart with isotropic resolution. 2,3 Besides reducing scan time, the new approach eliminates the need for prescribing several cardiac-specific anatomical planes and allows for reconstructing planes with arbitrary orientation during postprocessing. Second, the scan is accelerated using variable density k-t acceleration and motion is suppressed using an acquisition-efficient method with signal averaging at central k-space. In reconstruction, kat ARC, a spatiotemporal-correlation-based autocalibrating parallel imaging method with motion-adaptive temporal window selection, is applied. 4,5 Also, a static tissue removal method is used to eliminate chest wall signal before kat ARC unaliasing to reduce residual artifacts at high acceleration. The advanced sampling scheme and reconstruction technique combined provides a high acceleration factor of 8 such that a whole heart coverage could be achieved in as fast as sub 8-minute free-breathing scan. 6 Finally, the generated huge amount of images (~ 20GB) is processed on the cloud with GPU processing for real-time visualization and analysis of both function and flow information. The powerful online platform could provide automatic segmentation, flow quantification, and a variety of visualization options, including flow streamline tracing, flow vectors, and color-coded velocity map. The processed data is then displayed superimposed on the anatomical images, where the operator has the option of interactively changing the display orientation, visualization method, and generated parameters. To evaluated the proposed method, 20 pediatric subjects were scanned on GE 3T (MR750) using 32-channel cardiac coil with intravenous Ferumoxytol. Imaging parameters were: 2x2mm2 in plane resolution and 2 mm slice thickness. Typical temporal resolution is about 60ms for a heart rate of 60 beats/min.Gains and Losses
The main advantage of presented technique is its capability of simultaneously providing both functional and hemodynamic information about the cardiovascular system with significant reduction in scan and processing time. The 3D cine (magnitude) images are used to measure various global, e.g. ejection fraction, and regional, e.g. strain (using feature tracking techniques), functional parameters, while the velocity-encoded phase images are used to measure various hemodynamic parameters, e.g. flow volume, velocity, regurgitation rate, and different flow timings. The capability of analyzing the results while the patient is still on the table allows for addressing patient-specific questions and adding necessary imaging sequences as needed based on a case-by-case scenario. The significant reduction in scan time and lack of breath-holding makes the cardiac MRI exam more tolerable to the patient and accessible to a wider group of patients, including those who are not able to hold their breath. Finally, the reduced exam time would help reduce exam cost and improve productivity in general.Acknowledgements
No acknowledgement found.References
[1] Kramer C, JCMR 2013; [2] Pelc NJ, MRQ 1991; [3] Markl M, JMRI 2007; [4] Lai P, ISMRM 2009; [5] Lai P, ISMRM 2014; [6] Lai P, JCMR 2015Figures
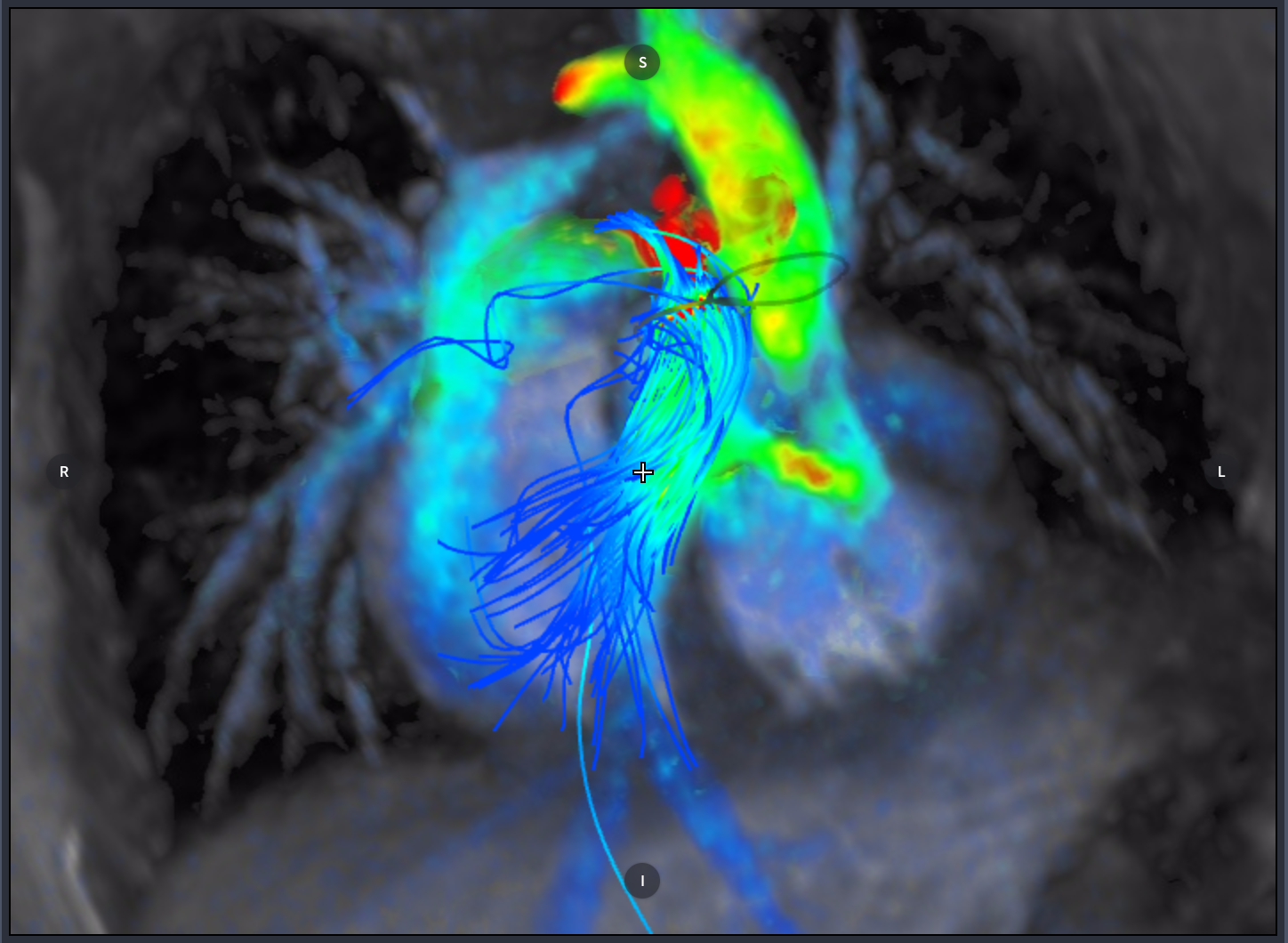
Figure 1. This figure shows the main pulmonary artery (MPA) streamlines and stenosis at the bifurcation (color coded in red). The figure also shows the ventricular septal defect (VSD).
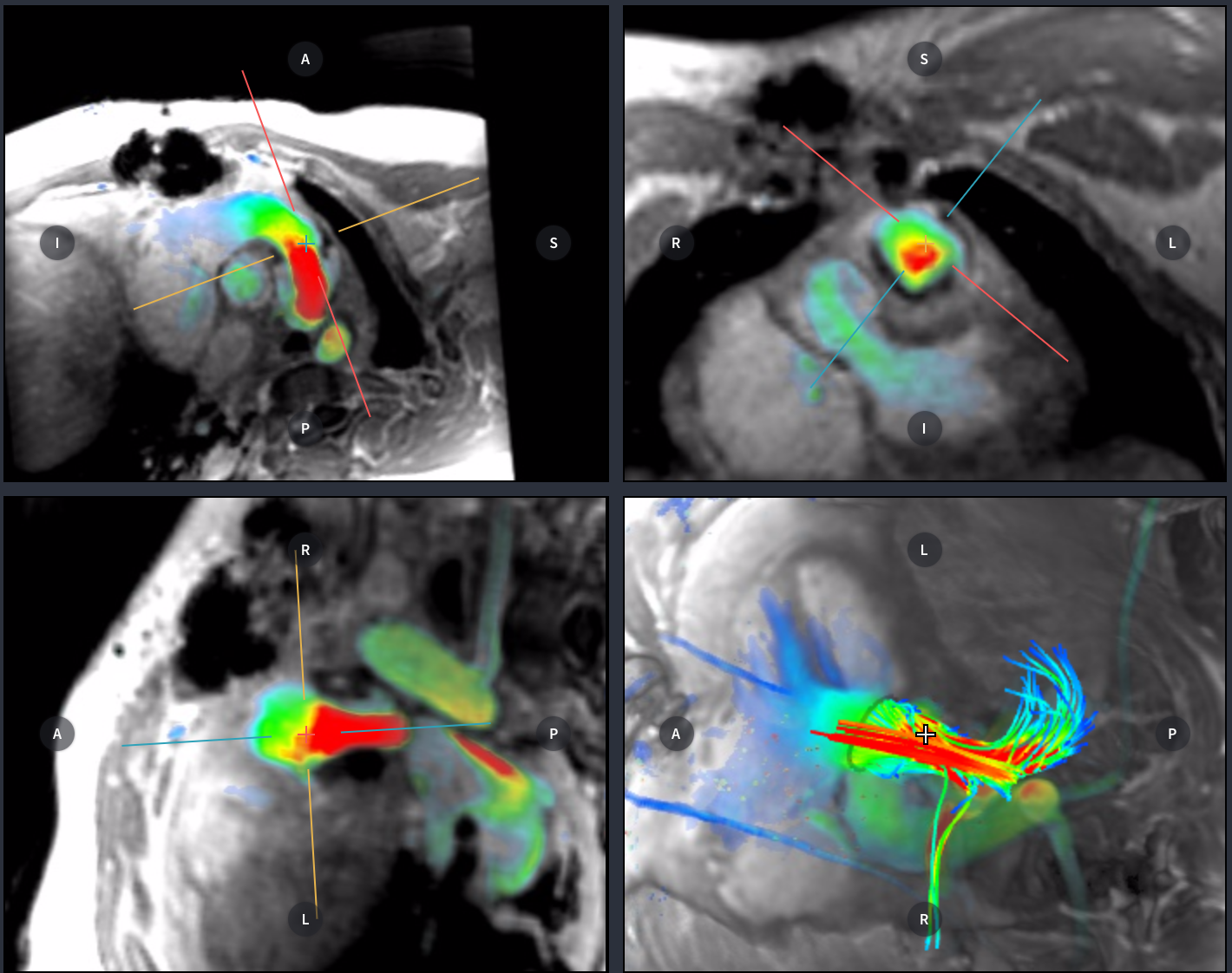
Figure 2. This figure shows a case of complex congenital heart malformation. The main pulmonary artery shows significant stenosis with consequent high accelerated flow pattern represented in red on color-coded velocity image and by the streamlines.