0223
Optimizing MRI for Focal Liver Lesions: Are All Our Sequences Really Necessary?1Department of Radiology, Case Western Reserve University, Department of Radiology, Cleveland, OH, United States, 2Department of Radiology, University hospitals Cleveland medical center, Cleveland, OH, United States, 3University Hospitals Cleveland Medical Center, Cleveland, OH, United States, 4Case Western University
Synopsis
In this proof-of-concept study, our aim was to determine an optimal minimum number of MRI sequences which allow confident characterization of liver lesions into benign versus malignant categories with reasonable accuracy. We hypothesized that an abbreviated liver MRI protocol including single shot T2-weighted, pre and dynamic post-contrast T1-weighted images has the potential to reduce overall scan time and throughput. If this can be performed without significant loss in diagnostic accuracy it may improve efficacy and be beneficial to current practice.
Clinical Question
What is the minimum number of MRI sequences required for accurately characterizing focal liver lesions?Impact
Abdominal MRI is a powerful tool for evaluating focal liver lesions (FLL), but is also recognized to be very lengthy due to the complexity of protocols containing several sequences. Over the past years, the improvements in speed and quality of imaging have been utilized to add extra sequences to the protocols rather than reducing the scan duration. While these sequences served the purpose of increasing the diagnostic accuracy, they might not always be necessary for characterization of FLL; in fact, in some cases they may lead to confusion and decrease diagnostic accuracy. Furthermore, prolonged imaging can result in patient anxiety and dissatisfaction, high institutional costs and increased interpretation time for the radiologists 1. Therefore, when using expensive diagnostic modalities such as MRI, it might be reasonable to optimize imaging protocols with shortened acquisition time, while maintaining the diagnostic accuracy.Approach
In this proof-of-concept study, our aim is to determine an optimal minimum number of MRI sequences which allow confident characterization of liver lesions into benign versus malignant categories with reasonable accuracy. We started with the postulate that the single shot T2-weighted images along with the pre and dynamic post contrast 3D T1- weighted fat saturated gradient echo sequences represent the core of a liver MR examination. We hypothesized that other sequences, such as T2-weighted fat saturated, diffusion weighted (DWI), in and opposed phase T1-weighted gradient echo images add only marginally to the diagnostic accuracy of a standard liver examination. In this retrospective study, 2 board-certified radiologists with 15 years (reader 1) and 5 years (reader 2) of experience in abdominal MR imaging, evaluated 62 FLL (20 metastases, 13 hepatocellular carcinomas, 1 adenoma, 3 Cholangiocellular carcinomas, 2 mixed HCC and CCCs, 4 lymphoma; 11 hemangioma, 5 focal nodular hyperplasias, 2 abscesses, 1 regenerative nodule) in 60 patients who underwent an abdominal MRI in our institution. Reference standard for the diagnosis was histopathology in 43 lesions and typical imaging features in 19 lesions as determined in consensus by 2 independent experienced radiologists. In a first session, each reader characterized the lesions as benign or malignant according to a 5 point rating scale (1. definitely benign, 2. most likely benign, 3. indeterminate, 4. most likely malignant, 5. definitely malignant) based on the abbreviated liver protocol (aMRI) and also reported their most probable diagnosis. Additionally, observers were asked to indicate if they require any additional sequence for better characterization or increased confidence and which they prefer. In a second session at 4-weeks interval, observers repeated the same analysis followed by a reassessment including DWI and the requested added imaging sequences.Gains and Losses
In our experience, T2-w, pre and dynamic post contrast T1-w images are the key to characterize liver lesions with MRI. While DWI has proven useful to improve lesion detection, the added value from DWI and T2-weighted fat saturated images to characterize and distinguish benign and malignant FLL is controversial2,3,4 . Understanding in which clinical scenario these sequences have significant impact on the diagnosis may help to better tailor protocols to the clinical needs and allow for time savings. The presented abbreviated protocol has the potential to reduce overall scan time and throughput. If this can be performed without significant loss in diagnostic accuracy it may improve efficacy and be beneficial to current practice despite a potential number of recalls in individual cases.Preliminary data
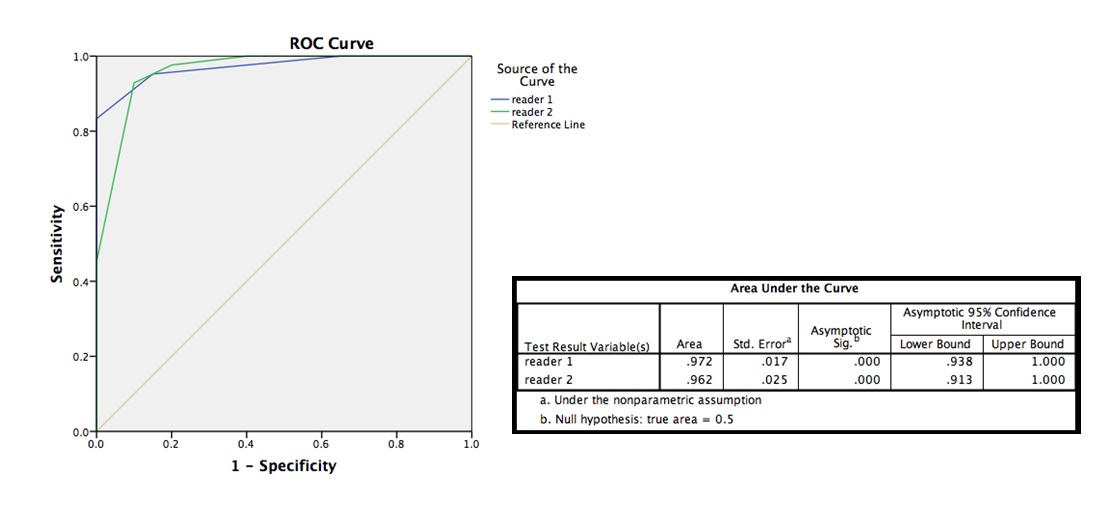
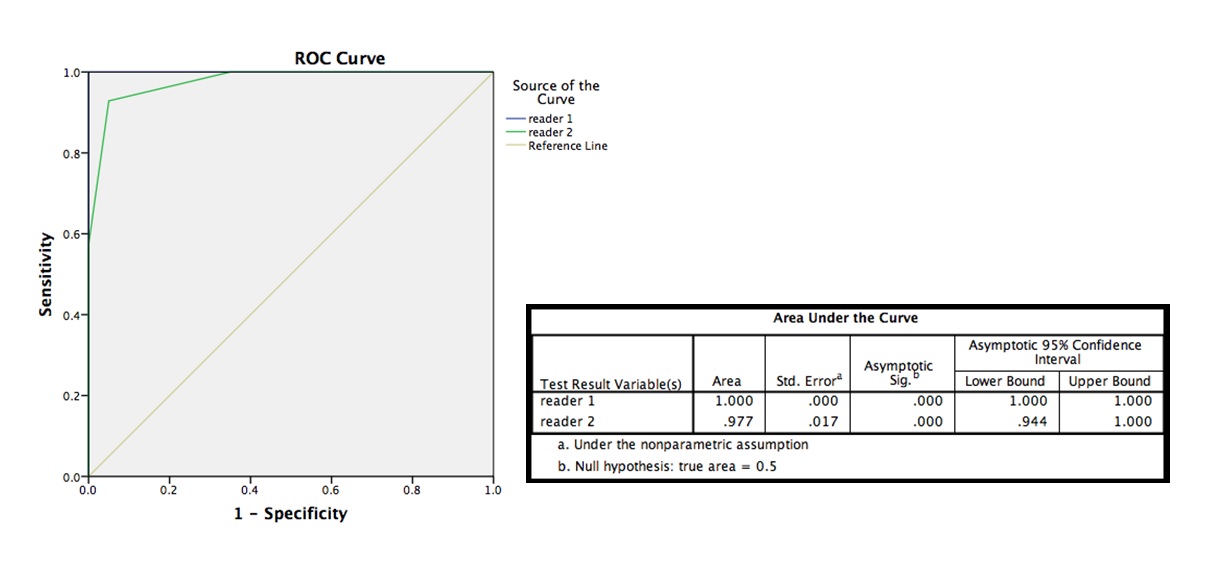
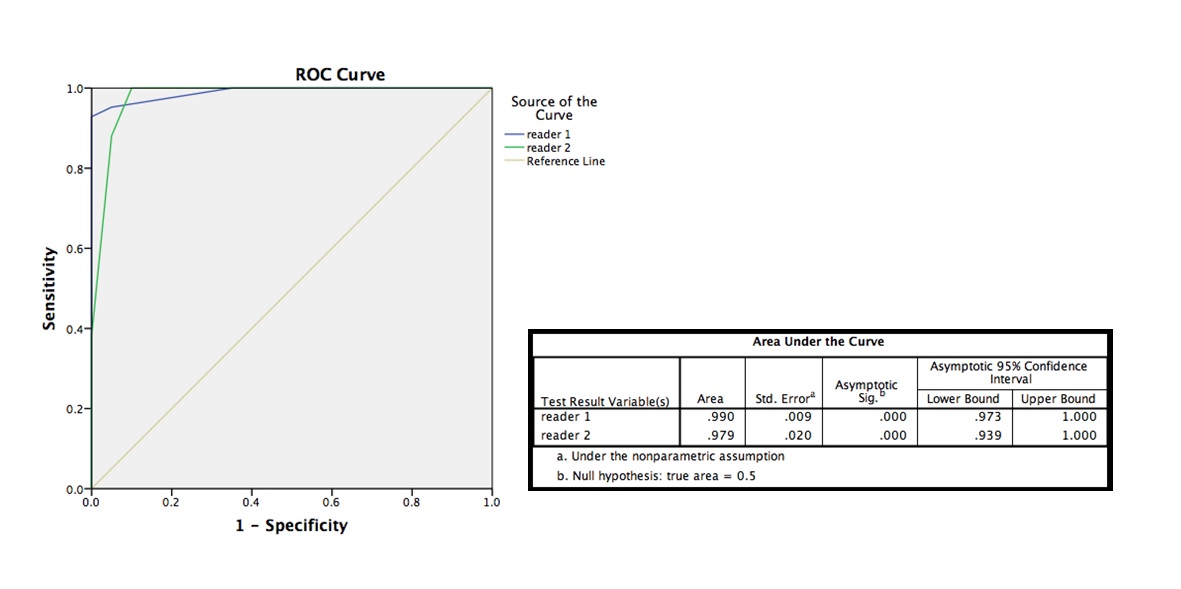
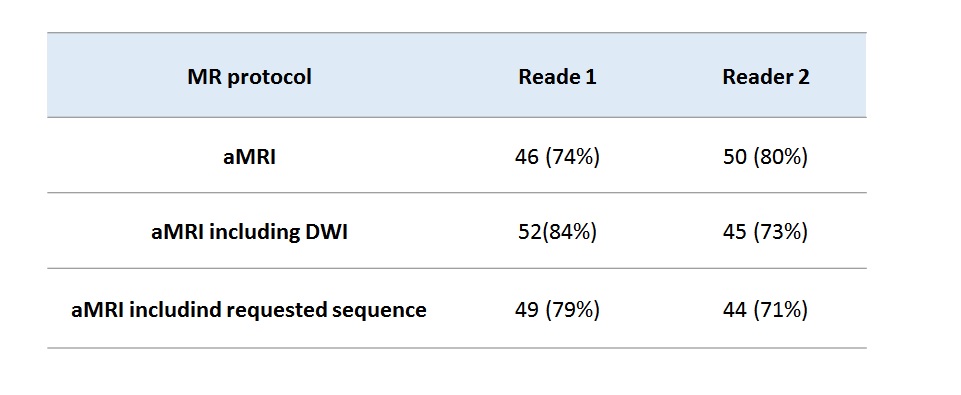
The results of a ROC analysis for both readers to distinguish benign and malignant lesions using aMRI protocol are shown in figure 1. Areas under the curve (AUC) were 0.97 and 0.96 for reader 1 and 2 respectively.The Cohen’s Kappa coefficient for inter-observer agreement was 0.78 (P.value<0.001). Additional sequences were requested for 24/62 (38%) and 39/62 (63%) lesions, respectively. DWI was requested in 54% and 61% of these cases. The effect of added DWI and requested sequences on lesion characterization is shown in figures 2 and 3 demonstrating improvement in one reader and less correct choices in the other. Based on aMRI, tissue diagnosis was correct for 46 (74%) and 50 (80%) lesions, respectively. The impact of DWI and added sequences on correct tissue diagnosis is shown in table 1. The number of correct tissue diagnosis increased with DWI for reader 1 but decreased for reader 2. These results suggest that initial diagnostic accuracy with aMRI is very high and comparable to references5. Adding DWI or other sequences may improve overall performance but also carries the risk of inducing less diagnostic confidence, conflicting information and decreased accuracy.Acknowledgements
No acknowledgement found.References
1- Schreiber-Zinaman J, Rosenkrantz AB, Frequency and reasons for extra sequences in clinical abdominal MRI examinations Abdom Radiol (2016). doi:10.1007/s00261-016-0877-6
2- Hussain HK, Syed I, Nghiem HV, et al. T2-weighted MR imaging in the assessment of cirrhotic liver. Radiology 2004; 230:637-644.
3- Goshima S, Kanematsu M, Kondo H, et al. Diffusion-weighted imaging of the liver: optimizing b value for the detection and characterization of benign and malignant hepatic lesions. J Magn Reson Imaging. 2008 Sep;28(3):691-7.
4- Yang DM, Jahng GH, Kim HC, et al. The detection and discrimination of malignant and benign focal hepatic lesions: T2 weighted vs diffusion-weighted MRI. The British Journal of Radiology. 2011;84(1000):319-326. doi:10.1259/bjr/50130643.
5- Morana G, Grazioli L, Kirchin MA, et al. Solid hypervascular liver lesions: accurate identification of true benign lesions on enhanced dynamic and hepatobiliary phase magnetic resonance imaging after gadobenate dimeglumine administration. Invest Radiol 2011;46:225-239
Figures