0148
Effective collateral circulation may related with better perfusion restoration after carotid endarterectomy (CEA): a pilot territory ASL (tASL) study1Radiology, Peking Union Medical College Hospital, Beijing, People's Republic of China, 2Vascular surgery, Peking Union Medical College Hospital, Beijing, People's Republic of China, 3GE Healthcare, MR Research China, Beijing, Beijing, People's Republic of China
Synopsis
Flow territories normalization was observed in patients underwent carotid endarterectomy (CEA). To investigate whether collateral flow associated with the redistribution of blood we performed 3D ASL and tASL on 25 patients prior to (PRE) and after (POST) surgery. Collateral flow was read as the presence of arterial transit artifact (ATA) on 3D ASL images. Alteration of flow territories was determined by comparing the PRE and POST tASL images. Our study demonstrated that good collateral compensation shown in ASL was associated with normalization of tASL flow territories after CEA.
Purpose
During the carotid endarterectomy (CEA) procedure, the internal carotid artery (ICA) would be clamped. While the ICA is being clamped, the ipsilateral brain is at risk of ischemia. The cerebral perfusion at the clamping side would be solely supplied by collateral flow, if no carotid shunt is placed during the cross-clamping procedure. Inadequate formation of collateral circulation might be associated with cognitive dysfunction after surgery1. Hence the evaluation of collateral circulation prior to surgical procedure is of significant clinical interest. It is known that healthy people feature a probabilistic perfusion territorial map2. The perfusion territories corresponding to different arteries may alter in carotid stenosis patients, and normalization of perfusion territories has been observed after CEA3, which offered a novel parameter to evaluate the outcome of carotid surgery. However, the level of perfusion territory normalization (i.e. to what extent it returns to the probabilistic map of healthy group) alters case by case. In this study, territorial ASL is used to investigate whether the normalization level is correlated with preoperative collateral circulation in patients with carotid stenosis.Method
Twenty-five patients (17 men and 8 women, mean age, 63.5 years, range, 51-81 years) with severe carotid stenosis (70%-99%) diagnosed by CT angiography (CTA), and underwent CEA were enrolled in this retrospective study. The patients received 3D arterial spin labeling (3D ASL) and territory arterial spin labeling (tASL) 4 with a post labeling delay (PLD) time of 2025ms within one-week prior surgery (PRE) and within five days after endarterectomy (CEA) (POST). Two neuro-radiologists, both with extensive experience in clinical ASL imaging, scored collateral flow on PRE 3D ASL images based on the presence of arterial transit artifact (ATA) according to Zaharchuk’s method5. The tASL images were stratified according to the variant of circle of Willis. The post-surgical flow territories were considered as normalized if it conformed to the established probabilistic map of flow territories in healthy population by visual evaluation2. The PRE and POST images were evaluated at separate times in a random blinded fashion. Disagreements were resolved by consensus. The relationship between the whole brain ASL collateral flow score and territories completely normalized or not was evaluated using Mann-Whitney U test.Results
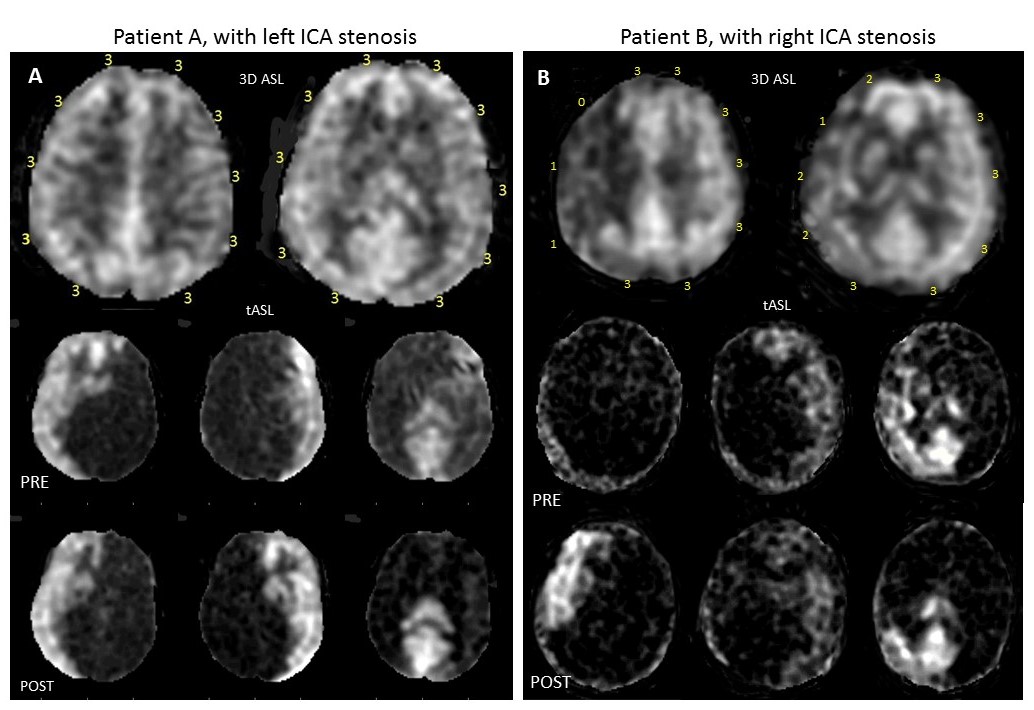
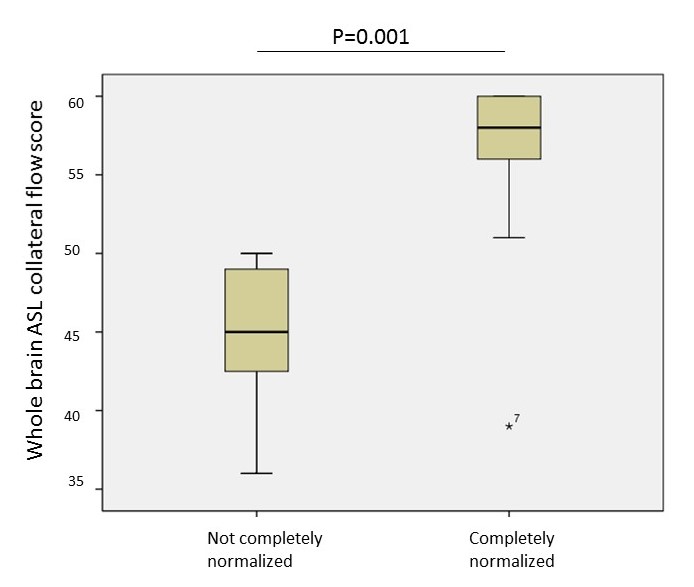
Out of the 25 subjects, completely normalization of tASL flow territories after CEA was observed in 18 cases, whereas 7 patients showed no completely normalization. Two cases, patient A with complete normalization and patient B with insufficient normalization of the perfusion territories after surgery, are shown in Fig.1. It is seen that patient A, who featured high pre-surgical collateral score, showed obvious compensatory circulation in RICA prior to surgery and high level of perfusion territory normalization after surgical operation; on the other hand, patient B featured low pre-surgical collateral score prior to surgery, correspondingly a low level of normalization was seen after surgical operation. Fig.2 displays that a high ASL collateral score in preoperative imaging was significantly associated with normalization of flow territories in tASL images after surgery (P=0.001).Discussion and conclusion
Several studies have investigated the pre-surgical collateral circulation and its relationship with intraoperative ischemia 6,7. The late arriving collateral flow that appears as serpiginous high signal within cortical vessel in ASL perfusion, termed as ATA, can be used to assess the presence of collateral flow prior to surgery. However, previous methods such as electroencephalography (EEG) only monitored perfusion condition during the surgical procedure and no direct biomarker was used to assess the perfusion level after surgery. In this study, tASL offering vessel specific perfusion map was used to assess the perfusion condition after CEA. It was seen that the level of perfusion restoration varied though the stenotic ICA recanalized completely in all cases enrolled, and the level of normalization was strongly correlated with the pre-surgery collateral level, indicating that efficient collateral circulation may associated with better outcome of carotid surgery. In the next stage of this study, the level of perfusion normalization shall be investigated with respected to the level of cognitive function changes. And voxel-based analysis shall be used to determine the extent of flow territories change more accurately.Acknowledgements
No acknowledgement found.References
1.Sussman, E. S. et al. Radiographic absence of the posterior communicating arteries and the prediction of cognitive dysfunction after carotid endarterectomy. Journal of neurosurgery 121, 593-598, doi:10.3171/2014.5.jns131736 (2014).
2.van Laar, P. J. et al. In vivo flow territory mapping of major brain feeding arteries. NeuroImage 29, 136-144, doi:10.1016/j.neuroimage.2005.07.011 (2006).
3.Van Laar, P. J. et al. Altered flow territories after carotid stenting and carotid endarterectomy. Journal of vascular surgery 45, 1155-1161, doi:10.1016/j.jvs.2006.11.067 (2007).
4.Wong, E. C. Vessel-encoded arterial spin-labeling using pseudocontinuous tagging. Magnetic resonance in medicine 58, 1086-1091, doi:10.1002/mrm.21293 (2007).
5.Zaharchuk, G. et al. Arterial spin-labeling MRI can identify the presence and intensity of collateral perfusion in patients with moyamoya disease. Stroke; a journal of cerebral circulation 42, 2485-2491, doi:10.1161/strokeaha.111.616466 (2011).
6. Bagan, P., Azorin, J., Salama, J. & Dumas, J. L. The value of phase-contrast magnetic resonance angiography of the circle of Willis in predicting cerebral ischemia-hypoxia (shunt need) during carotid endarterectomy. Surgical and radiologic anatomy : SRA 27, 544-547, doi:10.1007/s00276-005-0032-5 (2005).
7.Schwartz, R. B. et al. The value of cerebral angiography in predicting cerebral ischemia during carotid endarterectomy. AJR. American journal of roentgenology 159, 1057-1061, doi:10.2214/ajr.159.5.1414775 (1992)
8.Barber, P. A., Demchuk, A. M., Zhang, J. & Buchan, A. M. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet (London, England) 355, 1670-1674 (2000).
Figures