0103
In-utero non-contrast MR angiography of the fetal vasculature using a double-echo radial sampling scheme1Biomedical Engineering, Wayne State University, Detroit, MI, United States, 2Radiology, Wayne State University, Detroit, MI, United States, 3Obstetrics and Gynecology, Wayne State University, Detroit, MI, United States, 4Perinatology Research Branch, NICHD/NIH/DHHS, Detroit, MI, United States
Synopsis
To show that the isotropic gradient delay issue can be addressed by a simple shift of the
Introduction
Recent studies have shown the feasibility of using non-contrast time of flight (TOF) MRA in third trimester fetuses1. However, predominantly due to concerns of motion, it is challenging to consistently obtain diagnostic quality and replicate the same in younger gestation fetuses. On the other hand, it is known that oversampling the central k-space can provide immunity to motion related artifacts. However, radial trajectories are very susceptible to gradient delays causing relative shifts between the sampling window and the read-out gradient (shift in the center of the echo). Manufacturers address this delay by modifying the moment of the dephasing lobe which ensures that the echo-center occurs at the center of the sampling window. This approach is robust for a non-flow compensated gradient structure; addition of a bipolar gradient for flow compensation (FC), as required for MRA (or) SWI, makes it difficult to correct for the gradient delay by moment compensation because both the zeroth and first moment of the readout need to be simultaneously zero at the echo coinciding with the read-out window. In this work, we show that a simple shift of the readout-window to account for the isotropic gradient delays can address this issue. We report the use of a fully FC, readout-shifted 2D radial gradient echo sequence to perform non-contrast MRA of the human fetus in-utero. The added advantage of using radial sampling is the ability to do FC in all dimensions without additional time. With long TRs used in fetal angiography for reduced SAR1, multi echo readouts were also possible, allowing for T2* quantification of fetal blood at the same time.Methods
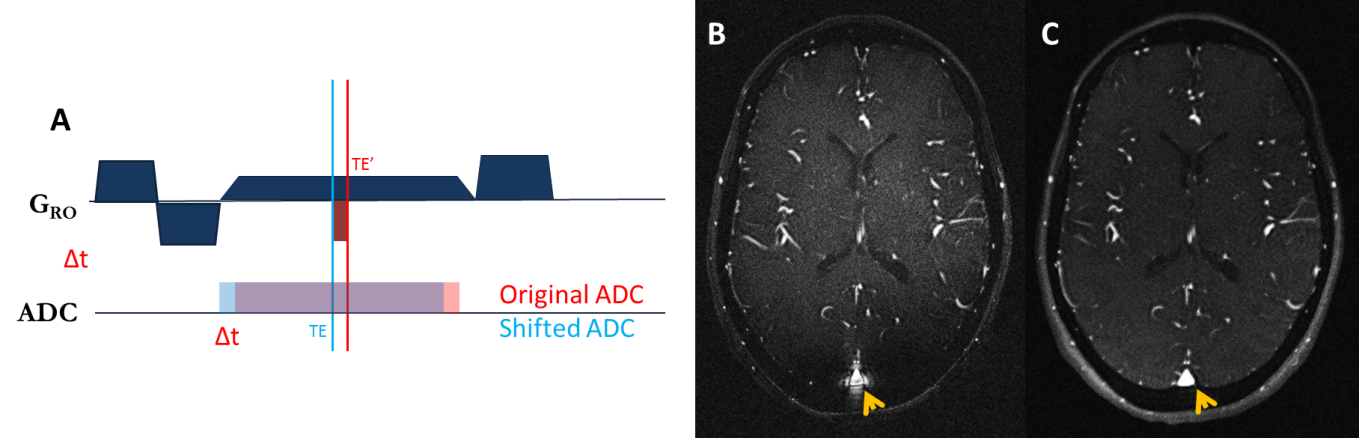
All MRI scans were performed on a Siemens Verio 3.0T. The quality of the gradient shifting concept was tested on adult volunteers. The isotropic gradient delay was calculated as Δt = 0.42*Tos – 3.7μs 2 and the readout was shifted by the same time (fig 1). A 2D TOF MRA1 sequence was first acquired followed by a 2D radial sampling scheme (rMRA), covering almost identical volumes in the fetuses. The same sequence timing parameters and field-of-view as the Cartesian were used for the radial acquisition with number of radial spokes = 361 (over 360o) and 720 points per readout with ~30% asymmetry in the readout for both cases. The in-plane resolution of the radial scans was higher (0.42mm vs. 0.57mm) compared to Cartesian data due to the differences in the number of points per readout (720 vs. 512). 3D rendering and maximum intensity projections (MIP) of the fetal vessels were created for visualization and anatomical landmarks. In a subset of the cases, T2* was estimated by fitting the dual echo data to a mono-exponential function. T2* of the fetal blood was measured by placing the ROI in the descending Aorta.Results
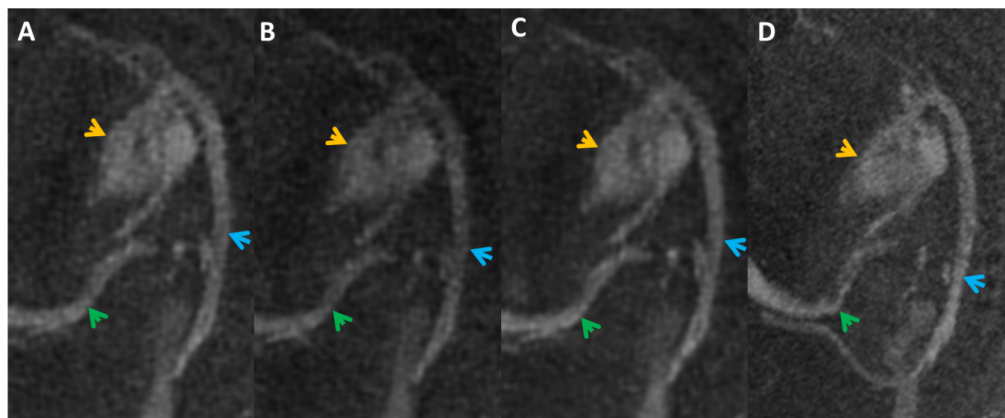
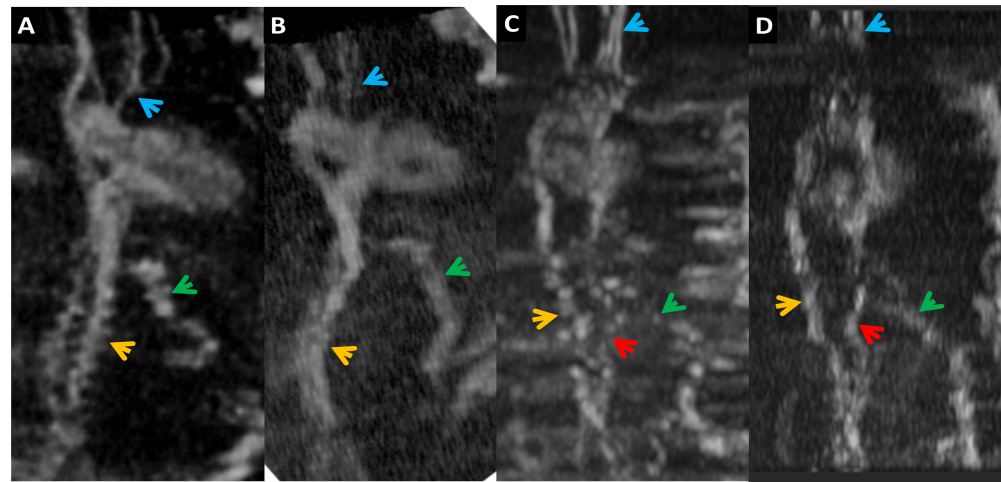
Shifting the sampling window to compensate for the gradient delay improves the image quality as demonstrated in Figure 1a. It is important to note the improvement in the edge definition of the superior saggital sinus (SSS). Fetal MRA data was acquired from 7 subjects (4 third & 3 second trimester) with uncomplicated singleton pregnancies. In cases of no fetal motion, particularly in the third trimester, the rMRAs were as good as those obtained from regular Cartesian MRA (Figure 2), however, in cases of moderate fetal motion, the rMRAs performed much better (figure 3). The T2* of blood measured from the descending aorta in a 27 week fetus was estimated to be 21.24 ± 3.23 ms.Discussion & Conclusion
Radially sampled data provided the touted advantage of motion-insenstivity in fetal angiography. Radial MRA, with 361 spokes however, took 7.9 sec/slice, compared to 4.73 sec/slices for Cartesian. This was because the Cartesian images used both partial Fourier (factor 1.33) and GRAPPA (factor 2). Radial GRAPPA or other non-Cartesian parallel imaging approaches were not taken advantage of for radial sampling in this work. The long TR allowed for fully FC multi-echo readouts that offers: (a) T2* mapping of the fetal vasculaure; b) enhancement of the SNR of the first echo through data averaging (figure 2c); and (c) using the phase from the second echo for MR susceptometry3. Higher order acceleration and turbulence terms might be underestimating the T2* and needs to be further optimized. In conclusion, the radial sampling scheme holds great promise for fetal angiography applications. Future works that can incorporate FC multi-spoke readout within the same TR could further accelerate such acquisitions, bringing the acquisition time under 2 or 3 seconds per slice, with the ability for simultaneous T2* quantification.Acknowledgements
No acknowledgement found.References
[1] Neelavalli, J., Krishnamurthy, U., Jella, P. K., Mody, S. S., Yadav, B. K., Hendershot, K., ... & Hassan, S. S. (2016). Magnetic resonance angiography of fetal vasculature at 3.0 T. European radiology, 1-7.
[2] Speier P, Trautwein F. Robust radial imaging with predetermined isotropic gradient delay correction. In: Proc 14th Annual Meeting ISMRM, Seattle; 2006: 2379.
[3] Neelavalli, J., Jella, P. K., Krishnamurthy, U., Buch, S., Haacke, E. M., Yeo, L., ... & Romero, R. (2014). Measuring venous blood oxygenation in fetal brain using susceptibility-weighted imaging. Journal of Magnetic Resonance Imaging, 39(4), 998-1006.
Figures