0045
Myocardial extracellular volume expansion precedes functional myocardial alterations during the evolution of systemic sclerosis1Institute for Biomedical Engineering, University & ETH Zurich, Zurich, Switzerland, 2Department of Cardiology, University Hospital Zurich, Zurich, Switzerland, 3Faculty Mechanical and Medical Engineering, Furtwangen University, Schwenningen, Germany, 4Department of Rheumatology, University Hospital Zurich, Zurich, Switzerland
Synopsis
Myocardial involvement is common in patients with systemic sclerosis and is known to cause myocardial fibrosis and subtle ventricular dysfunction. Both can be characterized by novel CMR methods like native T1-mapping, ECV quantification or LV deformation imaging. However, the temporal onset of myocardial fibrosis and functional impairment during the progression of the disease is still unknown. Therefore, we investigated the presence of subclinical functional and fibrotic myocardial involvement in patients with very early diagnosis of systemic sclerosis and found that the expansion of ECV can be detected before LV functional impairment, assessed by CMR feature tracking, can be observed.
Introduction
Myocardial involvement is common in patients with systemic sclerosis (SSc) and often characterized by Cardiovascular Magnetic Resonance (CMR) as focal fibrosis on late gadolinium enhancement (LGE) images [1]. Novel methods such as T1 mapping or the quantification of extracellular volume (ECV) have shown to identify subclinical myocardial fibrosis [2]. In addition, impaired ventricular function, as defined by reduced strain, has been found in patients with SSc [2,3]. However, the temporal onset of myocardial fibrosis and functional impairment during the progression of the disease is still unknown. Therefore we investigated the presence of subclinical functional and fibrotic myocardial involvement in patients with very early diagnosis of systemic sclerosis (VEDOSS) and compared the findings with healthy controls and patients with established SSc, fulfilling the criteria of the American College of Rheumatology (ACR).Methods
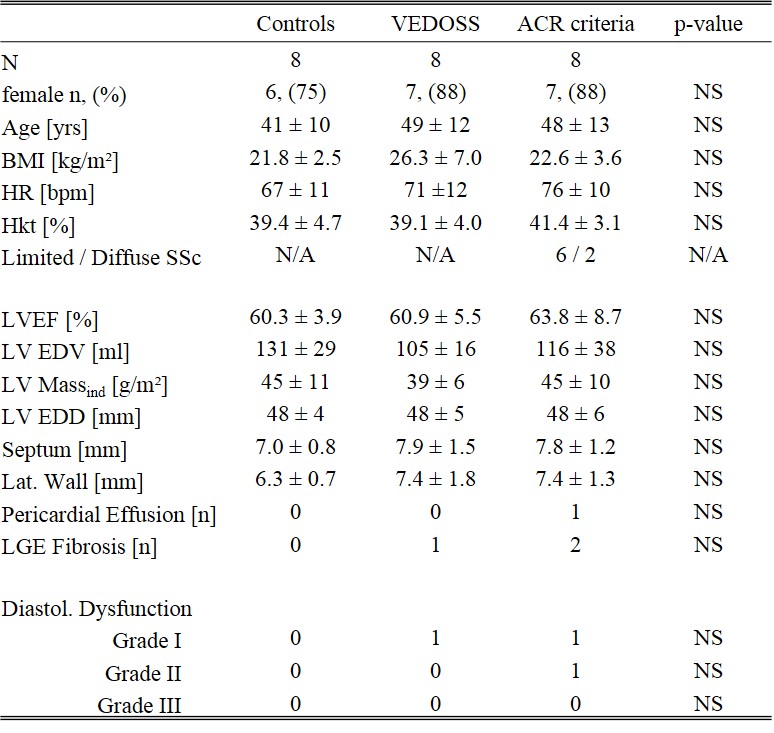
For this cross-sectional study, 8 VEDOSS patients (7 female, mean age 49 ± 12 years), 8 patients with established SSc according to the ACR criteria (7 female, mean age 48 ± 13 years) and 8 sex- and age-matched controls (6 female, mean age 41 ± 10 years) without known cardiovascular disease were prospectively recruited. All study subjects underwent CMR on a clinical 1.5T system (Philips Healthcare, Best, The Netherlands).
Myocardial fibrosis was assessed on three short axis slices. Pre- and post-contrast T1 mapping was performed using a MOLLI (Modified Look-Locker Inversion Recovery) sequence [4]. The registration of individual MOLLI images for motion compensation and calculation of T1 maps was performed in Matlab using a groupwise image registration method based on [5]. The evaluation of the T1 maps was performed with GTVolume (GyroTools LLC, Zurich, CH). For ECV measurements, a single bolus protocol with image acquisition 20 min. post-contrast injection was used.
For the assement of subtle impairment of ventricular function, myocardial deformation derived from a CMR feature tracking (FT) algorithm (TomTec, Unterschleissheim, Germany) was analysed. On standard SSFP cine images, FT was applied to three short axis views for the measurement of global circumferential strain (GCS) and to 2-, 3- and 4-chamber views for measuring global longitudinal strain (GLS).
All data are expressed as mean ± SD. Differences between the groups were analyzed using a one-way ANOVA with Tukey's HSD post-hoc comparison. A P value of <0.05 was considered statistically significant.
Results
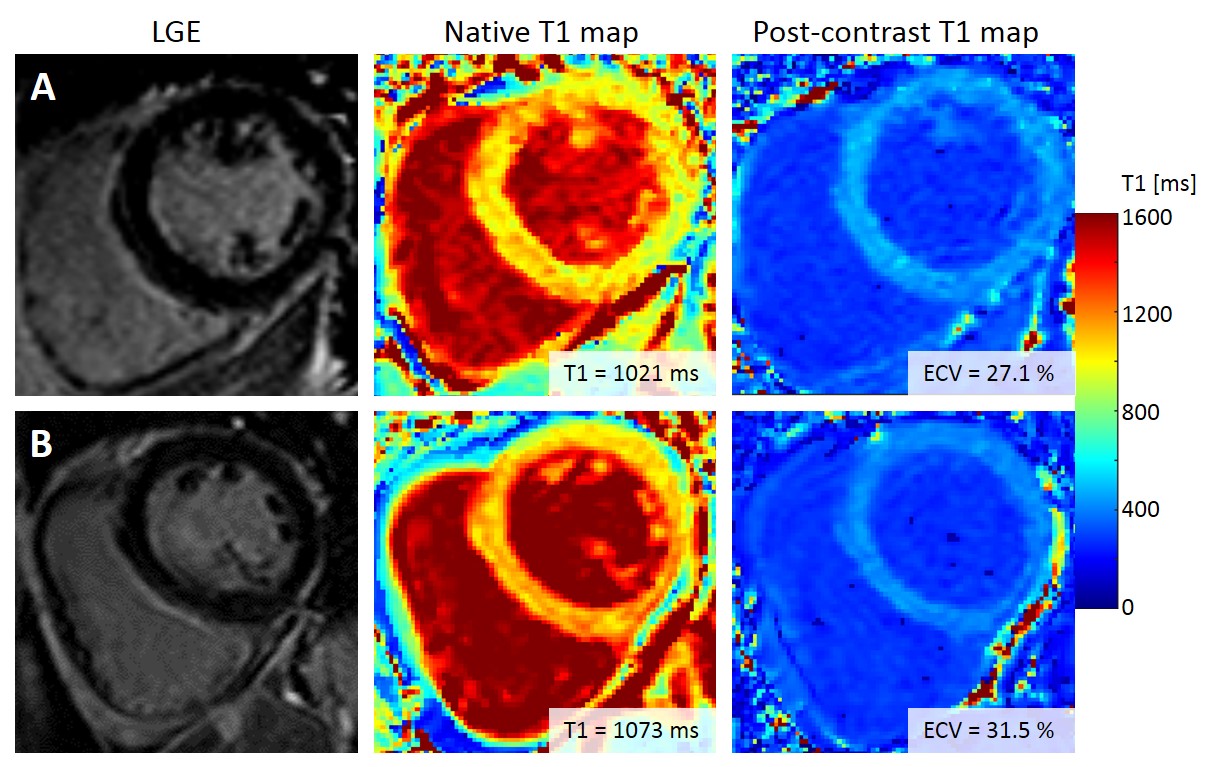
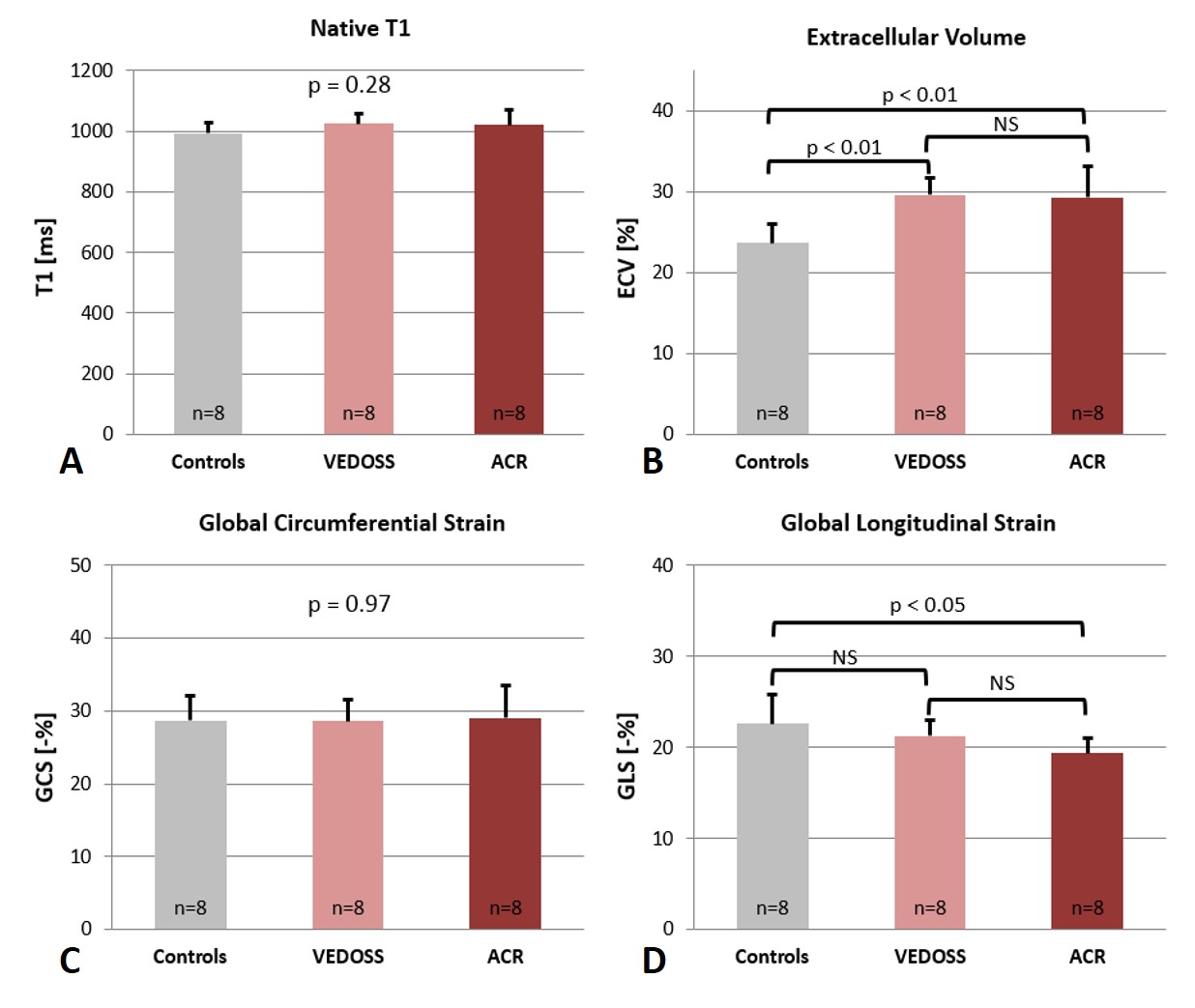
Except for a non-significant trend to larger LV EDV in healthy controls, the baseline characteristics showed no relevant differences between the groups (see Table 1). Native T1 values exhibited a trend to higher values in VEDOSS and ACR-SSc patients (Controls 993 ± 33 ms, VEDOSS 1024 ± 34 ms, ACR-SSc 1019 ± 51 ms; p = 0.28). In contrast, both VEDOSS and ACR-SSc patients showed a significant expansion of ECV compared to healthy controls (Controls 23.7 ± 2.3 %, VEDOSS 29.5 ± 2.1 %, ACR-SSc 29.4 ± 3.8 %; p < 0.01). Figure 1 displays exemplary LGE as well as native and post-contrast T1 images of a VEDOSS and a SSc patient.
In the LV deformation analysis, GLS was significantly elevated only for patients with established SSc compared to healthy controls (Controls -22.6 ± 3.2 %, VEDOSS -21.3 ± 1.8 %, ACR-SSc -19.4 ± 1.7 %; p = 0.039). GCS was similar across all groups (Controls -28.7 ± 3.5 %, VEDOSS -28.6 ± 2.9 %, ACR-SSc -29.0 ± 4.4 %; p = 0.98). All results are displayed in Figure 2.
Discussion
Our data demonstrates that subclinical myocardial changes first manifest as expansion of ECV and precedes subtle functional myocardial impairment in patients with very early stages of systemic sclerosis (VEDOSS). Regarding native T1 values, the literature reports conflicting data [2,6]. In our study population, native T1 was not significantly elevated in VEDOSS patients and patients with established SSc, which may partly be caused by the small sample size. In addition, patients with established SSc showed the largest variability of native T1 data.
LV deformation analysis identified impaired strain parameters only for GLS in patients with established SSc. Thereby, ECV as a biomarker of diffuse fibrosis seems to have the highest sensitivity for the detection of early myocardial remodeling, in very early SSc. Longitudinal studies are required to investigate the predictive value of ECV-mapping as an early marker for the progression of systemic sclerosis and internal organ involvement.
Acknowledgements
No acknowledgement found.References
1. Mavrogeni et al. Cardiovascular magnetic resonance in rheumatology: Current status and recommendations for use. Int J Cardiol. 2016;217:135-48.
2. Ntusi et al. Subclinical myocardial inflammation and diffuse fibrosis are common in systemic sclerosis--a clinical study using myocardial T1-mapping and extracellular volume quantification. J Cardiovasc Magn Reson. 2014;16:21.
3. Kobayashi et al. Detection of Left Ventricular Regional Dysfunction and Myocardial Abnormalities Using Complementary Cardiac Magnetic Resonance Imaging in Patients with Systemic Sclerosis without Cardiac Symptoms: A Pilot Study. Internal medicine. 2016;55:237-43.
4. Messroghli et al. Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magn Reson Med. 2004;52:141-6.
5. Vishnevskiy et al. Isotropic Total Variation Regularization of Displacements in Parametric Image Registration. IEEE transactions on medical imaging. 2016.
6. Barison et al. Early myocardial and skeletal muscle interstitial remodelling in systemic sclerosis: insights from extracellular volume quantification using cardiovascular magnetic resonance. Eur Heart J Cardiovasc Imaging. 2015;16:74-80.
Figures