0025
7T TOF-MRA Shows Different Patterns of Perforating Artery in Patients with Intracranial Atherosclerosis Disease (ICAD) and Cerebral Autosomal-Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL)1State Key Laboratory of Brain and Cognitive Science, Beijing MR Center for Brain Research, Institute of Biophysics, Chinese Academy of Sciences, Beijing, People's Republic of China, 2University of Chinese Academy of Sciences, Beijing, People's Republic of China, 3Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 4Xuanwu Hospital, Beijing, People's Republic of China, 5Department of Neurology, Peking University First Hospital, Beijing, People's Republic of China, 6Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, People's Republic of China
Synopsis
7T high-resolution TOF-MRA has the ability to image perforating arteries of middle cerebral artery (MCA). The distribution patterns of orifices in CADASIL (cerebral autosomal-dominant arteriopathy with subcortical infarcts and leukoencephalopathy) and ICAD (intracranial atherosclerosis disease) patients are still unclear. In this study, for the first time, we investigated the orientation distribution of perforating artery orifices on MCA trunks using 7T TOF-MRA. Specific features are found in the distribution patterns of orifices in patients with CADASIL, ICAD and healthy volunteers. This technique is promising in the pathological studies of intracranial vascular diseases.
Introduction
The orifices of perforating arteries may be affected by different intracranial vasculopathy1. This study aimed to investigate the pattern of the orifices of perforating arteries using high-resolution TOF-MRA at 7T in ICAD (intracranial atherosclerosis disease) patients, CADASIL (cerebral autosomal-dominant arteriopathy with subcortical infarcts and leukoencephalopathy) patients and healthy volunteers.Methods
Seventeen healthy controls (aged 33-63 years, 8 males) as well as thirteen ICAD patients (aged 15-72 years, 9 males) and twenty-four CADASIL patients (aged 29-64 years, 17 males) with confirmed clinical diagnosis were prospectively collected. Informed consent was obtained from all participants. All the images were acquired on a 7T research system (Siemens, Erlangen, Germany) equipped with a Nova 32-channel head coil. All subjects underwent 3D TOF-MRA and 3D T1-weighted (T1w) MPRAGE scans. The study was approved by the local IRB and written informed consent was obtained from all participants.
For 3D T1w-MPRAGE, the parameters were: FA (flip angle) = 7°, TR = 2200ms, TE = 3.29ms, voxel = 0.70x0.70x0.70mm3, FOV = 224x203x180mm3, GRAPPA = 2, TA (Time of Acquisition) = 5:06min. Before imaging the target vessels (i.e., perforating arteries) at high resolution, a low-resolution TOF-MRA with voxel=isotropic 0.80mm and TA = 1:08 was acquired. For high-resolution TOF-MRA, the following parameters were used: FA = 20°, TR = 15ms, TE = 4.30ms, voxel = 0.23x0.23x0.36mm3, FOV = 180x135x47mm3, GRAPPA = 2, TA = 7:34min.
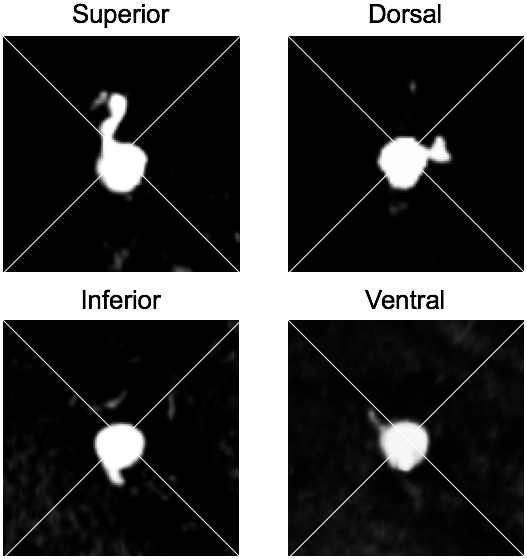
In pre-processing, the TOF-MRA images were reoriented to have an AC-PC alignment. Based on the maximum intensity projection (MIP) of the TOF. Section views of MCA were extracted where a perforating artery originated from an M1 segment. All cross-sections were classified based on the orientation of orifices. Mann-Whitney U test was used to compare the number of orifices in every quadrant between patients and volunteers. For patients with ICAD, the orifices of perforating arteries were separately analyzed on the ipsilateral side and the contralateral side.
Results
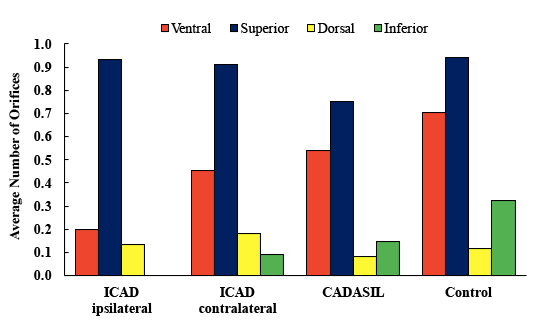
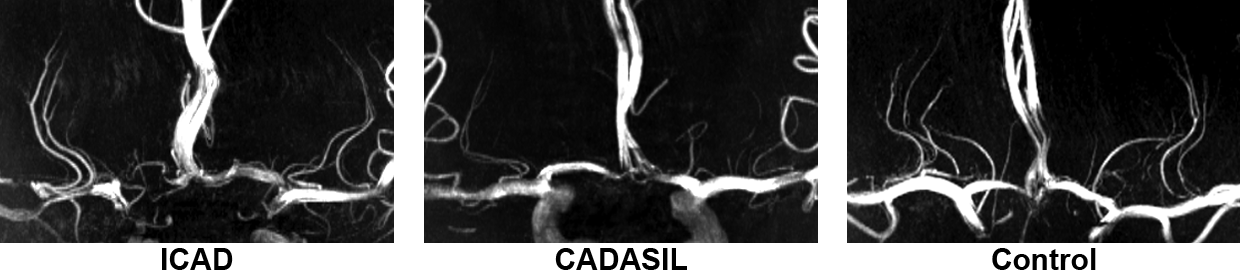
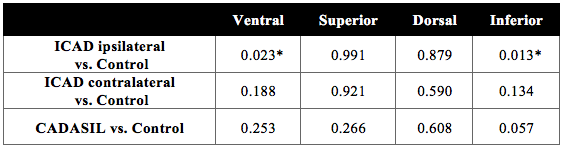
The criteria of orifices classification were demonstrated in Fig. 1. The distributions of perforating artery orifices in the 4 quadrants in hemispheres of patients and volunteers were shown in Fig. 2. Most orifices were located on the superior and ventral sides both in patients and in volunteers. The p values of Mann-Whitney U test on the numbers of orifices were listed in Table 1. In ICAD patients, the numbers of ventral and inferior orifices on the ipsilateral side were significantly lower than healthy controls, while the numbers on the contralateral side had no significant differences than the control group. The distribution pattern of CADASIL patients was consistent with the control group. The representative MIP images of 7T TOF-MRA were shown in Fig. 3.Discussion
For ICAD patients, the distribution and quantity of orifices were affected mainly on the ipsilateral side, especially on ventral and inferior part of MCA comparing with the contralateral side. Due to this different pattern, the blood flow of perforating arteries in ICAD patients is mostly supplied by the superior branches. This change may be related to the compensatory mechanism caused by the stenosis of MCAs.
In our study, we found that perforating arteries of CADASIL patients are rarely affected and the distribution of orifices is the same as the control group. However, the number of trunks decreased compared with healthy volunteers, although significant difference level (p=0.05) is not reached.
Conclusion
We demonstrated for the first time that the orientation distribution of perforating arteries orifices on MCA trunks can be visualized and analyzed on high-resolution TOF-MRA at 7T in different intracranial vasculopathy. High-resolution TOF-MRA at 7T may allow a better understanding of the pathology of large and small vessel diseases.Acknowledgements
This work was supported in part by Chinese MOST grants (2015CB351701, 2012CB825500), NSFC grant (91132302), and CAS grants (XDB02010001, XDB02050001).References
1. WH Xu, ML Li, S Gao, et al. Plaque distribution of stenotic middle cerebral artery and its clinical relevance. Stroke, 42 (2011), pp. 2957–2959.Figures