0006
Evaluation of cardiac magnetic resonance thermometry in patients1Electrophysiology and Heart Modeling Institute, Bordeaux, France, 2Siemens Healthcare, Paris, France, 3Mathematical Institute of Bordeaux, Bordeaux, France, 4Department of Cardiac Electrophysiology, Hôpital Cardiologique de Haut-Lévêque, Bordeaux, France
Synopsis
Recent studies have proposed to monitor radiofrequency ablation on the heart using real-time MR-thermometry. Methods rely on ECG triggering which can fail in presence of arrhythmia. This study evaluates the precision of MR-thermometry on patients (N=15) even in presence of cardiac arrhythmia. Phase images were acquired using a single-shot multi-slice echo planar imaging and temperature maps were calculated and displayed on the fly. ECG was recorded simultaneously for further analysis of cardiac rhythm and post-processing of temperature images. Stability of temperature mapping without RF-heating was evaluated in each pixel and correlated to the prevalence of arrhythmia.
INTRODUCTION
Catheter-based radiofrequency ablation (RFA) is a widely accepted method for clinical treatment of cardiac arrhythmia, with 200 000 procedures performed in Europe in 2014 [1]. However, both safety and efficacy could be improved by monitoring lesion formation in real time, thereby reducing recurrences which often require redo procedures [2]. MR-thermometry has the potential to visualize lesion formation in real-time during RFA [3]. Recent studies reported reliable cardiac thermometry [4, 5] during RFA by combining ECG-triggered imaging and online correction of respiratory motion and associated susceptibility artifacts. However, variations in cardiac cycle duration may lead to erroneous temperature estimate. The purpose of the present study is to evaluate the precision of MR-thermometry without RF-heating, including in patients with cardiac arrhythmia and to demonstrate feasibility of the method in clinical environment.METHODS
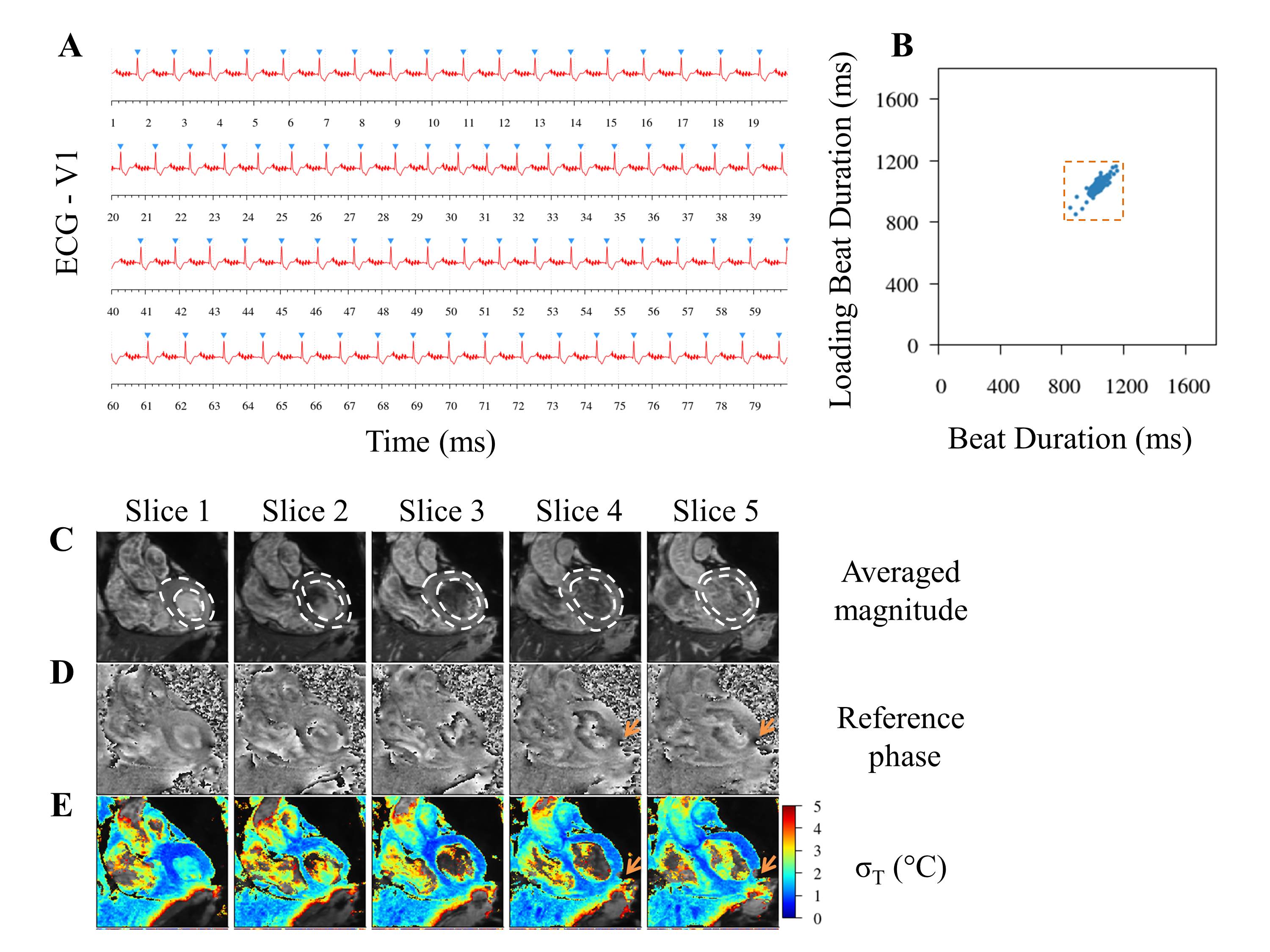
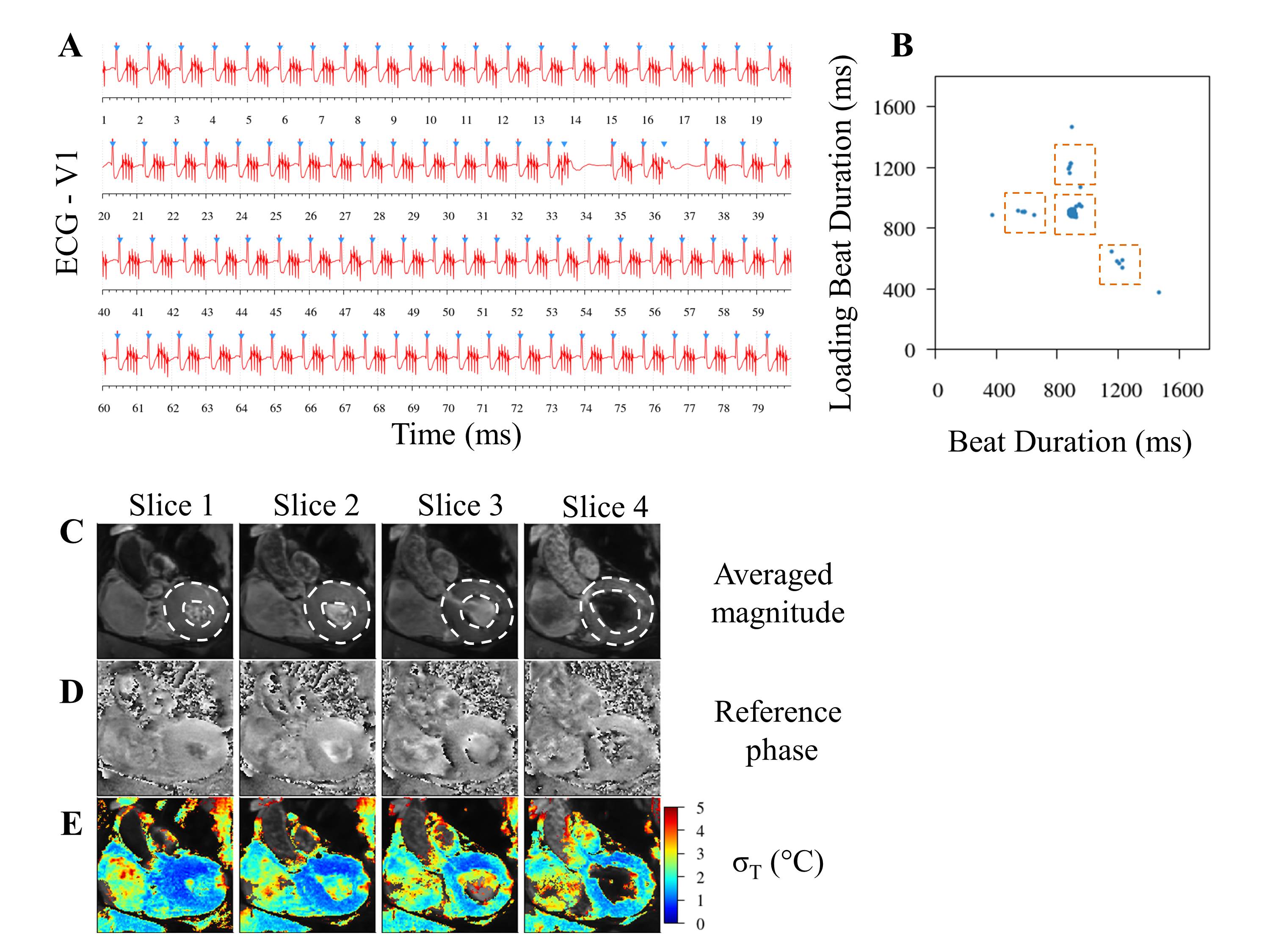
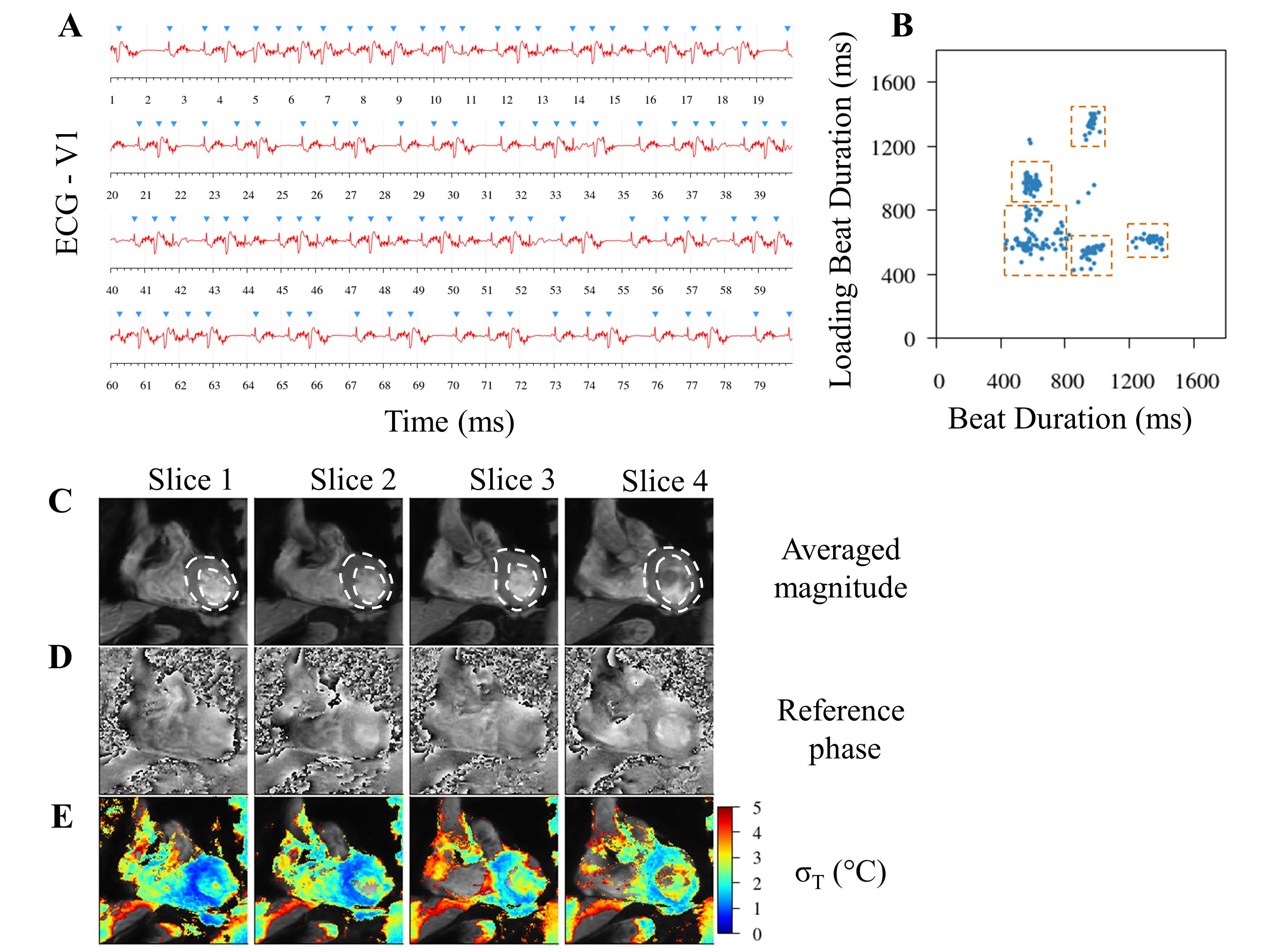
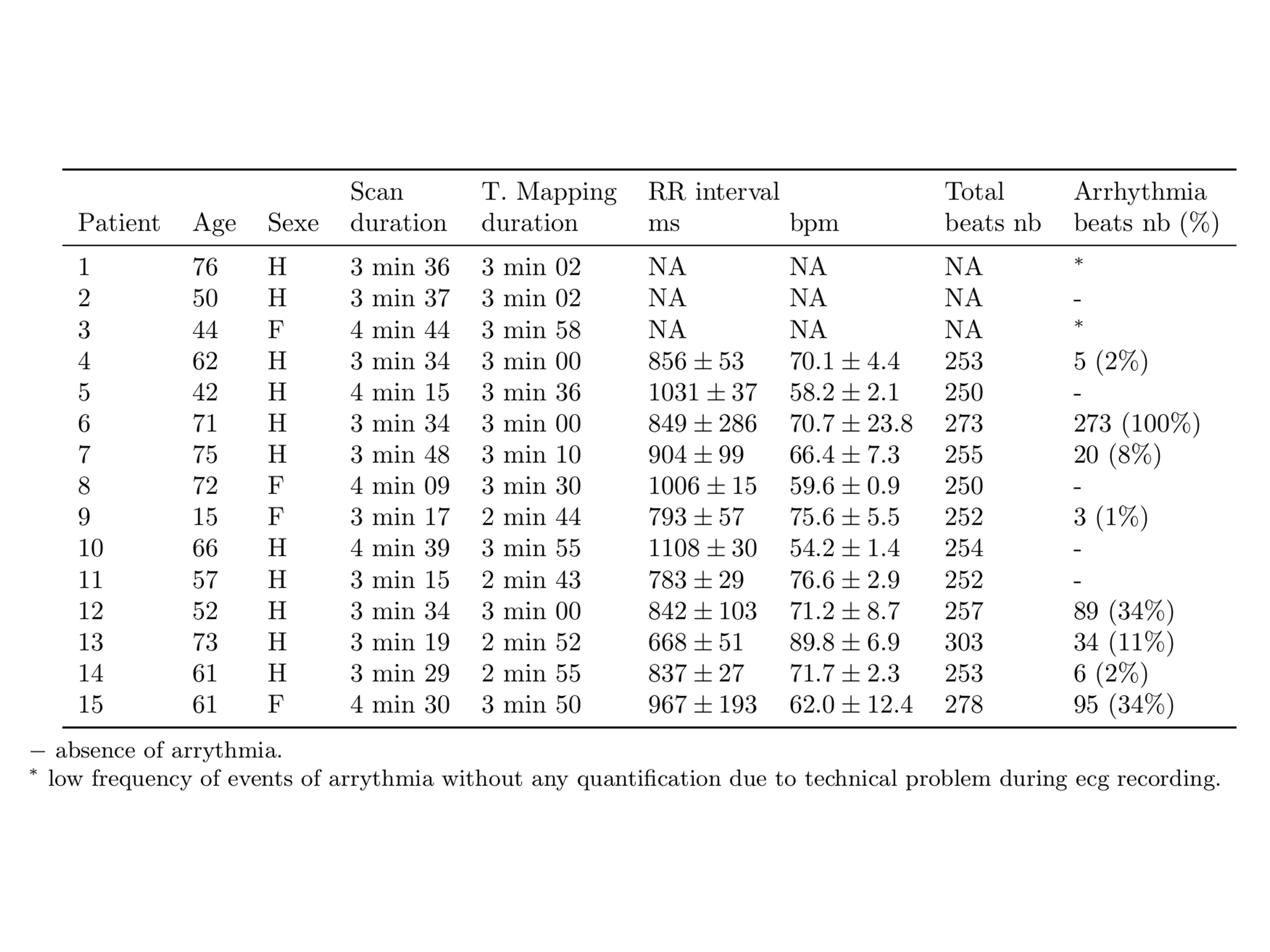
Patients: the study was approved by the Institutional Review Board and all subjects (N=15, 58.5 ± 16.2 years old and eleven male) gave informed consent to be included in the study. Five patients were in sinus rhythm and did not show substantial variations of the RR duration during scanning, whereas ten patients displayed irregular rhythm. MR Imaging: 4 to 5 temperature slices in coronal orientation were acquired sequentially under free breathing at each heartbeat during approximately 3’30 minutes on a 1.5 T MRI (Avanto, Siemens Healthcare). The sequence was a single shot gradient EPI (TE=20ms, TR=85ms, Grappa=2) with 110x110 voxels corresponding to a 1.6x1.6x3mm3 voxel size (zero filled to 0.8x0.8x3mm3). Image reconstruction, correction of residual in-plane respiratory motion and associated susceptibility variations, compensation of spatial-temporal phase drift and low pass temporal filtering were implemented in the Gadgetron framework [6], ensuring online visualization of temperature images [5]. To assess the precision of cardiac MR-thermometry, the temporal standard deviation of temperature (σT) over time was computed in each voxel from all slices during the procedure. The distribution of σT values was analyzed on a manually drawn ROI surrounding the left ventricle. Voxels where σT was higher than 5°C were removed from the statistical analysis. Categorization of Beats: ECG was recorded using standard 3-lead (ECG) acquisition. An algorithm was designed to identify, synchronize and categorize beats based on two successive RR durations, as proposed by Contijoch et al [7].RESULTS
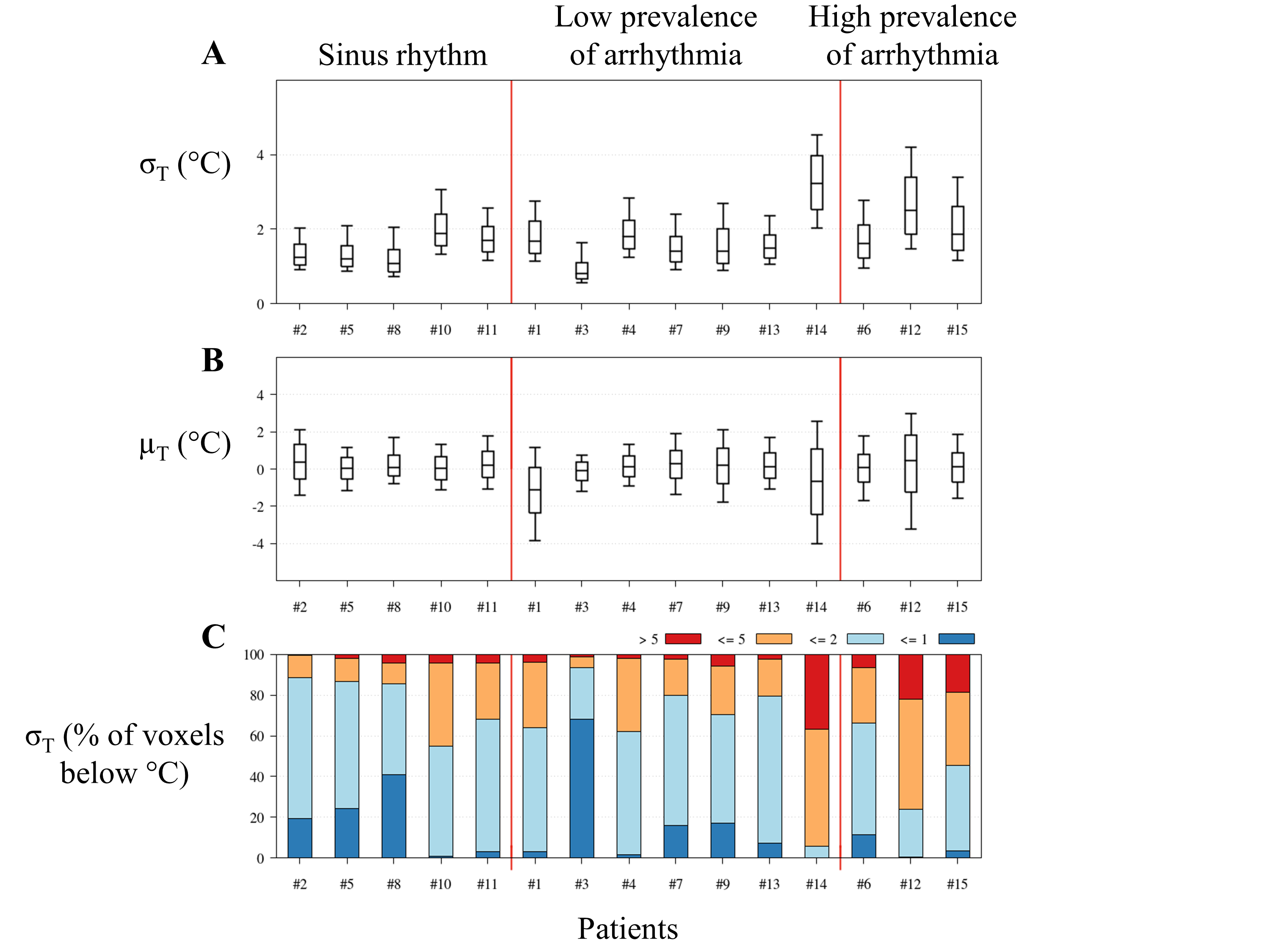
The mean ± SD heart rate across all patients was 69 ± 10 bpm, ranging from 54 to 90 bpm (Table 1). Data were first sorted in three groups: 1) patients in sinus rhythm, 2) patients with low frequency of event of arrhythmia (less than 15% prevalence) and 3) patients with high frequency of event of arrhythmia (more than 15% prevalence). In each group, a representative case study is detailed in Figures 1, 2 and 3, respectively. The statistical analysis of temperature distribution over the patients is presented in Figure 4 using a box and whisker plot. Over the patients in group 1, σT was 1.57 ± 0.34 °C with a total of 4343 ± 1817 voxels per slice. Only 3 % of the voxels in the ROI were excluded due to residual phase unwraps or σT higher than 5°C. In group 2, σT was 1.83 ± 0.70 °C (7 % of voxels excluded) and 2.17 ± 0.46 °C in group 3 (19 % of voxels excluded).DISCUSSION
Temperature uncertainty remains below 2°C in more than 60% of the voxels of the left ventricle in 12/15 patients (Fig 4C). In patient with sinus rhythm, temperature uncertainty was consistent across subjects, with variation below 0.5°C. Although significant cardiac motion inconsistency during arrhythmia can lead to image artifacts, in most cases phase images showed good quality, as illustrated in Figures 2D, 3D, 4D, resulting in stable temperature all over the left myocardium with the exception of small area. Nevertheless, both temperature uncertainty and number of voxel with imprecise temperature increased with prevalence of arrhythmia. Additional method to automatically identify and discard artifacted images in the time series might help to improve cardiac thermometry in presence of arrhythmia.CONCLUSION
This study presents the first evaluation of cardiac MR-thermometry on patients during free-breathing. The precision of temperature estimate was found of sufficient quality to monitor catheter-based RF ablation procedures in most cases.Acknowledgements
This work received the financial support from the French National Founding Agency (ANR) within the context of the Investments for the Future Program: referenced ANR-10-LABX-57 and named TRAIL and referenced ANR-10-IAHU-04 and named IHU LIRYC. This study was also supported by public grants from the French ANR: program TACIT ANR-11-TecSan-003-01; Equipex MUSIC ANR-11-EQPX-0030; and program MIGAT ANR-13-PRTS-0014-01References
1. Raatikainen MJ, Arnar DO, Zeppenfeld K, Merino JL, Levya F, Hindriks G, et al. Statistics on the use of cardiac electronic devices and electrophysiological procedures in the European Society of Cardiology countries: 2014 report from the European Heart Rhythm Association. Europace. 2015;17 Suppl 1:i1-75.
2. Tanner H, Hindricks G, Volkmer M, Furniss S, Kuhlkamp V, Lacroix D, et al. Catheter ablation of recurrent scar-related ventricular tachycardia using electroanatomical mapping and irrigated ablation technology: results of the prospective multicenter Euro-VT-study. J Cardiovasc Electrophysiol. 2010;21(1):47-53.
3. Kolandaivelu A, Zviman MM, Castro V, Lardo AC, Berger RD, Halperin HR. Noninvasive assessment of tissue heating during cardiac radiofrequency ablation using MRI thermography. Circ Arrhythm Electrophysiol. 2010;3(5):521-9.
4. de Senneville BD, Roujol S, Jaïs P, Moonen CTW, Herigault G, Quesson B. Feasibility of fast MR-thermometry during cardiac radiofrequency ablation. NMR in Biomedicine. 2012;25(4):556-62.
5. Ozenne V, Toupin S, Bour P, de Senneville BD, Lepetit-Coiffe M, Boissenin M, et al. Improved cardiac magnetic resonance thermometry and dosimetry for monitoring lesion formation during catheter ablation. Magn Reson Med. 2016.
6. Hansen MS, Sorensen TS. Gadgetron: an open source framework for medical image reconstruction. Magn Reson Med. 2013;69(6):1768-76.
7. Contijoch F, Rogers K, Rears H, Shahid M, Kellman P, Gorman J, 3rd, et al. Quantification of Left Ventricular Function With Premature Ventricular Complexes Reveals Variable Hemodynamics. Circ Arrhythm Electrophysiol. 2016;9(4).
Figures