5043
Transient respiratory motion artifacts in multiple arterial phases of contrast-enhanced dynamic MR imaging of the abdomen: a comparison using gadoxetate disodium and gadobutrol.1Radiology, Yamaguchi University Graduate School of Medicine, Ube, Yamaguchi, Japan
Synopsis
This
study compared the occurrence of transient respiratory motion artifacts (TRMA)
in multiple arterial phases of contrast-enhanced MR imaging using a rapid
acquisition technique with high temporal and spatial resolution between
gadoxetate disodium and gadobutrol. This study showed that the frequency of TRMA
after third arterial phase was significantly higher in patients using
gadoxetate disodium than in patients using gadobutrol. In multiple arterial
phase dynamic MR imaging, the frequency of TRMA in gadoxetate disodium increased,
compared with gadobutrol, caused by the intolerable respiratory suspension
after third arterial phase, possibly due to contrast agent-related effect.
INTRODUCTION:
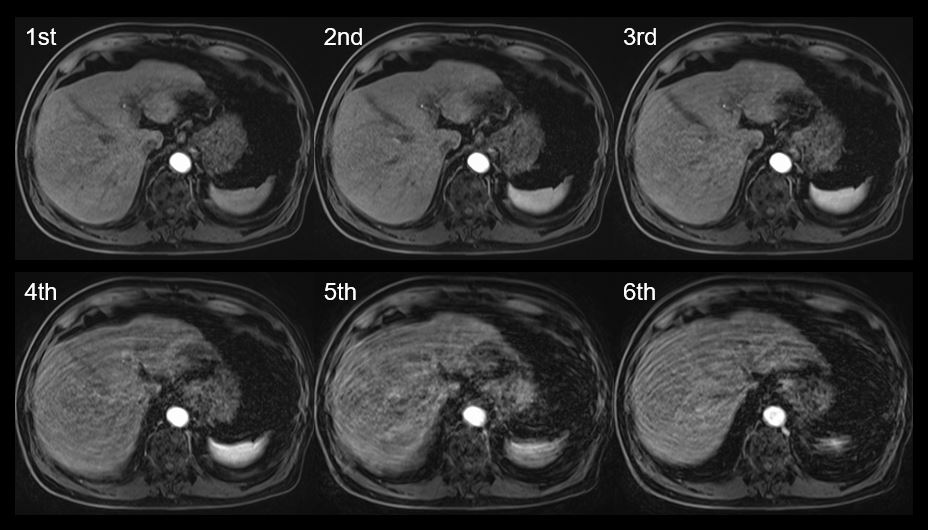
In gadoxetate disodium enhanced dynamic MR imaging of the abdomen, there have been several reports of increased transient respiratory motion artifacts (TRMA) on arterial phase imaging compared with other gadolinium-based contrast agents although the exact causes and mechanism of TRMA are still unclear 1-3. However, there has been no report comparing the frequency of TRMA between gadoxetate disodium and gadobutrol (both of them have same standard injection dose of 0.1ml/kg) using multiple arterial phases (6 arterial phases) imaging. The purpose of this study was to compare the occurrence of TRMA in multiple arterial phases (6 phases) of contrast-enhanced MR imaging using a rapid acquisition technique with high temporal and spatial resolution between gadoxetate disodium and gadobutrol.METHODS:
Two hundred fourteen abdominal MR examinations (101 with gadoxetate disodium [63 men; mean age, 67.4 years; range, 34 - 89 years], 113 with gadobutrol [61 men; mean age, 65.5 years; range, 26 - 86 years]) obtained using 3.0T MRI scanner (Magnetom Prisma, Siemens Healthcare) with 18-channel body coil were evaluated. Dynamic 3D contrast-enhanced T1-weighted MR imaging (CAIPIRINHA-Dixon-TWIST-VIBE) was performed, including single-breath-hold six arterial phase acquisitions. Imaging parameters for multiple arterial phases were as follows: TR 3.78 ms; TE 1.23-2.46 ms; FA 10°; bandwidth 1090 Hz; parallel imaging factor 4; FOV 36×27 cm2; matrix 288×151; slice thickness 2.5 mm; acquisition time 22 sec. Same injection protocol was used for both gadoxetate disodium and gadobutrol: injection dose of 0.1ml/kg, injection rate of 2 ml/s, followed by a 20 mL saline flush (2 ml/s). TRMA on dynamic 3D T1-weighted MR images (6 arterial phases) were assessed using 5-point rating scale (1 = no TRMA, 2 = minimal TRMA with no effect on diagnostic quality, 3 = moderate TRMA with some, but no severe effect on diagnostic quality, 4 = severe TRMA but images still interpretable, 5 = extensive TRMA and non-diagnostic images) 4. Mean TRMA scores were compared with the Mann-Whitney U test. The number of patients with TRMA was compared with the chi-squared test or Fisher exact test.RESULTS:
The frequency of TRMA in patients using gadoxetate disodium (39/101, 39%) was significantly higher than those in patients using gadobutrol (19/113, 17%) (P < .001). Mean TRMA scores in all arterial phases using gadoxetate disodium were significantly worse than those using gadobutrol (1.49 ± 0.78 vs. 1.182 ± 0.53, P < .001). Severe TRMA (score ≥ 4) occurred at a higher rate with gadoxetate disodium than with gadobutrol (16/101 [16%] vs. 5/113 [4%], P < .01). Regarding the timing of the occurrence of TRMA, they were seen in the first arterial phase in 13 (33%) of 39 patients using gadoxetate disodium while they were observed in the first arterial phase in 10 (53%) of 19 patients using gadobutrol, and this difference between the two was not significant (P = .25) (Table 1, Fig 1). The frequency of TRMA after third arterial phase in patients using gadoxetate disodium was significantly higher than that in patients using gadobutrol (25/39 [64%] vs. 6/19 [32%], P = .0189) although there was no significant difference in the mean age of patients between the two groups (68.6 vs. 68.8 years, P = .946).DISCUSSION:
This study showed that the frequency of TRMA after third arterial phase was significantly higher in patients using gadoxetate disodium than in patients using gadobutrol. This fact suggested that patients using gadoxetate disodium may not be able to hold their breath for longer time, possibly due to contrast agent-related effect (e.g., unknown chemical effect). Therefore, it will be important to shorten the acquisition time less than 10 seconds for the arterial phase imaging in order to reduce the risk of respiratory motion artifacts in gadoxetate disodium enhanced dynamic MR imaging. Conversely, there was no significant difference in the frequency of TRMA at the first arterial phase between gadoxetate disodium and gadobutrol. Therefore, we should also note that TRMA can occur in both gadoxetate disodium and gadobutrol at a fixed frequency regardless of length of breath-hold duration.CONCLUSION:
In multiple arterial phase dynamic MR imaging, the frequency of TRMA in gadoxetate disodium increased, compared with gadobutrol, caused by the intolerable respiratory suspension after third arterial phase, possibly due to contrast agent-related effect.Acknowledgements
No acknowledgement found.References
1. Shah MR, Flusberg M, Paroder V, Rozenblit AM, Chernyak V. Transient arterial phase respiratory motion-related artifact in MR imaging of the liver: an analysis of four different gadolinium-based contrast agents. Clin Imaging. 2017;41:23-7.
2. Luetkens JA, Kupczyk PA, Doerner J, Fimmers R, Willinek WA, Schild HH, et al. Respiratory motion artefacts in dynamic liver MRI: a comparison using gadoxetate disodium and gadobutrol. Eur Radiol. 2015;25(11):3207-13.
3. Davenport MS, Viglianti BL, Al-Hawary MM, Caoili EM, Kaza RK, Liu PS, et al. Comparison of acute transient dyspnea after intravenous administration of gadoxetate disodium and gadobenate dimeglumine: effect on arterial phase image quality. Radiology. 2013;266(2):452-61.
4. Kanki A, Tamada T, Abe T, Ikenaga H, Yoshida K, Ito K.
Relationship between transient severe motion of the liver in gadoxetic acid or
iodinated contrast agent-enhanced imaging and arterial oxygen saturation and
heart rate changes. Magn Reson Imaging. 2018;53:77-81.
Figures
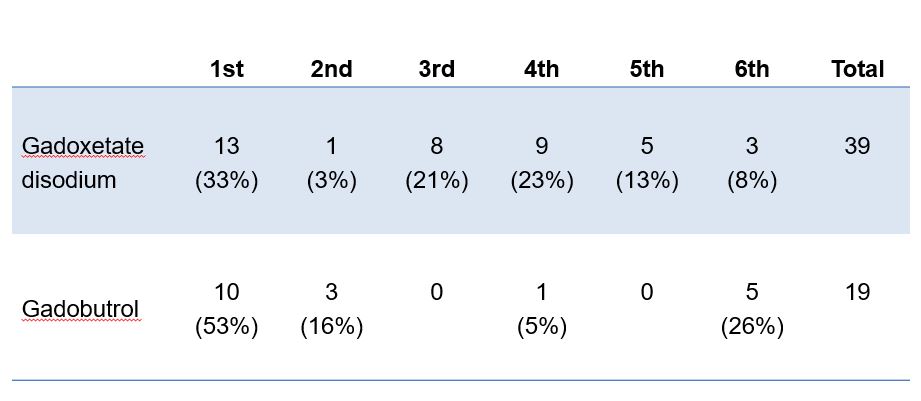
Table 1. The timing of the occurrence of TRMA
Data are given as number with percentage in parenthesis. TSMA = transient sever motion artifact in arterial phase.