5031
An Algorithm for the Automated Quality Assessment and Perfusion Biomarker Determination of Multicentre Dynamic Susceptibility Contrast (DSC-) MRI1Physical Sciences for Health CDT, University of Birmingham, Birmingham, United Kingdom, 2Institute of Cancer and Genomic Sciences, University of Birmingham, Birmingham, United Kingdom, 3Department of Oncology, Birmingham Children's Hospital, Birmingham, United Kingdom, 4RRPPS, University Hospitals Birmingham NHS Foundation Trust, Birmingham, United Kingdom, 5School of Biological Sciences and Medical Engineering, Southeast University, Nanjing, China, 6Radiology, Birmingham Children's Hospital, Birmingham, United Kingdom, 7Radiology, Alder Hey Children's NHS Foundation Trust, Liverpool, United Kingdom, 8Oncology, Alder Hey Children's NHS Foundation Trust, Li, United Kingdom, 9The Children's Brain Tumour Research Centre, University Of Nottingham, Nottingham, United Kingdom, 10Sir James Spence Institute of Child Health, Royal Victoria Infirmary, Newcastle, United Kingdom, 11Neuroradiology, The Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle, United Kingdom, 12Sir Peter Mansfield Imaging Centre, University Of Nottingham, Nottingham, United Kingdom, 13Institute of Digital Healthcare, University of Warwick, Coventry, United Kingdom
Synopsis
Dynamic Susceptibility Contrast (DSC-) MRI estimates biomarkers, such as cerebral blood volume (CBV). However, data quality varies between centres and quality control (QC) is carried out by qualitative review, which is time-consuming and subjective. An automated QC pipeline was developed and tested on 34 patient data sets. The pipeline analysed four slices from each patient, producing SNR, RMSE, relative CBV (rCBV), and quality maps for each slice, which were used to quantify QC. Average values for each parameter were produced for each centre, protocol and field strength, showing variability in data quality and providing a basis for multi-centre protocol optimisation.
Introduction
Dynamic Susceptibility Contrast (DSC-) MRI uses a contrast agent to estimate perfusion biomarkers, such as cerebral blood volume (CBV). The contrast agent causes a decrease in signal intensity as it passes through the brain. Each pixel has a time course, which shows changes in signal intensity1. The time course is susceptible to changes in protocol, field strength and artefacts such as motion and susceptibility; affecting biomarker accuracy. Different centres use different scanners and protocols, causing variability in data quality; making it difficult to obtain robust biomarker estimates. Some centres use a pre-bolus, which is important in low grade tumours, as leakage correction can result in T1 effects2. The current quality control (QC) method is based on expert qualitative review. However, this can be subjective and time-consuming, particularly in multicentre studies. This work focuses on developing an automated QC pipeline, which aims to provide a quantitative measure of QC.Methods
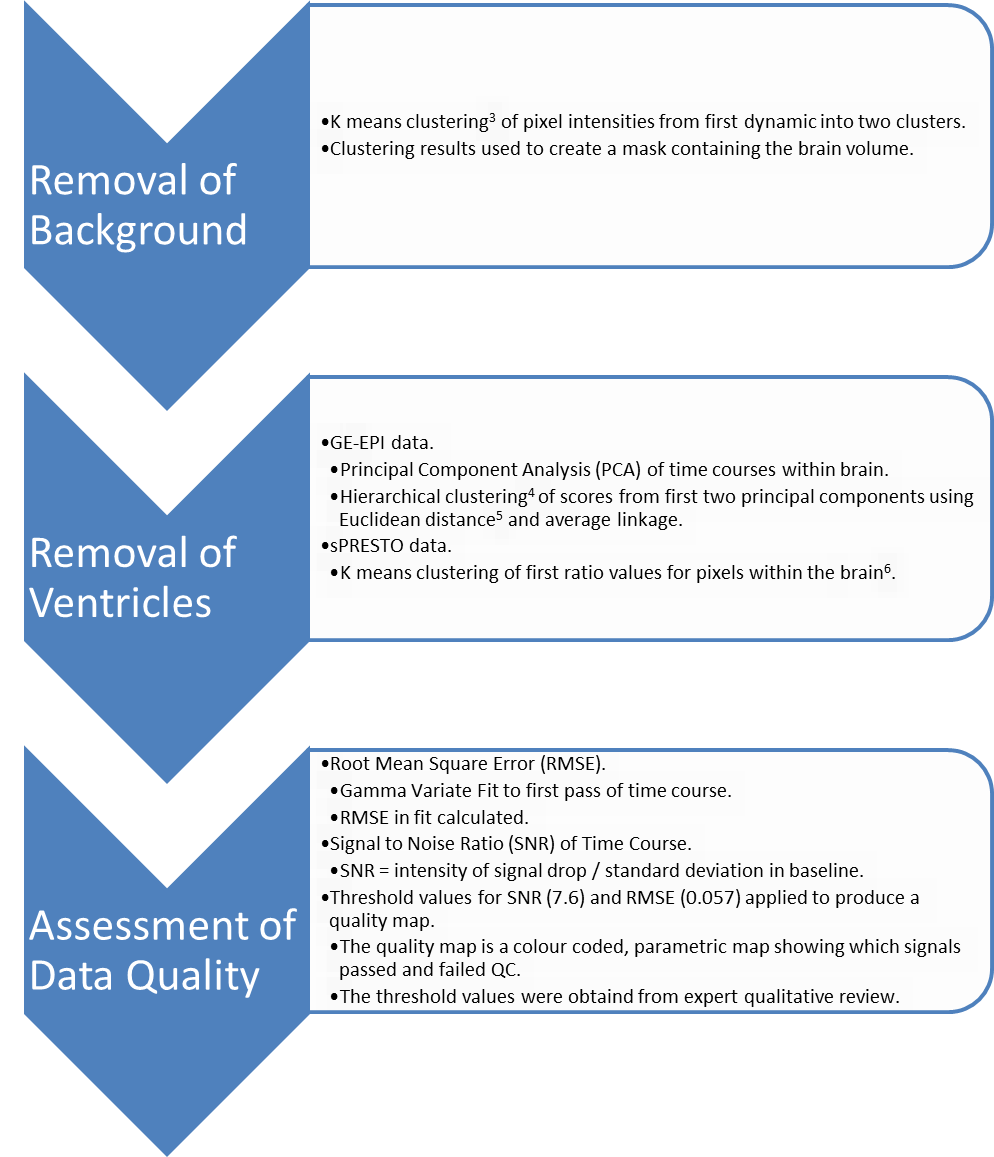
The QC pipeline was developed in Matlab 9.4. Anonymised scans from patients with cerebellar tumours were obtained from the CCLG functional imaging of tumours database, which contains patient scans from multiple centres with differing MR protocols. 34 patients were analysed, from four centres. Four consecutive slices, including the corpus callosum, were manually chosen from each data set. For data sets that didn’t include the corpus callosum in the field of view, the top four slices were used. Figure 1 shows the QC pipeline. Ventricle segmentation differed between the two protocols, due to reduced contrast in sPRESTO data. Pipeline outputs included parametric maps of signal-to-noise-ratio (SNR), root-mean-square error (RMSE), rCBV and a quality map.Results
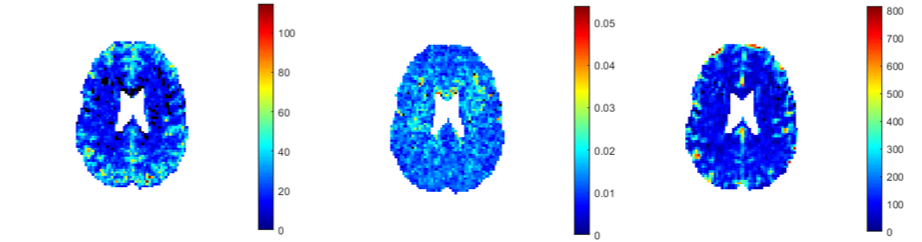
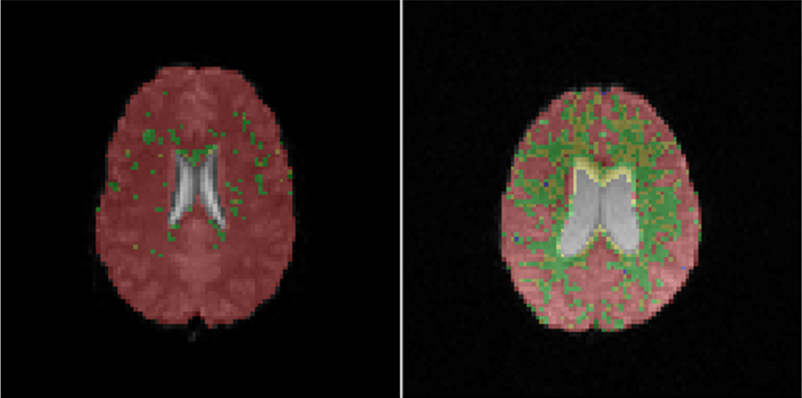
The automated QC code segmented and created parametric maps for all 34 data sets. Figure 2 shows example maps produced by the algorithm for one slice. Figure 3 shows quality maps overlaid onto brain, for data acquired at different field strengths. Table 1 shows quality parameters and rCBV values, grouped by centre and protocol.Discussion
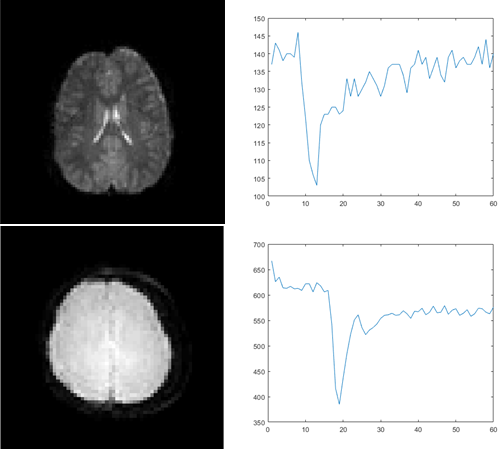
Figure 1 shows larger RMSE and lower SNR in white matter (WM) than grey matter (GM), which is expected as WM is less perfused; therefore it is more affected by noise. From table 1, the worst-performing data is 1.5T data from centre 1, suggesting that 1.5T acquisition with pre-bolus results in poor SNR. When a pre-bolus was used, the total dose was split between the pre-bolus dose and the main dose, resulting in a reduced main dose. The best-performing data is from centre 3, giving the largest SNR and highest percentage of pixels passing. Centre 3 is the only 3T GE-EPI data that does not have any pre-bolus, boosting SNR, and the percentage of pixels passing. The lack of pre-bolus may explain why sPRESTO equals or outperforms GE-EPI in centres 1 and 4. Although sPRESTO has high SNR in these cases, this comes at the cost of spatial resolution and image contrast. Figure 4 shows a comparison of sPRESTO and GE-EPI data, showing sPRESTO gives poor contrast between GM, WM and ventricles, and that the spatial resolution of sPRESTO datasets is poor. The sPRESTO sequence is also reported to have poorer temporal resolution than the EPI sequence7.
SNR from table 1 shows a correlation with rCBV, as larger SNR gives a larger signal drop. There is also an inverse correlation between SNR and RMSE. TR, TE, flip angle and voxel volume appears to have less effect on data quality. Each centre gives similar average coverage, other than centre 3, as the field of view is focussed on the cerebellum. Although it has better SNR the whole brain isn’t in the field of view, meaning the whole tumour may not be covered.
Normalised rCBV is smaller for sPRESTO data sets, showing greater similarity between rCBV values of passed and failed pixels. Standard deviations in rCBV for failed pixels are large compared to average rCBV showing the importance of good SNR and how it affects biomarker accuracy. The standard deviation for passed pixels is large, due to the inclusion of GM and WM.
Conclusion
This work demonstrates an automated QC pipeline, tested on healthy slices of brain acquired using a range of different protocols. The results show that 1.5T acquisition with a pre-bolus results in too many pixels being discarded. It shows the importance of good SNR in achieving robust biomarkers. It also shows some of the compromises involved in DSC-MRI acquisition. For example, choosing between GE-EPI and sPRESTO means compromising either on signal quality or image contrast, whilst splitting the Gd bolus reduces SNR. These factors should be taken into account when designing protocols for multi-centre use.Acknowledgements
This work was funded by EPSRC through a studentship from the Sci-Phy-4-Health CDT (EP/L016346/1) and the National Institute for Health Research (NIHR) via a research professorship (13-0053) and Help Harry Help Others Cure.References
[1] Shiroishi, Mark S., et al. "Principles of T2*‐weighted dynamic susceptibility contrast MRI technique in brain tumor imaging." Journal of Magnetic Resonance Imaging 41.2 (2015): 296-313.
[2] Withey, Stephanie., et al. “Multicentre pediatric brain tumour dynamic susceptibility contrast (DSC-) MRI with contrast agent leakage correction.” Proceedings of the Joint Annual Meeting ISMRM-ESMRMB 2018 June 16-21, Paris, Abstract No. 5418
[3] MacQueen, James. "Some methods for classification and analysis of multivariate observations." Proceedings of the fifth Berkeley symposium on mathematical statistics and probability. Vol. 1. No. 14. 1967.
[4] Patel, Sakshi, Shivani Sihmar, and Aman Jatain. "A study of hierarchical clustering algorithms." Computing for Sustainable Global Development (INDIACom), 2015 2nd International Conference on. IEEE, 2015.
[5] Pandit, Shraddha, and Suchita Gupta. "A comparative study on distance measuring approaches for clustering." International Journal of Research in Computer Science 2.1 (2011): 29-31.
[6] Kao, Yi‐Hsuan, et al. "Removal of CSF pixels on brain MR perfusion images using first several images and Otsu's thresholding technique." Magnetic resonance in medicine 64.3 (2010): 743-748.
[7] van Gelderen, Peter, et al. "The PRESTO technique for fMRI." NeuroImage 62.2 (2012): 676-681.
Figures