5023
Quantifying Blood Flow of Rat Spinal Cord Injury Using in vivo Flow-sensitive Alternating Inversion Recovery (FAIR)1Biomedical Engineering, Marquette University & Medical College of Wisconsin, Milwaukee, WI, United States, 2Medical College of Wisconsin, Milwaukee, WI, United States, 3Neurosurgery, Medical College of Wisconsin, Milwaukee, WI, United States, 4Clement J. Zablocki Veterans Affairs Medical Center, Milwaukee, WI, United States
Synopsis
Perfusion weighted MRI has been widely used as a non-invasive MR biomarker in brain imaging but its application to spinal cord imaging has been limited due to the inherent difficulties. In this study, we evaluated flow-sensitive alternating inversion recovery to quantify spinal cord blood flow (SCBF) in rat spinal cord with varying severities of contusion injury. A trend of decreasing SCBF was observed with greater injury severity, suggesting that arterial spin labeling may be useful as a reliable non-invasive indicator of spinal cord traumatic injury. Furthermore, T1 values demonstrated greater sensitivity to injury severity and functional outcomes.
Introduction
The purpose of this study was to quantify spinal cord blood flow (SCBF) in a rat spinal cord contusion injury model. Maintaining blood flow and perfusion to the injured cord is one of the important clinical recommendations for spinal cord trauma, but methods for noninvasive monitoring are limited. Arterial spin labelling (ASL) has been widely used for the brain to quantify cerebral blood flow. However, the application of this technique has been limited in the spinal cord, in part, due to the challenges of imaging the cord such as motion and susceptibility artifacts1 as well as the complex nature of spinal cord vasculature2-4. In this study, we investigated flow-sensitive alternating inversion recovery (FAIR) to quantify SCBF and evaluated its potential as a MR biomarker of spinal cord contusion injury, hypothesizing that SCBF measured at the epicenter of injury would relate to the severity of the injury.Methods
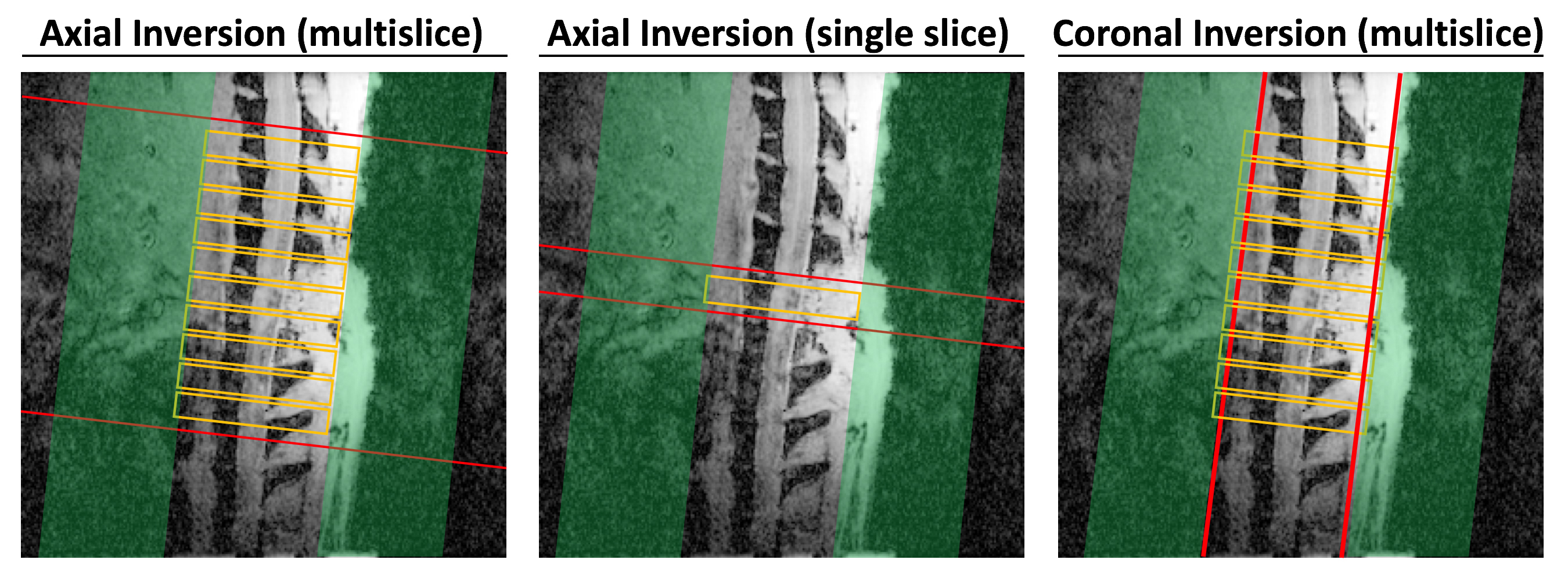
A sham (n=8), mild (n=10), moderate (n=10), or severe (n=10) contusion injury was induced at the T10 thoracic vertebral level in 38 female Sprague-Dawley rats. All Imaging was performed at 1 day post injury (24 hrs) on a Bruker 9.4T MRI system using a 2x2 surface coil for signal reception. The injured epicenter was identified on a sagittal T1-weighted image (TE=4 ms; TR=122 ms). FAIR- images were acquired using a 4-shot echo-planar spin-echo readout (TE=18 ms; Constant recovery time=3000 ms; In-plane resolution=165 µm2; Slice thickness=2 mm). Ten inversion times (TI) ranging from 50 ms to 7500 ms were used for both slice-selective and non-selective inversion recovery images. A single-slice axial inversion was used as the reference standard compared to prior studies5,6. To differentiate inflow effects and examine the possibility for multi-slice imaging, axial and coronal inversion slabs were used with slices acquired in a burst mode similar to OPTIMAL FAIR7 (Fig. 1). Images were fit to an inversion recovery exponential equation to obtain T1 parameters. Manual ROI analysis to quantify T1 values in the cord tissue, and subsequently SCBF values (mL/100 g/min) using the equation (1/T1ss = 1/T1ns + f/λ) where T1ss and T1ns are T1-relaxation time constants of slice-selective and non-selective inversion images, respectively. Pearson’s product moment correlations were used to examine the relationship between MRI metrics and behavioral assessments for locomotion (Basso, Beattie and Bresnahan score; BBB)8.Results
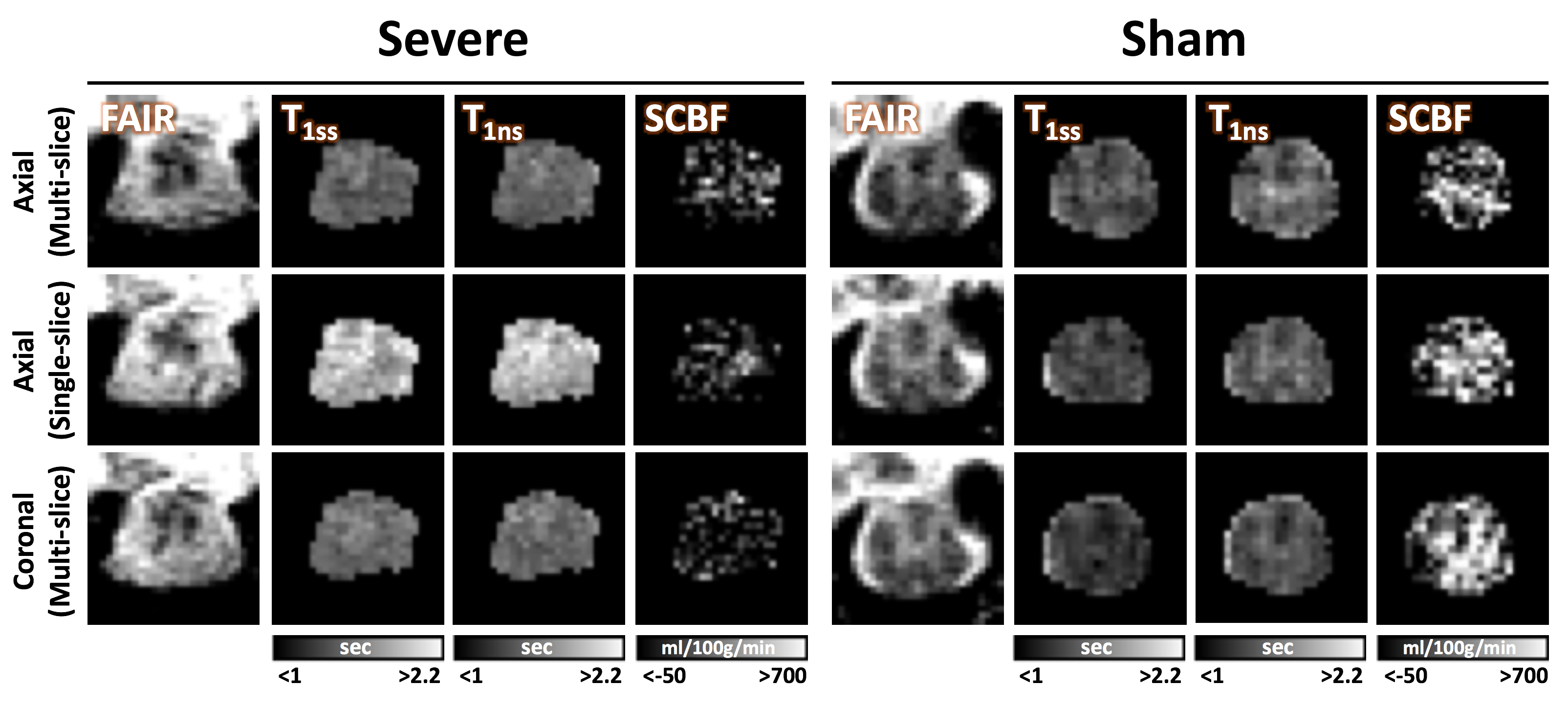
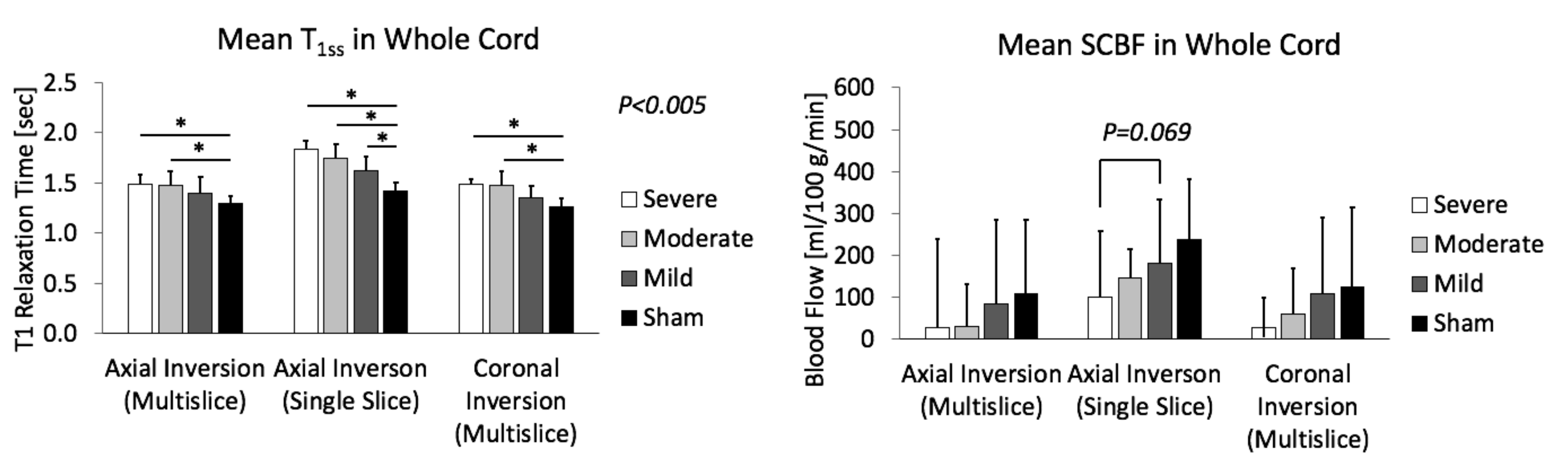
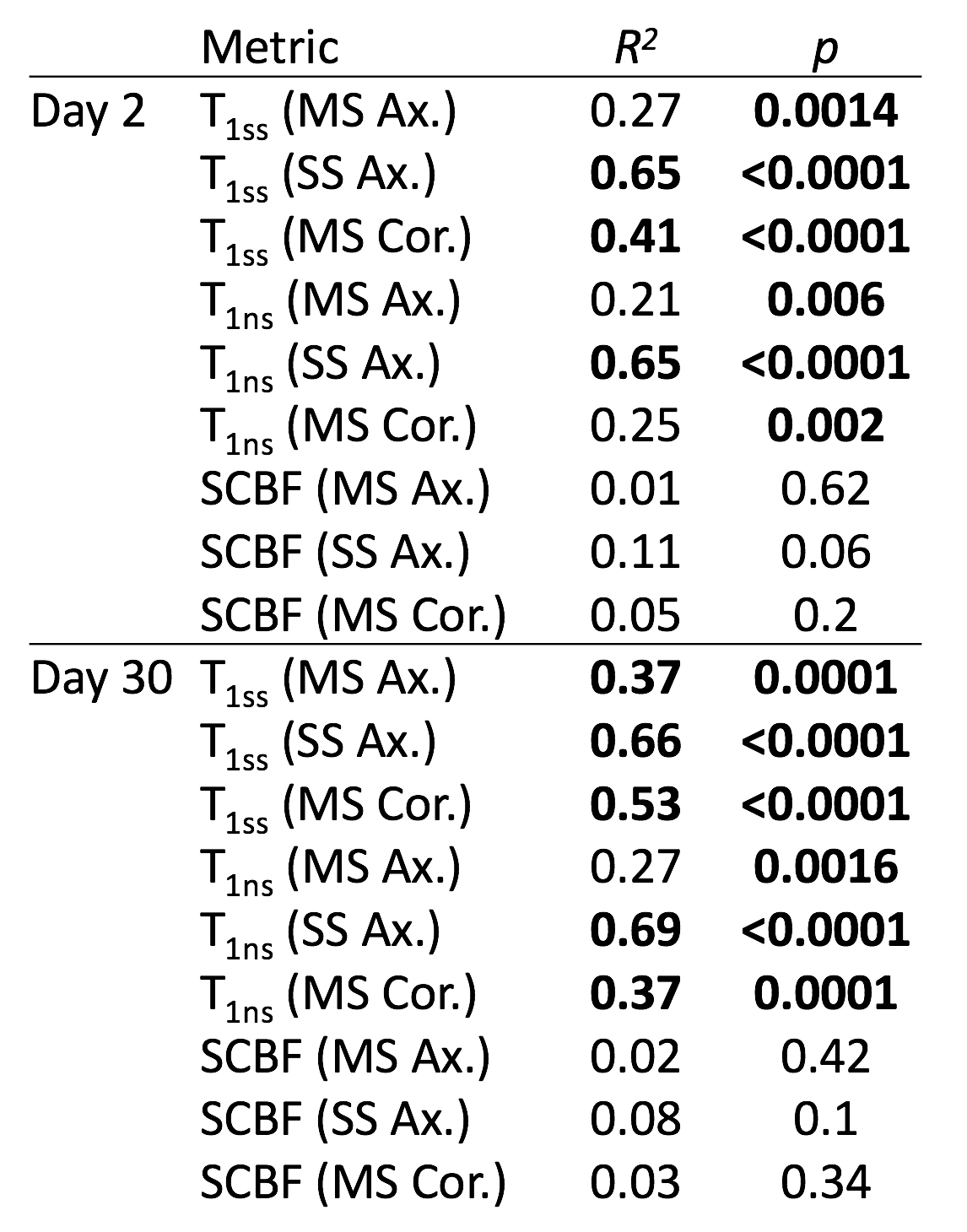
With increasing severity of the injury, T1ss and T1ns values were found to be higher at the epicenter in both axial and coronal inversion schemes (Fig. 2 & 3). SCBF decreased at the injury epicenter with greater severity. The descending trends of T1ss and SCBF across injury severities are clearly seen for all the inversion schemes (Fig. 3). Irrespective of inversion orientation, multi-slice results showed relatively lower blood flow values than the single slice. Strong positive correlations were found between locomotor function and T1 relaxation time constant while no significant correlation was present between the SCBF values and BBB score (Fig. 4). Among the different inversion schemes, single slice axial inversion showed the strongest correlate of BBB score with all metrics compared to multi-slice axial or coronal inversion.Conclusion
This study showed that spinal cord FAIR can be used as a biomarker of spinal cord injury. In all inversion experiments, estimated SCBF at the injury epicenter decreased as the injury severity increased. Results also indicate that both T1ss and T1ns values at the acute stage of injury were strong predictors of outcome especially when using single slice axial inversion. The limitation of this study, however, is the variability in estimated SCBF values, in part due to complications from motion artifacts and limited SNR. Future efforts to employ more efficient and sensitive ASL methods, such as pseudo-continuous ASL or velocity-selective ASL may be useful to improve the accuracy and spatial resolution of SCBF estimates with MRI in the spinal cord.Acknowledgements
This work was supported in part by Merit Review Award I01 RX001497 from the US Department of Veterans Affairs Rehabilitation Research and Development Service.References
1. Stroman PW, Wheeler-Kingshott C, Bacon M, et al. The current state-of-the-art of spinal cord imaging: methods. Neuroimage. 2014 Jan 1;84:1070-81.
2. Amato ACM, Stolf NAG. Anatomy of spinal blood supply. J Vasc Bras. 2015 July-Sept.; 14(3):248-252
3. Melissano G, Bertoglio L, Rinaldi E, et al. An anatomical review of spinal cord blood supply. J Cardiovasc Surg (Torino). 2015 Oct;56(5):699-706.
4. Gillilan LA. The arterial blood supply of the human spinal cord. J Comp Neurol. 1958 Aug;110(1):75-103.
5. Duhamel G, Callot V, Decherchi P, et al. Mouse lumbar and cervical spinal cord blood flow measurements by arterial spin labeling: sensitivity optimization and first application. Magn Reson Med. 2009 Aug;62(2):430-9.
6. Duhamel G, Callot V, Cozzone PJ, et al. Spinal cord blood flow measurement by arterial spin labeling. Magn Reson Med. 2008 Apr;59(4):846-54.
7. Li X, Sarkar SN, Purdy DE, et al. Anteroposterior perfusion heterogeneity in human hippocampus measured by arterial spin labeling MRI. NMR Biomed. 2013 Jun;26(6):613-21.
8. Basso DM, Beattie MS, Bresnahan JC. A sensitive and reliable locomotor rating scale for open field testing in rats. J Neurotrauma. 1995 Feb;12(1):1-21.
Figures