4980
Reproducibility of Simultaneous in vivo Blood T1 and T2 Imaging Method1Interdisciplinary Institute of Neuroscience and Technology, Qiushi Academy for Advanced Studies, College of Biomedical Engineering & Instrument Science, Zhejiang University, Hangzhou, China, 2Center for Magnetic Resonance Research, School of Medicine, University of Minnesota, Minneapolis, MN, United States, 3Division of Biostatistics, School of Public Health, University of Minnesota, Minneapolis, MN, United States, 4Laboratory of Integrative Human Physiology, School of Kinesiology, University of Minnesota, Minneapolis, MN, United States, 5Neuropsychology Section, Hennepin County Medical Center, Minneapolis, MN, United States, 6Berman Center for Clinical Research Hennepin Health Research Institute, Hennepin Healthcare, Minneapolis, MN, United States
Synopsis
The longitudinal and transverse relaxation time constants of blood vary across
subjects, developmental stages, physiological states or specific diseases. We
implemented a fast method for simultaneous in
vivo measurements of blood T1 and T2. Although such
an approach has been successfully demonstrated, its repeatability or robustness
has not been assessed. We performed a two-session study using our fast in vivo blood T1 and T2
imaging method, and the study results are reported in the following.
Purpose
The longitudinal and transverse relaxation time constants of blood are important parameters for MRI methods 1,2. Due to their variation across subjects and significant differences across developmental stages, physiological states or specific diseases 3-5, rapid in vivo measurements of blood T1 and T2 are needed to better facilitate diverse biomedical research studies 6-8. We implemented a fast imaging method for simultaneous in vivo measurements of blood T1 and T2 taking only about 25 s by combining the look-locker T1-weighted acquisition following an adiabatic saturation recovery and the blood-tagging-facilitated T2-weighted image acquisition using the MLEV T2 preparation 5. Although such an approach has been successfully demonstrated 9, its reproducibility has not been assessed. Therefore, we have performed a two-session study using our in vivo blood T1 and T2 imaging method, and the study results are reported below.Methods
The reproducibility study was performed on a Siemens 3T Prisma MRI scanner under an IRB-approved protocol with written informed consent. The body coil was used for RF transmission and a 32-channel head array for signal reception. Seven healthy volunteers were imaged with a previously implemented simultaneous blood T1 and T2 imaging method 9 in two sessions in the same day separated in time by 1 to 1.5 hours.
The sequence diagram of the relaxometry imaging method is presented in Figure 1A. The slabs for superior venous blood tagging using the PICORE method 10 and the imaging slice to measure the venous blood within the sagittal sinus are illustrated in Figure 1B. In brief, the T1-weighted image acquisitions were followed by T2-weighted label or control image acquisitions that were acquired in an interleaved fashion and sequentially for four effective TE times: 0, 40, 80 and 160 ms. The number of look-locker T1-weighted images acquired before the acquisitions of four T2-weighted label or control images were: 2, 4, 8, and 16. The major imaging parameters for single-shot EPI were as follows: FOV = 218 x 218 mm2; matrix size = 64 x 64; in-plane resolution = 3.4 x 3.4 mm2; slice thickness = 5 mm; TI1 = ΔTI = 200 ms; post-labeling delay = 1050 ms; and total acquisition time = ~ 25 s.
Post-processing, including 2D motion correction, was performed using the FSL toolbox, and model fittings for the estimates of blood T1 and T2 utilized the equations in Figure 1C and scripts implemented in MATLAB. The T1-weighted images acquired with the same saturation recovery time were co-registered and averaged before obtaining the means of venous blood signals within the sagittal sinus. Varying T1-weighting effects on the measured T2-weighted blood signals across four label or control images were compensated by using the estimated blood T1. Statistical analyses were performed using the GraphPad Prism software.
Results and Discussions
The blood T1 and T2 measurements from two sessions are presented in Figure 2, and are comparable to those in the literature 6-8. Figure 3 shows the scatter plots of blood T1 and T2 measurements from two sessions. The percentage differences of blood T1 and T2 measurements across two sessions are shown in Figure 4. These results indicate that the implemented rapid in vivo blood T1 and T2 imaging method can provide reproducible estimates of blood T1 and T2. The percentage differences of blood T1 and T2 measurements across two sessions were within 5%, suggesting that the implemented approach is able to accurately detect small differences and can be a useful tool for functional MRI studies. The long-term reproducibility of this approach will be assessed in the future.Conclusions
Our rapid simultaneous in vivo blood T1 and T2 imaging method can provide reproducible blood T1 and T2 measurements.Acknowledgements
P41 EB015894, P30 NS076408, UMF0003900, and UL1TR000114. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.References
- Detre JA, Leigh JS, Williams DS, Koretsky AP. Perfusion imaging. Magn Reson Med. 1992;23(1):37-45.
- Edelman RR, Chien D, Kim D. Fast selective black blood MR imaging. Radiology. 1991;181(3):655-660.
- Li W, Liu P, Lu H, Strouse JJ, van Zijl PCM, Qin Q. Fast measurement of blood T1 in the human carotid artery at 3T: Accuracy, precision, and reproducibility. Magn Reson Med. 2017;77(6):2296-2302.
- Qin Q, Strouse JJ, van Zijl PC. Fast measurement of blood T1 in the human jugular vein at 3 Tesla. Magn Reson Med. 2011;65(5):1297-1304.
- Xu F, Uh J, Liu P, Lu H. On improving the speed and reliability of T2-relaxation-under-spin-tagging (TRUST) MRI. Magn Reson Med. 2012;68(1):198-204.
- Jordan LC, Gindville MC, Scott AO, et al. Non-invasive imaging of oxygen extraction fraction in adults with sickle cell anaemia. Brain. 2016;139(Pt 3):738-750.
- Kety SS, Schmidt CF. The Effects of Altered Arterial Tensions of Carbon Dioxide and Oxygen on Cerebral Blood Flow and Cerebral Oxygen Consumption of Normal Young Men. J Clin Invest. 1948;27(4):484-492.
- Xu F, Ge Y, Lu H. Noninvasive quantification of whole-brain cerebral metabolic rate of oxygen (CMRO2) by MRI. Magn Reson Med. 2009;62(1):141-148.
- Zhang J, Wang D, Zhang X, Eberly LE, Metzger GJ, Dengel DR, Tupper D, Murray AM, Li X. Evaluation of A Method for Simultaneous in vivo Measurements of Blood T1 and T2. Proc. Intl. Soc. Mag. Reson. Med. 26 (2018): 2254.
- Wong EC, Buxton RB, Frank LR. Implementation of quantitative perfusion imaging techniques for functional brain mapping using pulsed arterial spin labeling. NMR Biomed. 1997;10(4-5):237-249.
Figures
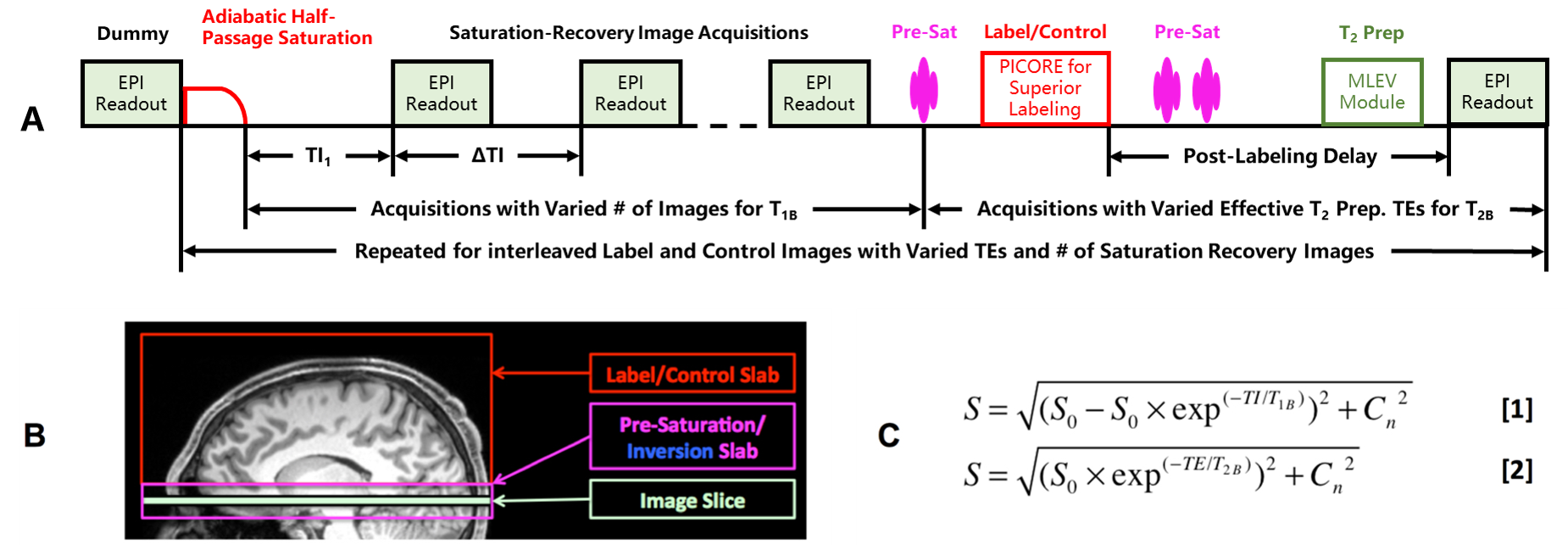
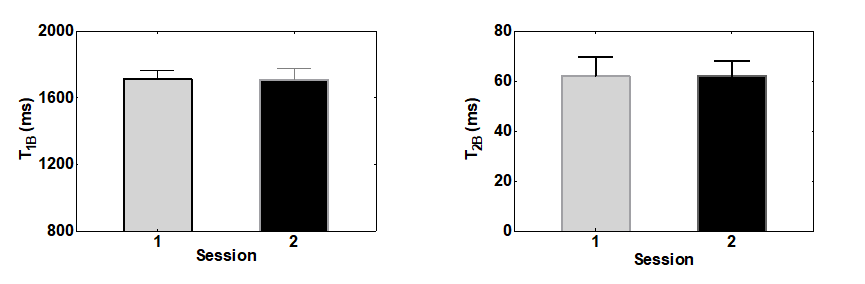
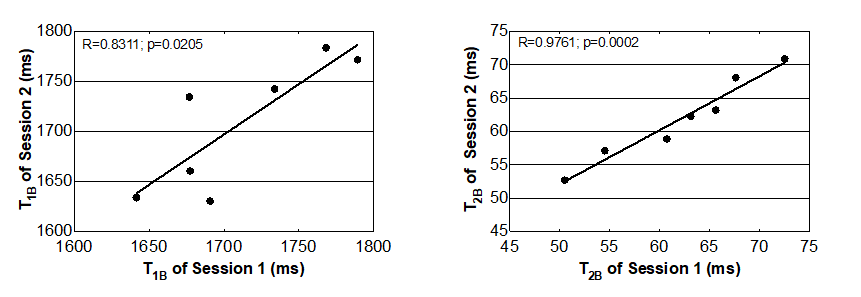
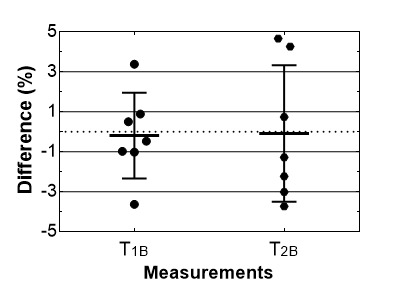
Figure 4. Percentage difference of T1 (T1B) and T2 (T2B) measurements across two sessions. Percentage difference was calculated using the difference and mean values of measurements from two sessions. Error bars represent standard errors.