4949
Enabling free-breathing renal pCASL with background suppression and motion correction: a comparison with paced-breathing1Center for Image Sciences, University Medical Center Utrecht, Utrecht, Netherlands, 2C.J.Gorter Center for High Field MRI, Leiden University Medical Center, Leiden, Netherlands, 3Department of Radiology, University Medical Center Utrecht, Utrecht, Netherlands
Synopsis
Renal perfusion imaging using arterial spin labeling (ASL) is challenged by respiratory motion and physiologic noise, often dealt with by breathing instructions requiring patient cooperation. We investigated if background suppression (BGS) combined with image registration, guided by the ASL-images themselves or additionally acquired fat-images, would enable free-breathing renal ASL. To this end, free-breathing ASL was compared with paced-breathing ASL, both including BGS and image registration. BGS and registration improved the quality of free-breathing renal pCASL, showing increased temporal SNR similar to paced-breathing ASL, without reducing perfusion-weighted signal. In conclusion, free-breathing renal pCASL is possible when employing BGS and image registration.
Introduction
Renal perfusion imaging using arterial spin labeling (ASL) MRI is challenged by respiratory motion and physiologic noise. To date, those challenges are dealt with by breath-holding and paced-breathing, requiring patient cooperation.1–4 However, free-breathing is desired as it alleviates the need for patient cooperation. For free-breathing (FB) renal ASL, retrospective realignment has been found essential to reduce subtraction artifacts3,5 and, independently, background suppression (BGS) has been demonstrated to reduce physiologic noise.1–3,6 Nevertheless, with the combination of image registration and BGS, negative results on ASL precision and accuracy have been reported.3 We investigated the effect of the BGS-level in combination with image registration on ASL signal quality, with registration either on the ASL-images themselves or guided by additionally acquired fat-images.7 To assess whether these measures permit FB renal ASL, results from FB acquisitions were compared with the reference paced-breathing (PB) motion compensation strategy, for both with BGS and image registration.Methods
Imaging: 10 volunteers (age
22–60, 3 men) were scanned on a 1.5T MRI (Ingenia, Philips, The Netherlands) using a 28-element
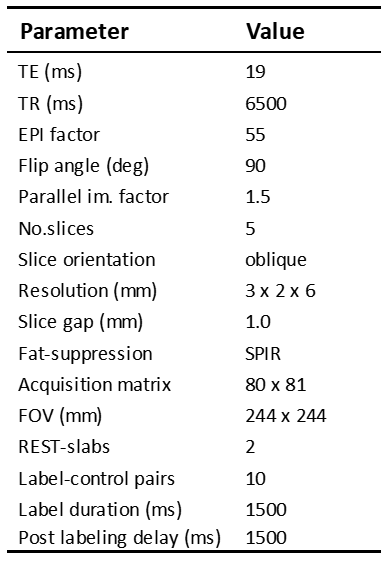
phased-array coil. Multi-slice 2D pseudo-continuous ASL (pCASL) was acquired
with a single-shot gradient echo EPI readout (see Table 1). Within the same
sequence, fat-images were acquired as introduced previously7 with the shortest
fat-signal recovery delay of 65ms. Five different BGS-levels were evaluated using
two or four inversion pulses with pulse timings [% suppression]: 1520/2400ms[70%] (BGS2m),
1520/2500ms[80%] (BGS2M), 1520/2600ms[90%]
(BGS2H), 1501/2320/2752/2943ms[90%] (BGS4H)4. All BGS
scans were acquired twice, in FB and PB. During PB subjects were asked to hold
their breath during labeling plus readout and to take a shallow breath after
the readout. For each volunteer an
equilibrium magnetization image (M0) was also acquired.
Analysis:
Registration was performed using the ASL-images themselves (ASLReg) or via
their corresponding fat-images (FatReg). The M0 was always co-registered to the
fat-images, as large contrast differences between the M0 and
BGS ASL-images challenged direct image registration and those results were compared
to direct M0-ASL registration by visual assessment. For ASL-quality assessment, the average perfusion-weighted
signal (PWS=∆M/M0) was reported as a surrogate for accuracy and mean voxel-wise
temporal SNR (tSNR) as a measure of precision.
The effect of BGS combined
with image registration for FB renal pCASL was evaluated based on the resulting
tSNR and PWS from FB scans with different BGS-levels, after ASLReg and FatReg. For
unbiased interpretation of the BGS effect on PWS, comparison to a reference was
performed. The reference PWS per subject was defined as the average PWS over all PB
BGS scans after ASLReg (PWSPBref). The difference with the
reference PWS was referred to as PWS-error which was evaluated as a function of
BGS. PWS-error can be caused by subtraction artifacts or PWS reduction; negative
sign possible. To assess feasibility of FB renal pCASL, tSNR and PWS
from FB and PB scans, after ASLReg and FatReg, were compared with the focus on NoBGS
and the most favorable BGS-level for ASL-quality. Statistical testing was done
using paired
Wilcoxon-signed-rank tests (α=0.05).
Results
From 10 volunteers, 1 was excluded due
to poor adherence to the PB protocol. M0 co-registration with FatReg
outperformed ASLReg with success rates of 100% and 54%, respectively.
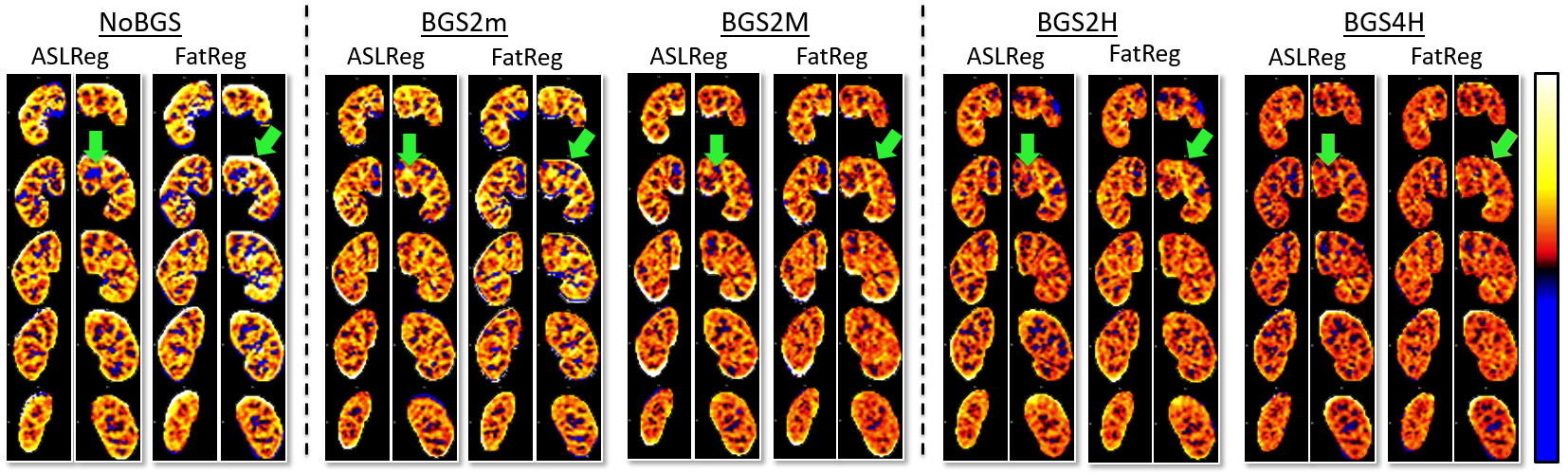
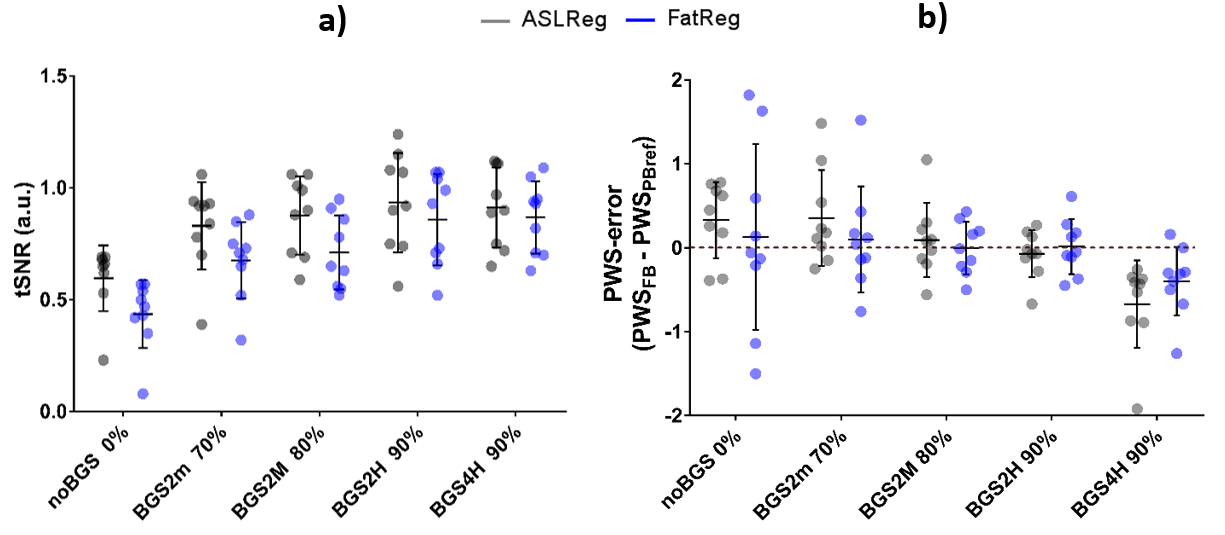
With BGS, there is a noticeable
reduction of the number of extreme values in PWS (Figure 1), which is accompanied with an
increase in tSNR and a smaller PWS-error (Figure
2). tSNR improvement was significant for
all BGS-settings compared to NoBGS, regardless of the image registration
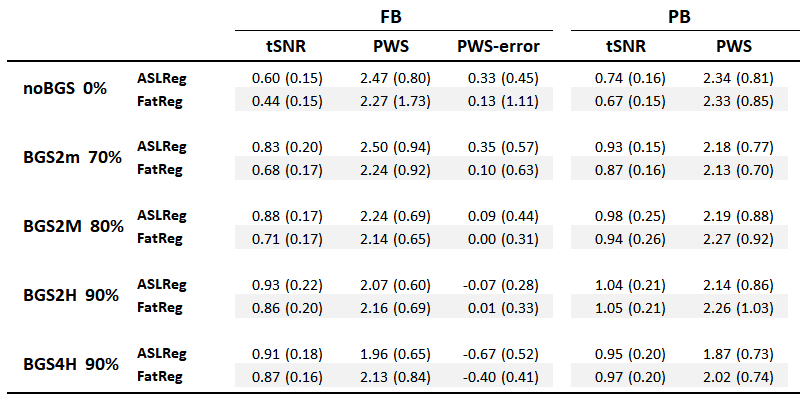
technique. Without BGS the tSNR was 0.60±0.15/0.44±0.15
and the PWS-error 0.33%/0.13% after ASLReg/FatReg, respectively. With BGS2H the
tSNR increased to 0.93±0.22/0.86±0.20 and
the PWS-error reduced to 0.07%/0.01%, with ASLReg/FatReg respectively. ASLReg yielded higher tSNR than FatReg
for NoBGS, however, this difference was substantially reduced when background
suppression was employed (Figure 2a).
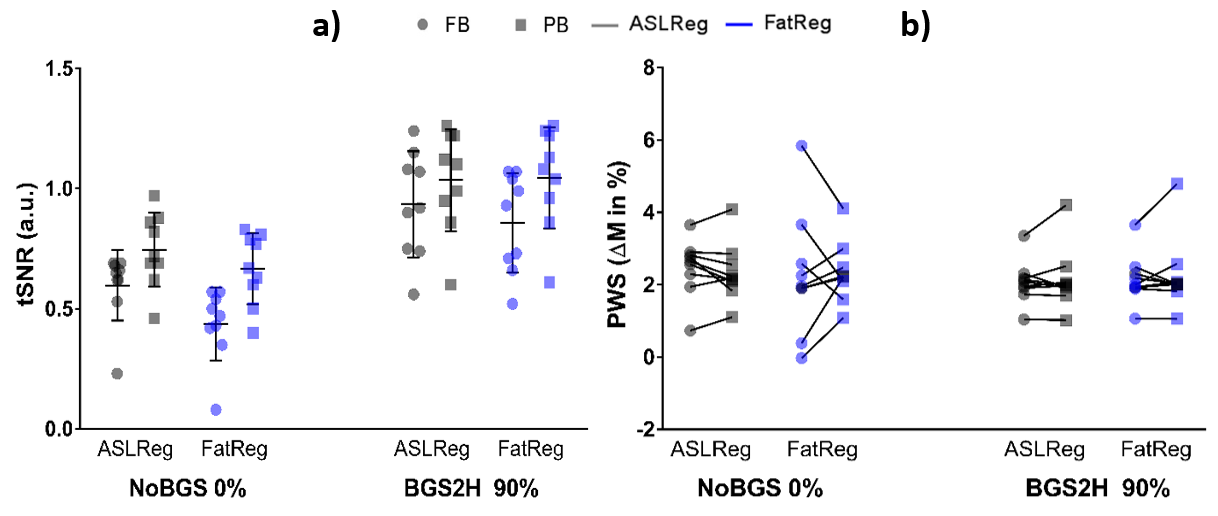
Figure
3
shows FB and PB results for NoBGS and BGS2H (results for all scans reported in Table
2),
allowing a comparison between breathing strategies. Using BGS2H, differences in
tSNR between FB and PB are reduced, independent of the registration technique. Moreover,
PWS is similar for the breathing strategies, without significant difference and
good intra-subject agreement (intra-subject variability: 0.35%/0.48% for ASLReg/FatReg).
Discussion & Conclusion
We found BGS highly beneficial for improving free-breathing renal pCASL precision without compromising accuracy, in combination with both the conventional ASLReg and our proposed FatReg method, although FatReg was advantageous for M0 co-registration. Finally, with the application of heavy BGS and image registration, free breathing renal pCASL has shown similar performance as the reference paced-breathing strategy, providing a clinically viable method for non-contrast renal perfusion imaging without the need for instructed breathing.Acknowledgements
This work is part of the research program Applied and Engineering Sciences with project number 14951 which is (partly) financed by the Netherlands Organization for Scientific Research (NWO). We thank MeVis Medical Solutions AG (Bremen, Germany) for providing MeVisLab medical image processing and visualization environment, which was used for image analysis.References
1. De Bazelaire C, Rofsky NM, Duhamel G, Michaelson MD, George D, Alsop DC. Arterial spin labeling blood flow magnetic resonance imaging for the characterization of metastatic renal cell carcinoma. Acad Radiol. 2005;12(3):347-357.
2. Robson PM, Madhuranthakam AJ, Dai W, Pedrosa I, Rofsky NM, Alsop DC. Strategies for reducing respiratory motion artifacts in renal perfusion imaging with arterial spin labeling. Magn Reson Med. 2009;61(6):1374-1387.
3. Gardener AG, Francis ST. Multislice perfusion of the kidneys using parallel imaging: Image acquisition and analysis strategies. Magn Reson Med. 2010;63(6):1627-1636.
4. Robson PM, Madhuranthakam AJ, Smith MP, et al. Volumetric Arterial Spin-labeled Perfusion Imaging of the Kidneys with a Three-dimensional Fast Spin Echo Acquisition. Acad Radiol. 2016;23(2):144-154.
5. Taso M, Guidon A, Alsop D. Influence of background suppression and retrospective realignment on free- breathing renal perfusion imaging using ASL. In: 26th Annual Meeting of ISMRM 2018: 2177.
6. Cutajar M, Thomas DL, Banks T, Clark CA, Golay X, Gordon I. Repeatability of renal arterial spin labelling MRI in healthy subjects. Magn Reson Mater Physics, Biol Med. 2012;25(2):145-153.
7. Bones IK, Harteveld AA, Franklin S, Osch MJP Van. Introducing a fat-image guided registration technique for image-based retrospective motion compensation for free-breathing background suppressed renal pCASL. In: 26th Annual Meeting of ISMRM 2018:2169.
8. Klein S, Staring M, Murphy K, Viergever MA, Pluim JPW. elastix : A Toolbox for Intensity-Based Medical Image Registration. 2010;29(1):196-205.
Figures