4912
In vivo inhomogeneous magnetization transfer (ihMT) outside the brain using radial ultra-short echo-time acquisitions1Radiology, Division of MR Research, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, United States, 2Aix Marseille Univ, CNRS, CRMBM, Marseille, France
Synopsis
Inhomogeneous magnetization transfer (ihMT) effects have been readily observed in myelinated structures. The advent of low duty-cycle ihMT to increase the signal allows application of ihMT in other tissues. In this work, we explore the feasibility of applying ihMT in non-myelinated tissues such as the heart, liver, and kidneys of mice. This is achieved using a radial, ultra-short echo-time acquisition for greater motion robustness. The results demonstrate a measurable ihMT signal outside the central nervous system. Thus the microstructure of such tissues might be assessed based on the dipolar order contribution to ihMT.
Introduction
From its inception, inhomogeneous magnetization transfer (ihMT) has been most associated with MRI of the central nervous system (CNS), as myelinated structures provide the greatest ihMT signal in vivo1,2. The ihMT signal equates to the difference between signal prepared with off-resonance RF irradiation applied at a single offset frequency, and that prepared with RF applied at both negative and positive versions of the offset frequency with equal power. With developed understanding that ihMT is sensitive to dipolar order3,4, and the increase of the ihMT signal achieved by the use of low duty-cycle preparations5,6, rigorous exploration of its use outside the central nervous system is warranted. In this work, we make use of a radial, ultra-short echo-time (UTE) acquisition, in part for its relative motion insensitivity7, and partly for the ability to probe components with short transverse relaxation times8, to measure ihMT in tissues outside the CNS of mice, including the heart, liver, and kidneys.Methods
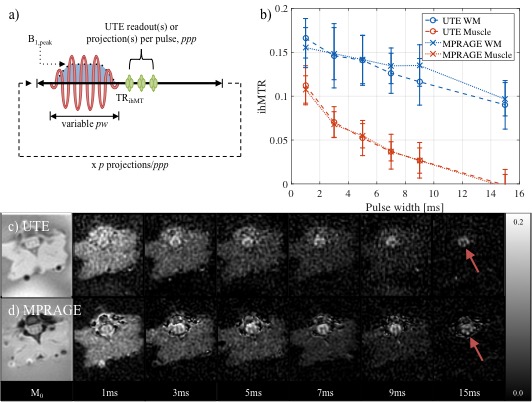
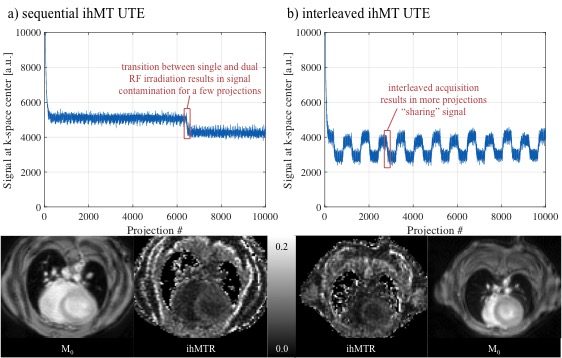
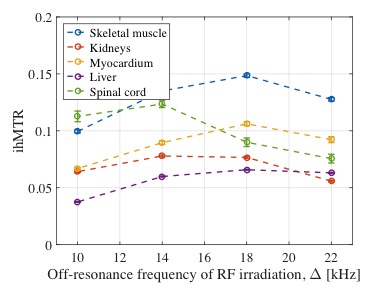
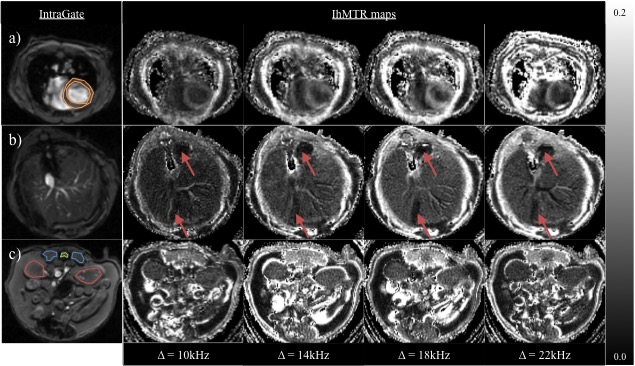
All experiments were conducted on a horizontal-bore 9.4T pre-clinical scanner using a 32mm transmit/receive volume coil. Use of a radial UTE free induction decay acquisition with the series of MT preparations required for ihMT (Fig. 1a), was first tested in an ex-vivo sample extracted at the spinal cord level from a Wistar rat. In vivo ihMT UTE data were compared to a magnetization prepared rapid gradient echo (MPRAGE) implementation to confirm ihMT ratios (ihMTRs) had the same response to increasing pulse widths, pw (i.e. decreasing duty-cycle) for the same power applied over TRihMT. IhMT UTE data were acquired in B6 mice. Acquisition of radial projections per image followed a golden angle ordering9. The ihMT UTE acquisition required repetition to increase signal-to-noise. Repetition of the MT preparations (i.e. single versus dual frequency RF irradiation) in a sequential manner was compared to that obtained in an interleaved order. The response of ihMTR to the off-resonance frequency of the MT pulses was examined in the 10 to 22kHz range, and guided acquisition of higher resolution data.Results
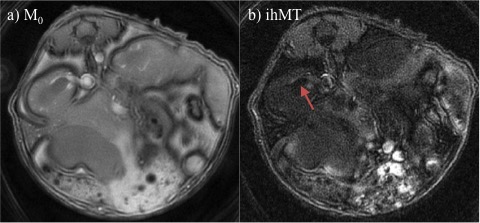
The ihMTRs obtained from the ihMT UTE acquisition in ex-vivo spinal cord and surrounding muscle were comparable to ihMTRs obtained with an MPRAGE implementation (Figs. 1b-d). Both sets of data showed the expected decay with pulse width, leaving only ihMT from the spinal cord at the longest pw of 15ms, owing to the high duty-cycle. A 40% decrease in the ihMTR contrast between myocardium and blood pool was measured going from sequential to an interleaved ihMT UTE cardiac acquisition (Fig. 2). The ihMTRs from different tissue types provided varying responses to changes in Δ (Figs. 3-4). Hypo-intensities in ihMTR maps of the liver (arrows in Fig. 4b) corresponded with hyper-intensities in T2-weighted images. Both skeletal and cardiac muscle peaked at Δ=18kHz, but the myocardial ihMTR was 30% lower. Interpolating the kidney ihMTR to peak at Δ=16kHz (Fig. 3), ihMT UTE at higher resolution allowed distinction between the medulla and pelvis of a kidney (arrow in Fig. 5).Discussion
Implementation of ihMT into a UTE sequence, particularly for applications outside the CNS, is open to optimization. An interleaved implementation can hamper the difference between signals following single or dual frequency RF irradiation on which ihMT is based, but allows selection/combination of ihMT data for greater temporal resolution (Fig. 2). The radial nature of the acquisition provides potential for further retrospective corrections based on respiration, or the cardiac cycle with increased ppp9. A measurable ihMT signal from different tissues might provide further and/or complementary insight into microstructure based on dipolar order.Conclusions
The use of ihMT outside the brain is feasible, and with a radial UTE free induction decay acquisition allows an application that is more robust to motion. As for CNS applications, optimization of the ihMT UTE sequence based on the tissue of interest is necessary.Acknowledgements
No acknowledgement found.References
1. Varma, G., Duhamel, G., De Bazelaire, C. & Alsop, D. C. Magnetization transfer from inhomogeneously broadened lines: A potential marker for myelin. Magn. Reson. Med. 73, 614–622 (2015).
2. Girard, O. M. et al. Magnetization transfer from inhomogeneously broadened lines (ihMT): Improved imaging strategy for spinal cord applications. Magn. Reson. Med. 77, 581–591 (2017).
3. Varma, G. et al. Interpretation of magnetization transfer from inhomogeneously broadened lines (ihMT) in tissues as a dipolar order effect within motion restricted molecules. J. Magn. Reson. 260, 67–76 (2015).
4. Manning, A. P., Chang, K. L., MacKay, A. L. & Michal, C. A. The physical mechanism of “inhomogeneous” magnetization transfer MRI. J. Magn. Reson. 274, 125–136 (2017).
5. Mchinda, S. et al. Whole brain inhomogeneous magnetization transfer (ihMT) imaging: Sensitivity enhancement within a steady-state gradient echo sequence. Magn. Reson. Med. 79, 2607–2619 (2018).
6. Varma, G. et al.Low duty-cycle pulsed irradiation reduces magnetization transfer and increases the inhomogeneous magnetization transfer effect. J. Magn. Reson. (2018). doi:10.1016/j.jmr.2018.08.004
7. Glover, G. H. & Pauly, J. M. Projection Reconstruction Techniques for Reduction of Motion Effects in MRI. Magn. Reson. Med. 28, 275–289 (1992).
8. Chang, E. Y., Du, J. & Chung, C. B. CME Article UTE Imaging in the Musculoskeletal System. 883, 870–883 (2015).
9. Winkelmann, S. & et al. An Optimal Radial Profile Order Based on the Golden Ratio for Time-Resolved MRI. IEEE Trans. Med. Imaging 26, 68–76 (2007).
Figures