4870
Preoperative prediction of pelvic lymph nodes metastasis in early-stage cervical cancer using radiomics model based on T2-weighted and diffusion-weighted MRI1Department of Radiology, Shaanxi Provincial People's Hospital, xi'an, China, 2Department of Medical Imaging, First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, China, 3School of Life Science and Technology, Xidian University, Xi’an, China
Synopsis
1. A radiomics nomogram for preoperatively predicting of PLN metastasis in patients with ECC was developed and validated.
2. The model displayed good performance (C-index=0.893 in primary cohort and C-index=0.922 in validation cohort).
3. The radiomics nomogram showed a significant improvement over the clinical nomogram in predicting PLN metastasis.
4. The radiomics signature derived from the combined T2WI and DWI has the best performance.
Introduction
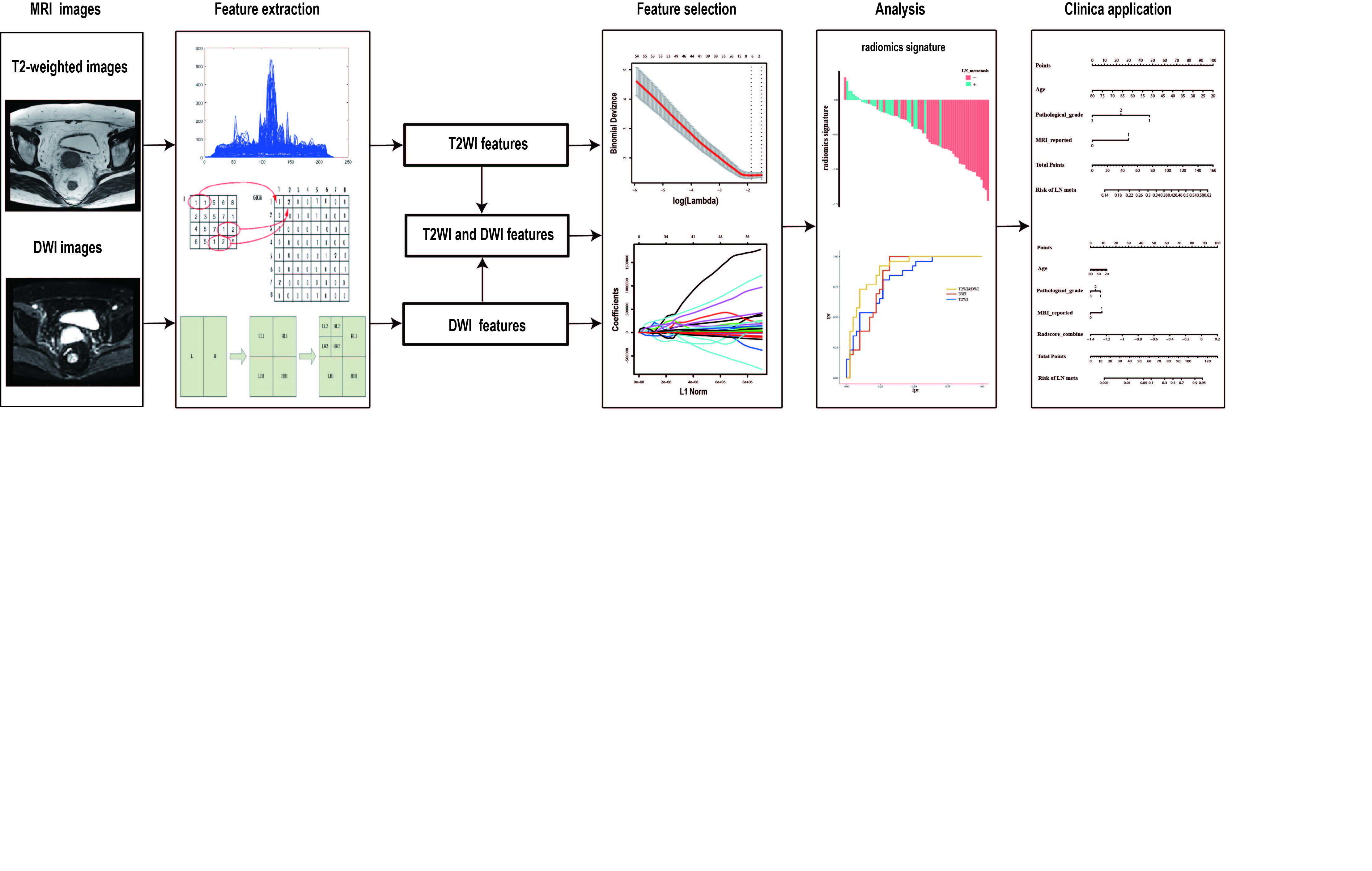
Pelvic lymph node (PLN) metastasis is one of the most significant prognostic factors in cervical cancer [1]. Knowing the accurate status of PLN metastasis preoperatively can help clinicians determine whether to perform a pelvic lymph node dissection (PLND), as well as which postoperative adjuvant therapy to use. In this study, we aim to develop and validate a noninvasive radiomics model based on T2WI and DWI for preoperatively predicting of PLN metastasis in patients with ECC.Methods
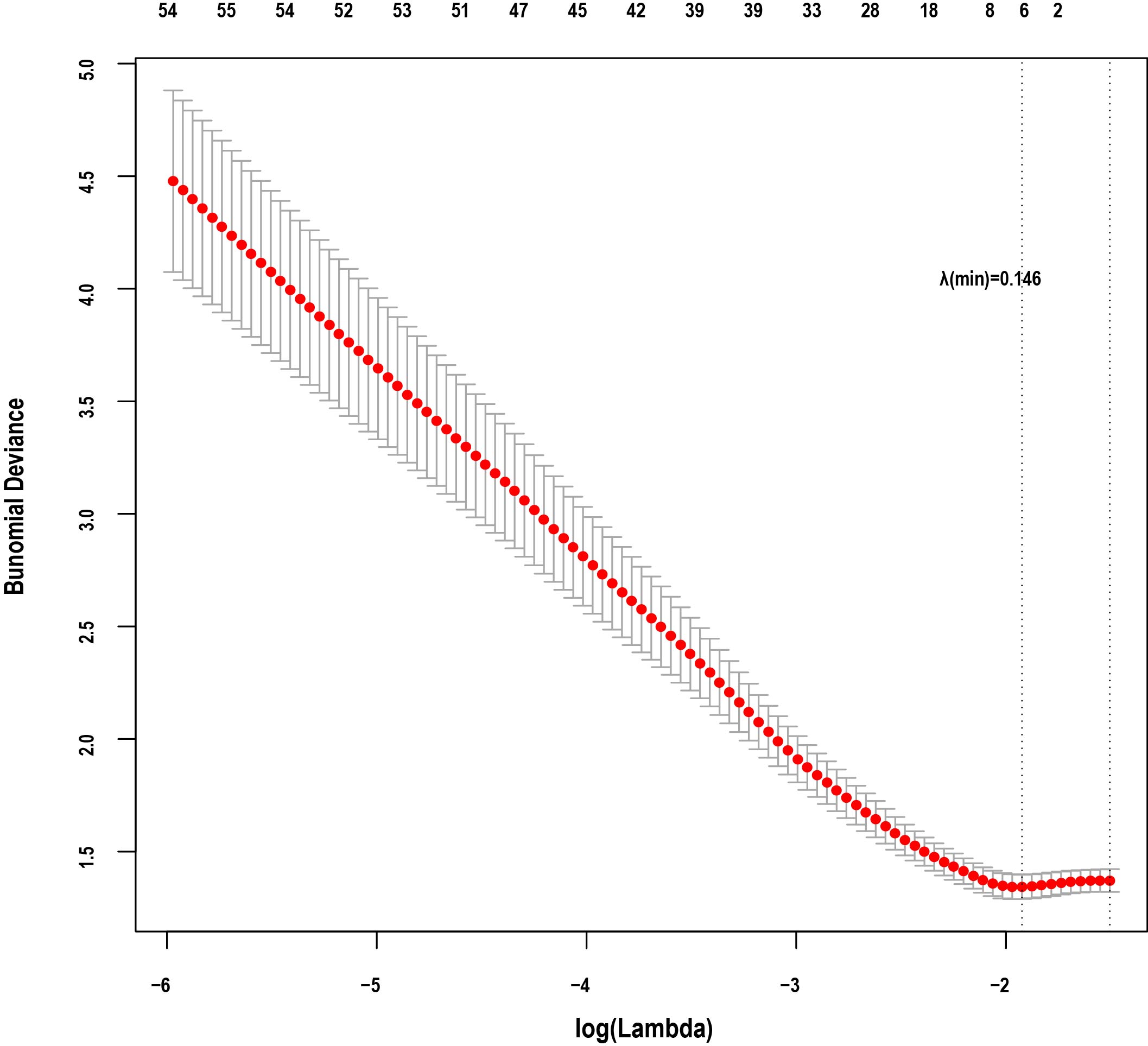
Ninety-six patients with ECC were enrolled in this study. All patients underwent T2WI and DWI scans before radical hysterectomy with PLN dissection surgery. Radiomics features extracted from T2WI and DWI were selected by least absolute shrinkage and selection operation regression for further radimoics signature calculation. The discrimination of this radiomics signature for PLN metastasis was then assessed using a support vector machine (SVM) model. Subsequently, a radiomics nomogram was constructed based on the radiomics signature and clinicopathologic risk factors using a multivariable logistic regression method. The performance of the radiomics nomogram for the preoperative prediction of PLN metastasis was evaluated for discrimination and calibration.Results
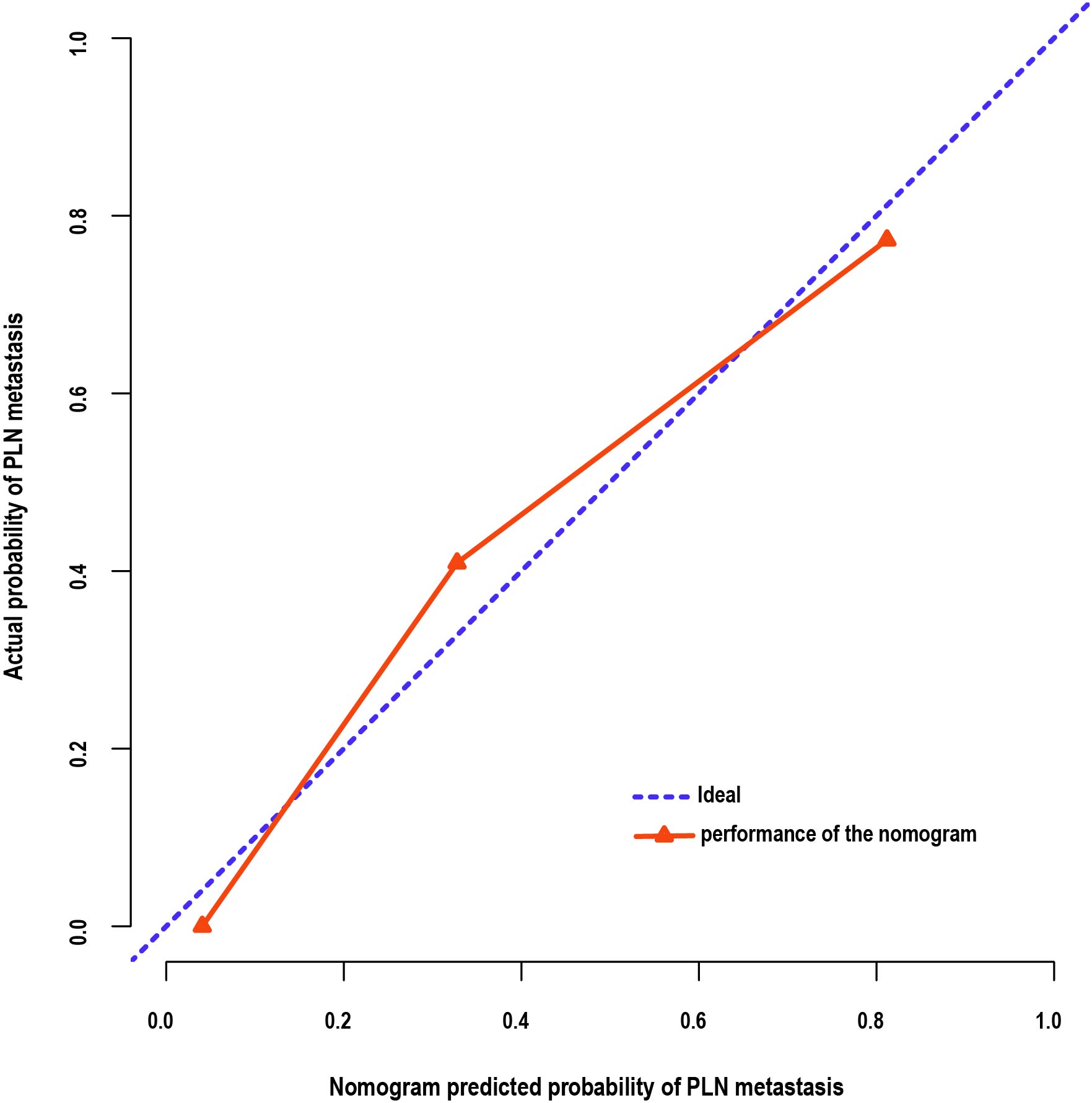
The radiomics signatures demonstrated a good discrimination for PLN metastasis. A radiomics signature derived from joint T2WI and DWI yielded higher AUC than the signatures derived from T2WI or DWI alone. For T2WI, DWI and joint T2WI and DWI, the radiomics signature yielded an AUC of 0.816(95% CI, 0.716-0.916), 0.830(95% CI, 0.732-0.928) and 0.893(95% CI, 0.817-0.970) respectively in the primary cohort, and 0.844(95% CI, 0.702-0.987), 0.870(95% CI, 0.733-1) and 0.909(95% CI, 0.801-1) respectively in the validation cohort. The radiomics nomogram integrating the radiomics signature with clinicopathologic risk factors showed a significant improvement over the nomogram based only on clinicopathologic risk factors in the primary cohort (C-index, 0.893 vs. 0.616; P=6.309 ) and validation cohort (C-index, 0.922 vs. 0.799; P=2.903 ).The calibration curves also showed good agreement.Discussion
Currently, accurate preoperative detection of PLN metastasis using conventional imaging (such as CT or MRI scans) is still a challenge in clinical settings[2]. CT and MRI have the same limitation in detecting lymph node metastasis—the only recognized criterion for diagnosing lymph node metastasis is that the shortest axis of the lymph node is greater than 1 cm, and this limitation would easily lead to some missed diagnosis of lymph node micro-metastasis.
Although pelvic lymph node dissection is the standard criterion to evaluate the lymph nodal status of cervical cancer, it results in operation time increase and also is associated with some serve short- and long-term complications[3]. Clinically, a reliable and effective method for preoperative prediction PLN metastasis in patients with early-stage cervical cancer is needed.
Radiomics has been proved to be able to help facilitate cancer staging, diagnosis and prognosis via characterising intratumour heterogeneity on the basis of quantitative image features derived from routine medical imaging[4]. In this study, the radiomics features from combine T2-weighted and diffusion-weighted MRI demonstrated favorable discrimination in both the primary (AUC=0.885) and validation cohorts (AUC=0.890). A set of 8 potential features that are strongly associated with PLN metastasis status were selected from a total of 2092 candidate radiomics features extracted from combined T2WI and DWI by using a LASSO logistic regression model.
T2WI can show higher resolution of tumour anatomical characteristics, such as shape and size, because of its excellent contrast resolution in soft tissue. In addition, as a functional imaging technique, DWI enables the noninvasive characterization of biological tissues based on the random translational molecular motion of water molecules.Textural features from DWI have been proved to be useful for prediction of lymph node metastasis in cervical cancer[5]. Therefore, the features extracted from combination of T2WI and DWI could take full advantages of each other and reflect much more detailed and comprehensive information of the tumours. Accordingly the radiomics signature based on joint T2WI and DWI could provide a more accurate prediction of PLN metastasis.Different from the traditional methods, radiomics nomogram offers a noninvasive and low-cost method for clinical use of assessing the risk of lymph node metastasis before surgery and helping clinicians to make optimal surgery decision for patients.With radiomics method, we could get rid of this limitation for extracting information of lymph node metastasis from tumour imaging analysis.
Conclusion
We developed and validated an effective and easy-to-use radiomics model based on T2WI and DWI for the preoperative prediction of PLN metastasis in patients with early-stage cervical cancer. This new approach provides a noninvasive and reliable tool to help make individualized treatment planning in patients with early-stage cervical cancer.Acknowledgements
NoneReferences
[1] Small Jr, W., Bacon, M. A., Bajaj, A., Chuang, L. T., Fisher, B. J., Harkenrider, M. M., Jhingran, A., Kitchener, H. C., Mileshkin, L. R. & Viswanathan, A. N. J. C. (2017) Cervical cancer: a global health crisis. 123, 2404-2412.
[2] Testa, A. C., Di Legge, A., De Blasis, I., Moruzzi, M. C., Bonatti, M., Collarino, A., Rufini, V., Manfredi, R. J. B. p., obstetrics, r. C. & gynaecology (2014) Imaging techniques for the evaluation of cervical cancer. 28, 741-768.
[3]Gien, L. & Covens, A. J. J. o. s. o. (2009) Lymph node assessment in cervical cancer: prognostic and therapeutic implications. 99, 242-247.
[4] Gillies, R. J., Kinahan, P. E. & Hricak, H. J. R. (2015) Radiomics: images are more than pictures, they are data. 278, 563-577.
[5] Schob, S., Meyer, H. J., Pazaitis, N., Schramm, D., Bremicker, K., Exner, M., Höhn, A. K., Garnov, N., Surov, A. J. M. I. & Biology (2017) ADC histogram analysis of cervical cancer aids detecting lymphatic metastases—a preliminary study. 19, 953-962.
Figures
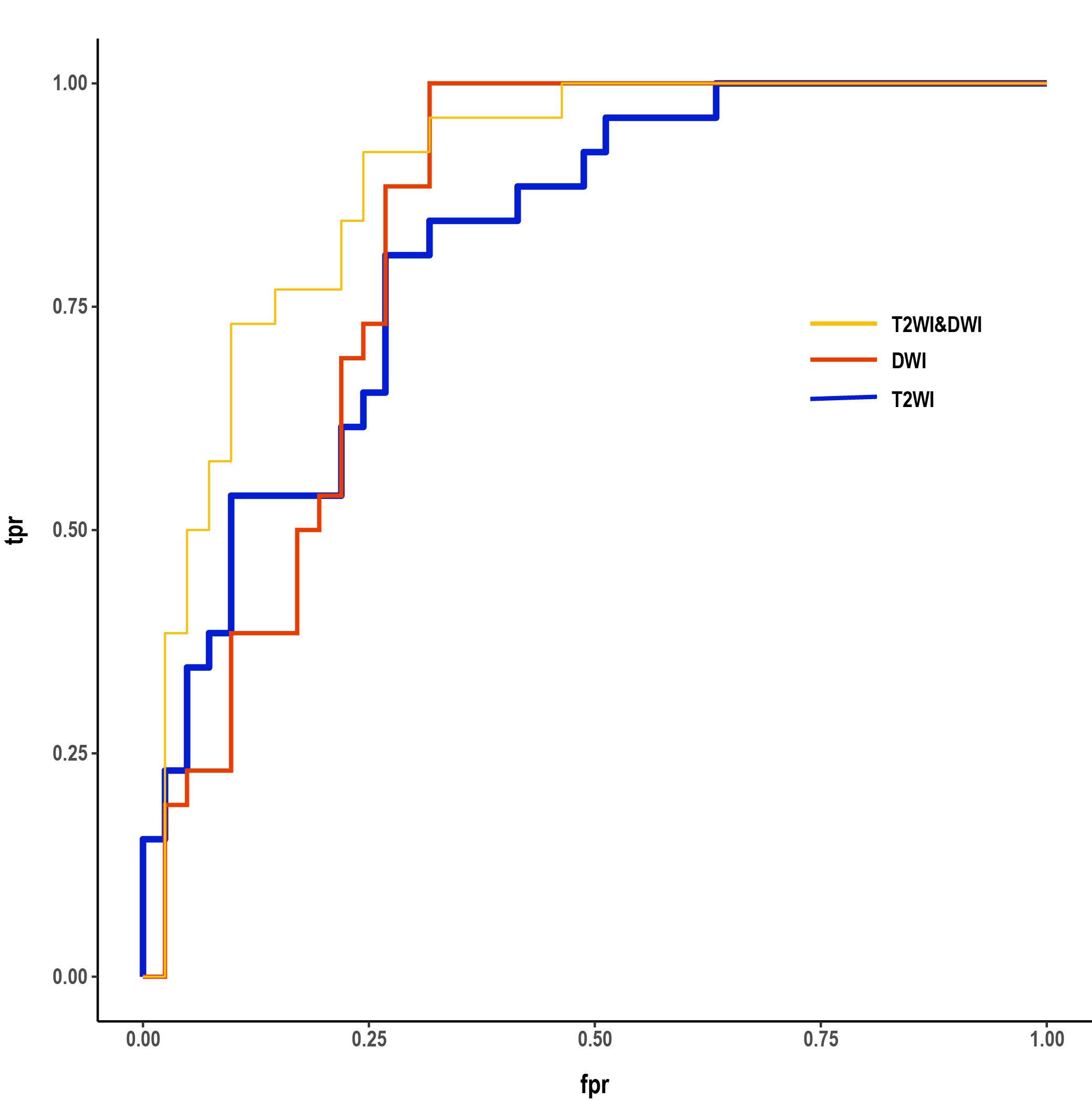
ROC curves of SVM models for radiomics signatures from T2WI, DWI, joint of T2WI and DWI, respectively.ROC curves in the primary cohort.
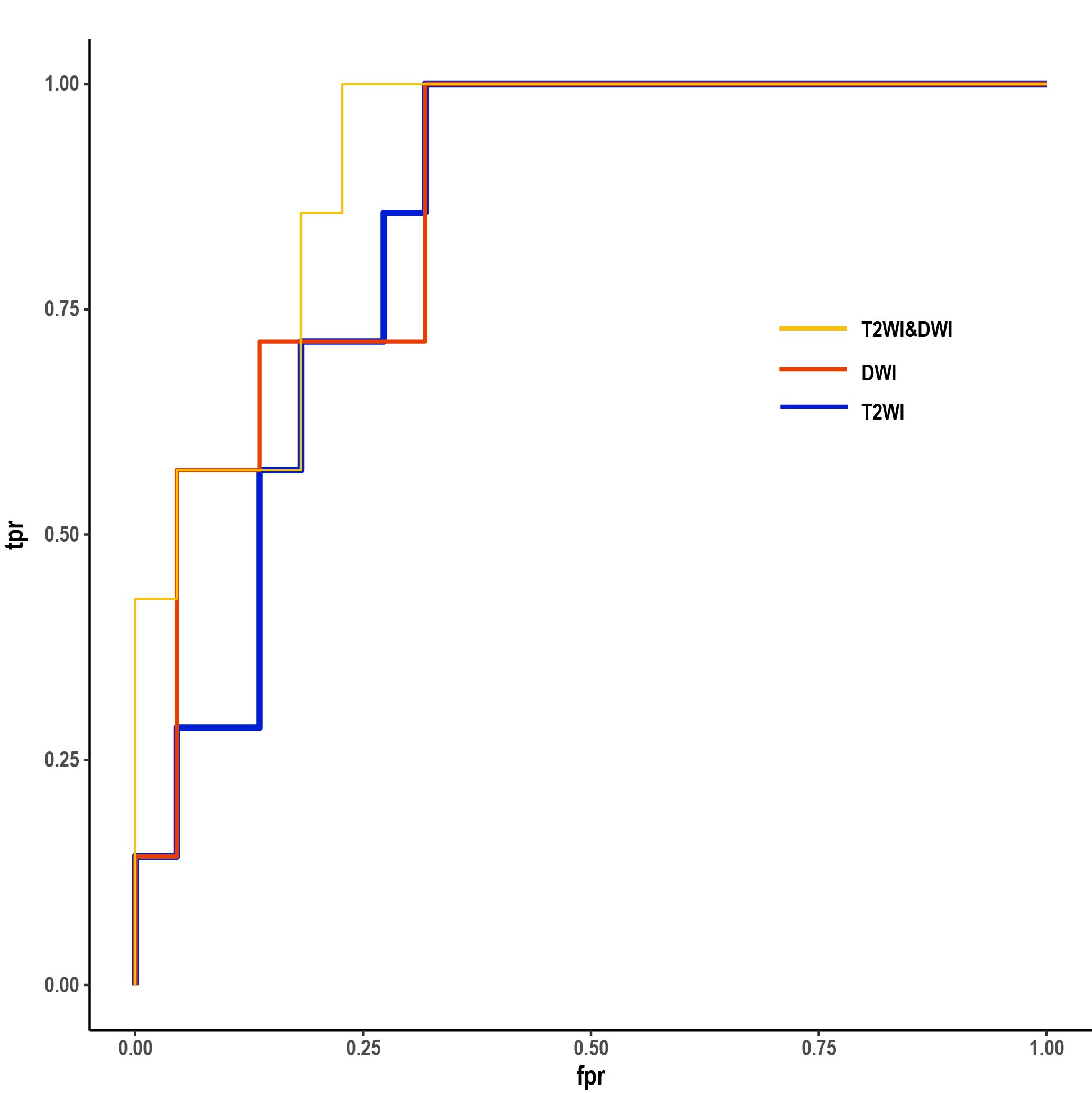
ROC curves of SVM models for radiomics signatures from T2WI, DWI, joint of T2WI and DWI, respectively.ROC curves in the validation cohort.
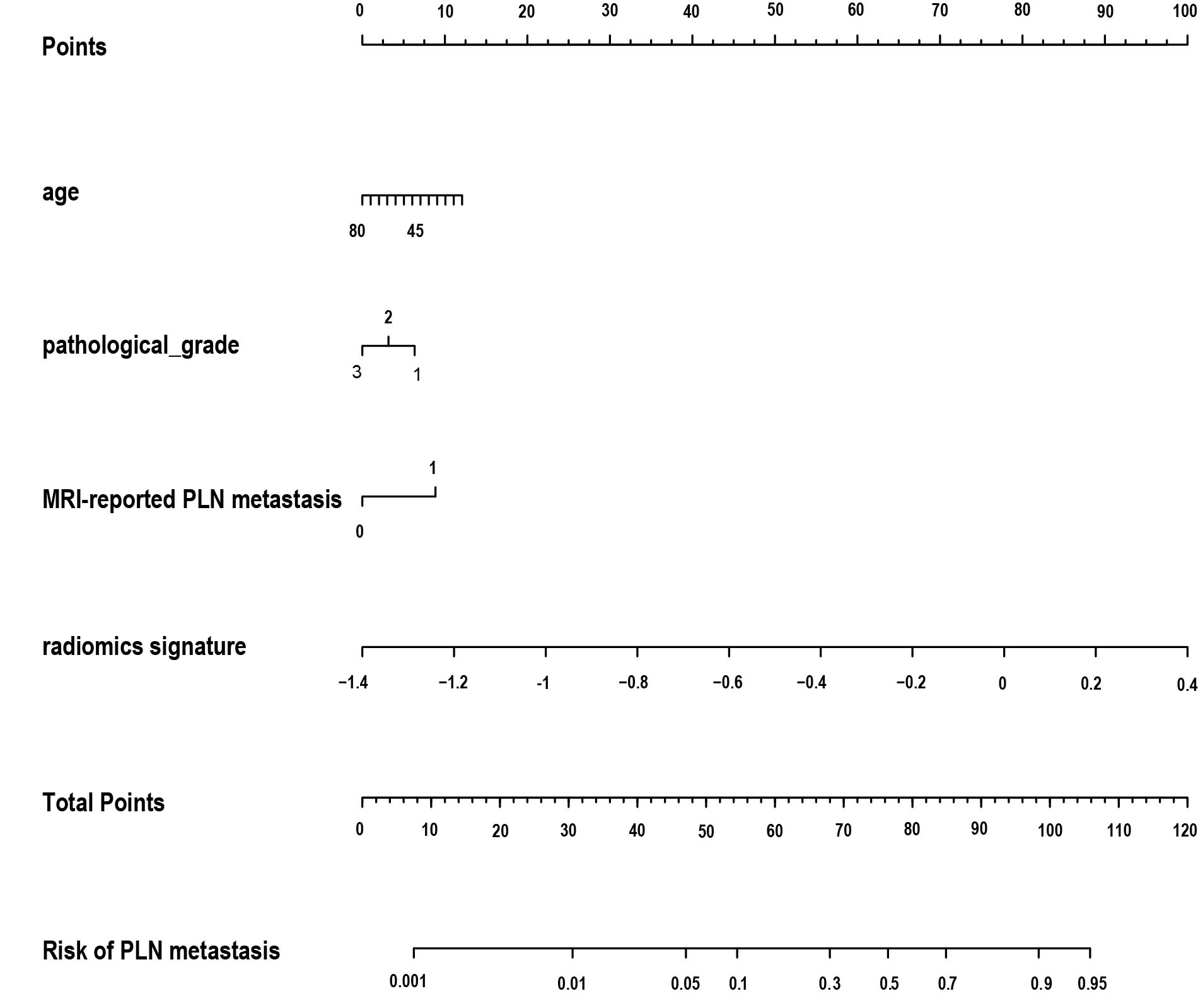
The radiomics nomogram integrated clinicopathological factors with the radiomics signature from joint T2WI and DWI.