4850
Automated Identification of Noise Signal in Spinal DCE-MRI using Independent Component Analysis and Unsupervised Machine Learning1Department of Biomedical Informatics and Medical Education, University of Washington, Seattle, WA, United States, 2Philips Healthcare, Gainsville, FL, United States, 3Radiology, University of Washington, Seattle, WA, United States, 4Radiation Oncology, University of Washington, Seattle, WA, United States
Synopsis
Dynamic Contrast-Enhanced (DCE) MR perfusion has shown early promise in evaluation of spinal metastatic disease and can improve prediction of treatment responses and post-treatment complications. However, spinal DCE-MRI exams frequently suffer from suboptimal image quality due to factors including cerebral spinal fluid (CSF) and vascular pulsation, respiration, bowel motion and patient bulk motion. Independent component analysis has been successfully used as a method to identify and remove motion artifacts from functional MR images. In this work, we combine ICA with an unsupervised machine learning method to automatically identify image components arising from contrast-enhancing tissues and those due to artifacts.
Introduction
Dynamic Contrast-Enhanced (DCE) MR perfusion has shown early promise in evaluation of spinal metastatic disease and can improve prediction of treatment responses and post-treatment complications. However, spinal DCE-MRI exams frequently suffer from suboptimal image quality due to factors including cerebral spinal fluid (CSF) and vascular pulsation, respiration, bowel motion and patient bulk motion. In this work, we combined an independent component analysis (ICA) technique [2] with an unsupervised machine learning strategy to automatically identify image components arising from contrast-enhancing tissues and those due to artifacts.5 Manual classification has often been used to label signal and noise components for supervised classification.5 We hypothesize that ICA components can be clustered in an unsupervised manner to identify signal and noise components, reducing the need for manually generating labeled training data.Methods
DCE-MRI Acquisition
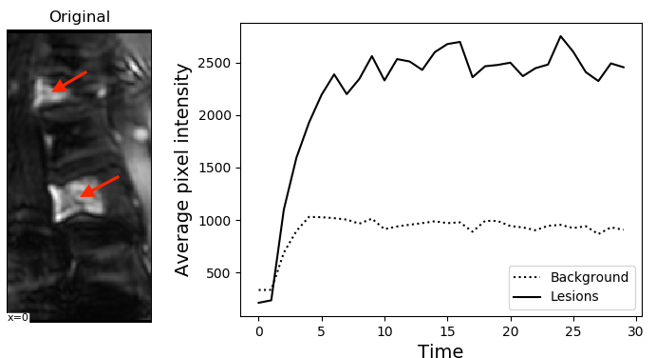
DCE-MRI was performed on a 3T Ingenia scanner (Philips Medical Systems, Best, the Netherlands) using a fat-suppressed 3D T1-weighted fast gradient echo readout (4D THRIVE) allowing a 6-s temporal resolution and 1.5 mm2 spatial resolution. An example anatomical DCE image (left), and the temporal signal enhancement of tumor (arrow) are shown in Figure 1.
ICA & Unsupervised Clustering
FastICA algorithm (convergence tolerance=0.001) is applied to each 4D DCE-MRI dataset extracting 30 independent component spatial maps sk and their associated temporal mixing weights ak(t). We use an unsupervised clustering algorithm to separate the resulting components into signal and artifact components. Each component is first mapped into feature space, and k-means clustering is used to compute clusters based on the Euclidean distance in feature space. Engineered features consist of signal statistical features derived from the temporal mixing weights ak(t).
K-means clustering with three target clusters is used to cluster the independent components. We initialize with three clusters to represent the three groups of components we expect to see: signal related to lesion enhancement, signal related to vascular enhancements, and noise due to motion artifacts. The enhancement profile of vasculature, like arteries and veins, is distinguishable from those of lesions, and are characterized by an immediate spike in voxel intensity.
Because an unsupervised model is used, no labels are provided for any of the the components. The outputs of the clustering algorithm are grouped by cluster and the clusters sorted by size. The two smaller clusters of components are labeled as the signal cluster.
Results
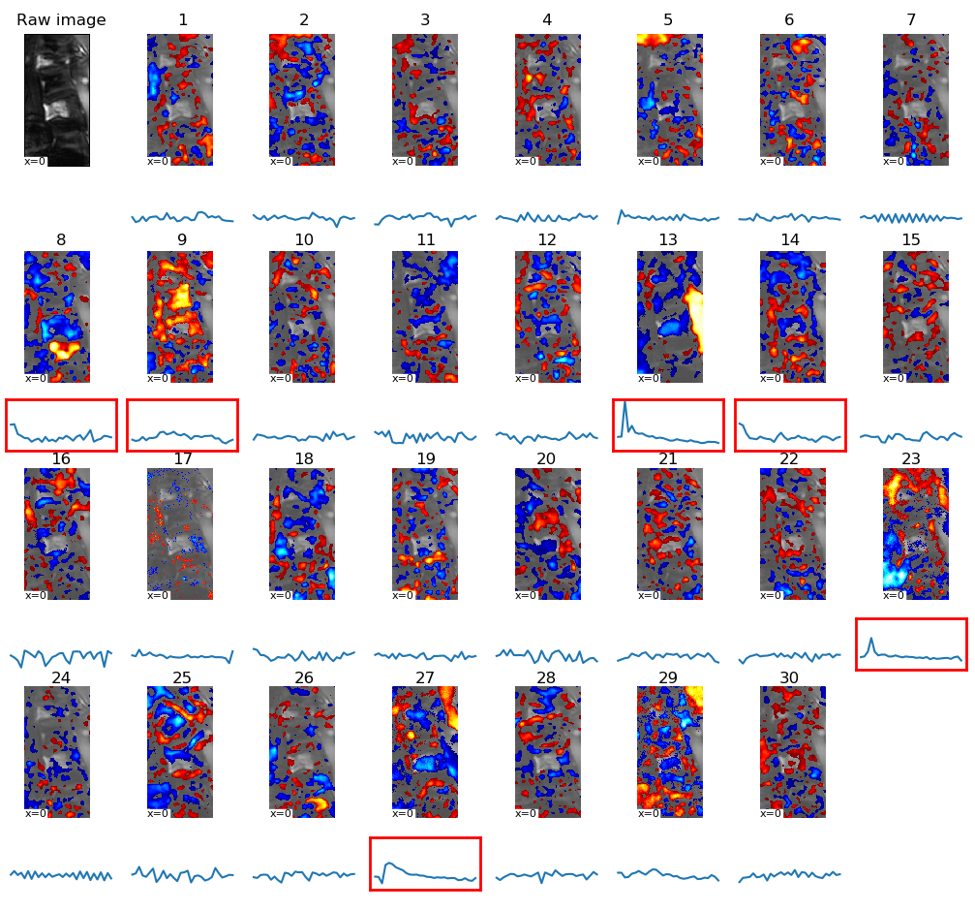
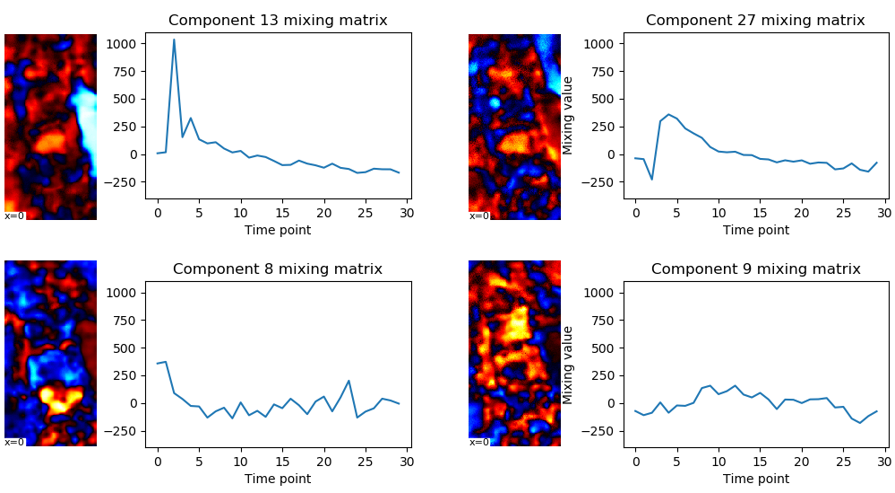
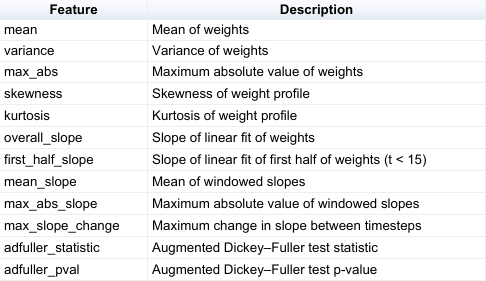
A full list of features and feature descriptions is given in Table 1. These features were computed over the ICA mixing weights. Many features are typical statistics of time series, such as mean, variance, skewness, kurtosis, etc, and some are features that attempt to measure trend in the time series, such as slope. The Augmented Dickey-Fuller test is a test of stationarity in time series, and is used as well. Figure 2 shows an example output of the ICA pipeline. A total of 30 components were extracted, and each component is displayed relative to the temporal mean of the raw image. Unsupervised clustering identified six components as signal components, more likely to correspond to vascular structures, such as lesions, vertebrae, or arteries and veins. Figure 3 shows several signal components and their temporal mixing values in greater detail.
Discussion
The mixing matrix of ICA components describes the importance of individual components over time, and can be used to identify spatial components corresponding to highly vascular tissues. We have demonstrated an unsupervised clustering technique based on manually engineered features that leverages these mixing matrices to cluster components into signal and noise groups. The signal components tend to correspond to vascular regions, such as lesions and vascular anatomy, and could be useful for automated identification of lesions in DCE spinal MR images. We have applied this technique to 15 patient images, and intend on expanding our analyses to 60 patients. Our hope is that an unsupervised approach can identify independent components with high fidelity without the need for generating expensive labeled training data.Conclusions
We have demonstrated the ability to use ICA for identifying high likelihood signal and noise components of DCE MR images. The unsupervised clustering algorithm using hand-engineered features is able to separate signal and noise components as demonstrated in our initial analysis. Further work is necessary to assess the validity of the identified signal components, and to apply this method at scale for denoising and automated lesion detection.Acknowledgements
This work was funded by Philips Healthcare.References
[1] V. Cuvinciuc, M. Viallon, I. Barnaure, M. I. Vargas, K. Lovblad and S. Haller. “Dynamic Contrast-Enhanced MR Perfusion of Intradural Spinal Lesions.” American journal of neuroradiology, 38(1): 192-194; 2017.
[2] A. Hyvärinen and E. Oja. “Independent component analysis: algorithms and applications.” Neural networks: the official journal of the International Neural Network Society, 13(4-5): 411-30; 2000.
[3] G. Salimi-Khorshidi, G. Douaud, C. F. Beckmann, M. F. Glasser, L. Griffanti and S. M. Smith. “Automatic denoising of functional MRI data: Combining independent component analysis and hierarchical fusion of classifiers.” NeuroImage, 90: 449-68; 2014.
[4] R. H. R. Pruim, M. Mennes, D. van Rooij, A. Llera, J. K. Buitelaar and C. F. Beckmann. “ICA-AROMA: A robust ICA-based strategy for removing motion artifacts from fMRI data.” NeuroImage, 112: 267-277; 2015.
[5] L. Griffanti, G. Douaud, J. D. Bijsterbosch, S. Evangelisti, F. Alfaro-Almagro, M. F. Glasser et al. “Hand classification of fMRI ICA noise components.” NeuroImage, 154: 188-205; 2017.
Figures