4842
A Realistic Numerical Simulation for Fetal Cardiac MRI1Radiology, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 2Medical Biophysics, University of Toronto, Toronto, ON, Canada, 3Translational Medicine, The Hospital for Sick Children, Toronto, ON, Canada, 4Pediatric Cardiology, The Hospital for Sick Children, Toronto, ON, Canada, 5Radiology, Duke University Medical Center, Durham, NC, United States, 6Pediatrics and Diagnostic Imaging, University of Toronto, Toronto, ON, Canada
Synopsis
Validating new techniques for fetal CMR is challenging due to random fetal movement that precludes repeat measurements. Consequently, fetal CMR development has been largely performed using physical phantoms or postnatal volunteers. In this work, we present an open-source simulation designed to aide in the development and validation of new approaches for fetal CMR. Our phantom: Fetal XCMR, builds on established methods for simulating MR acquisitions but is tailored toward the dynamic physiology of the fetal heart and body. We present comparisons between the Fetal XCMR phantom and data acquired in utero, resulting in image quality, anatomy, tissue signals and contrast.
Introduction
Assessing the fetal heart with cardiac magnetic resonance imaging (CMR) requires high-resolution acquisitions and reconstructions that are robust to motion. Studies have proposed accelerated imaging, motion compensation, and image-based gating to enable diagnostic fetal CMR [1–7]. Still, validating new techniques is challenging, as fetal movement precludes repeat measurements. Consequently, fetal CMR development has been largely performed using physical phantoms or postnatal volunteers. In this work, we present an open-source simulation designed to aide in the development and validation of new approaches for fetal CMR. Our approach – fetal extended Cardiac-Torso cardiac magnetic resonance imaging (Fetal XCMR) – builds on XCAT and MRXCAT, two previously established methods for simulating MR acquisitions, but is tailored toward the dynamic physiology of the fetal heart and body [8,9]. We present comparisons between the Fetal XCMR phantom and CMR data acquired in utero and highlight potential applications [3].Methods
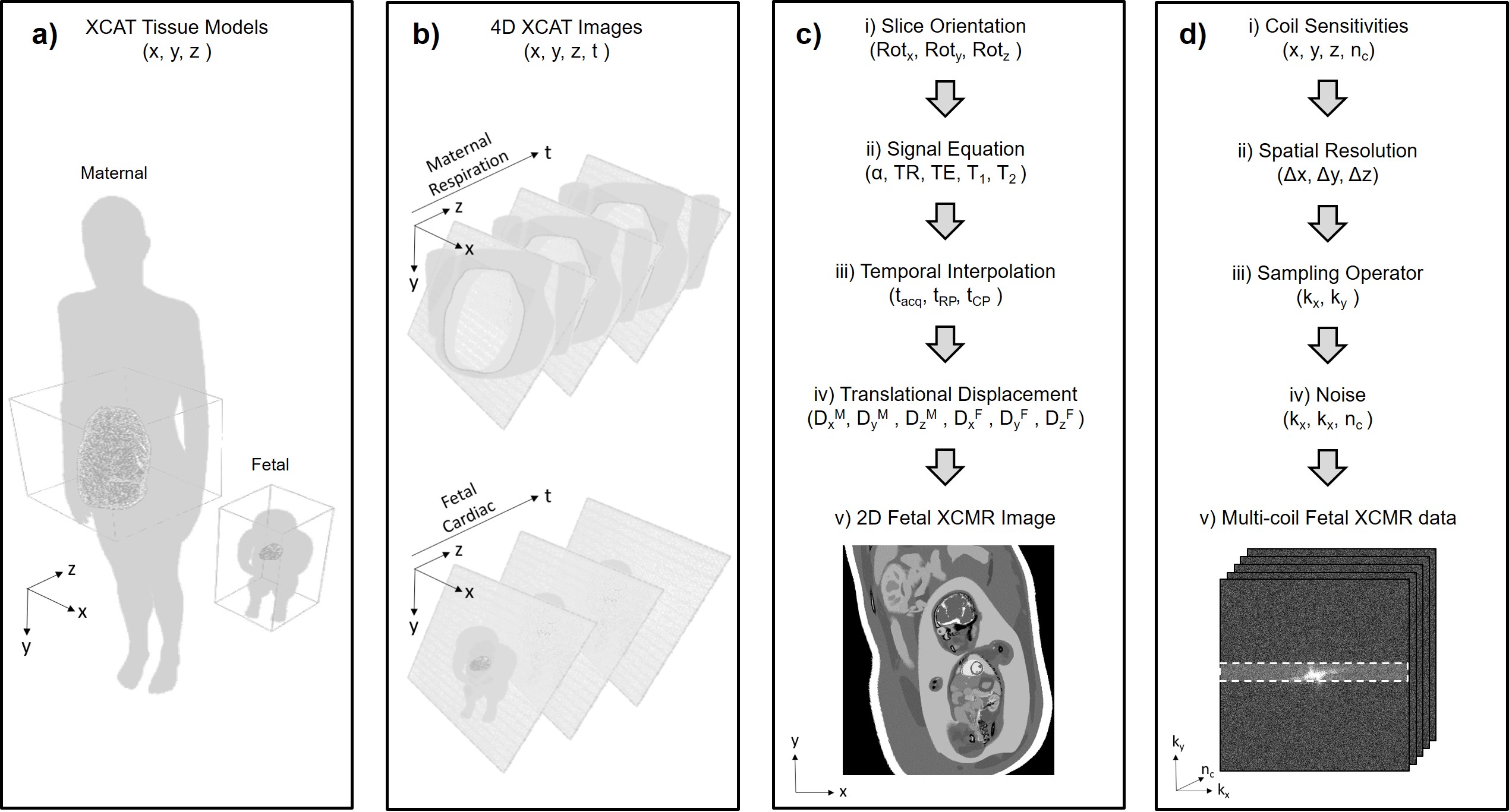
Fig. 1 provides an overview of the proposed workflow for simulating fetal CMR acquisitions. First, existing XCAT models are modified to create maternal and fetal anatomy (Fig. 1a). Second, 4D image arrays are generated from the modified XCAT models to form the basis of the phantom (Fig. 1b). Third, independent 4D XCAT arrays are combined and XCAT tissue values are mapped to MR contrast (Fig. 1c). Fourth, MR data is calculated from the image in the previous stage (Fig. 1d). Stages three and four are repeated to generate simulated k-space according to a user-selected sampling trajectory and reordering scheme. To provide a comparison between the proposed simulation and experimental fetal CMR images acquired in utero, images from a typical scan of a pregnant woman are included and simulated acquisitions were generated using matching MR parameters, motion and noise levels. A multi-slice 2D bssfp sequence with continuous golden angle radial sampling was prescribed in transverse, sagittal, coronal, and short-axis planes of the fetal heart on a 1.5T clinical MRI system (Avanto Fit, Siemens Healthineers – Germany). All scans were acquired free-breathing with the following CMR parameters: flip angle: 70°, acquired spokes: 1500, TR/TE: 4.95/2.41 ms, samples per spoke: 256, field-of-view: 256 × 256 mm2, spatial resolution: 1 × 1 × 4 mm3, acquisition length per slice: 7 seconds. For both simulated and in utero acquisitions, three reconstructions (static, real-time, and CINE) were performed in a manner described previously for golden angle radial fetal CMR data [3].Results
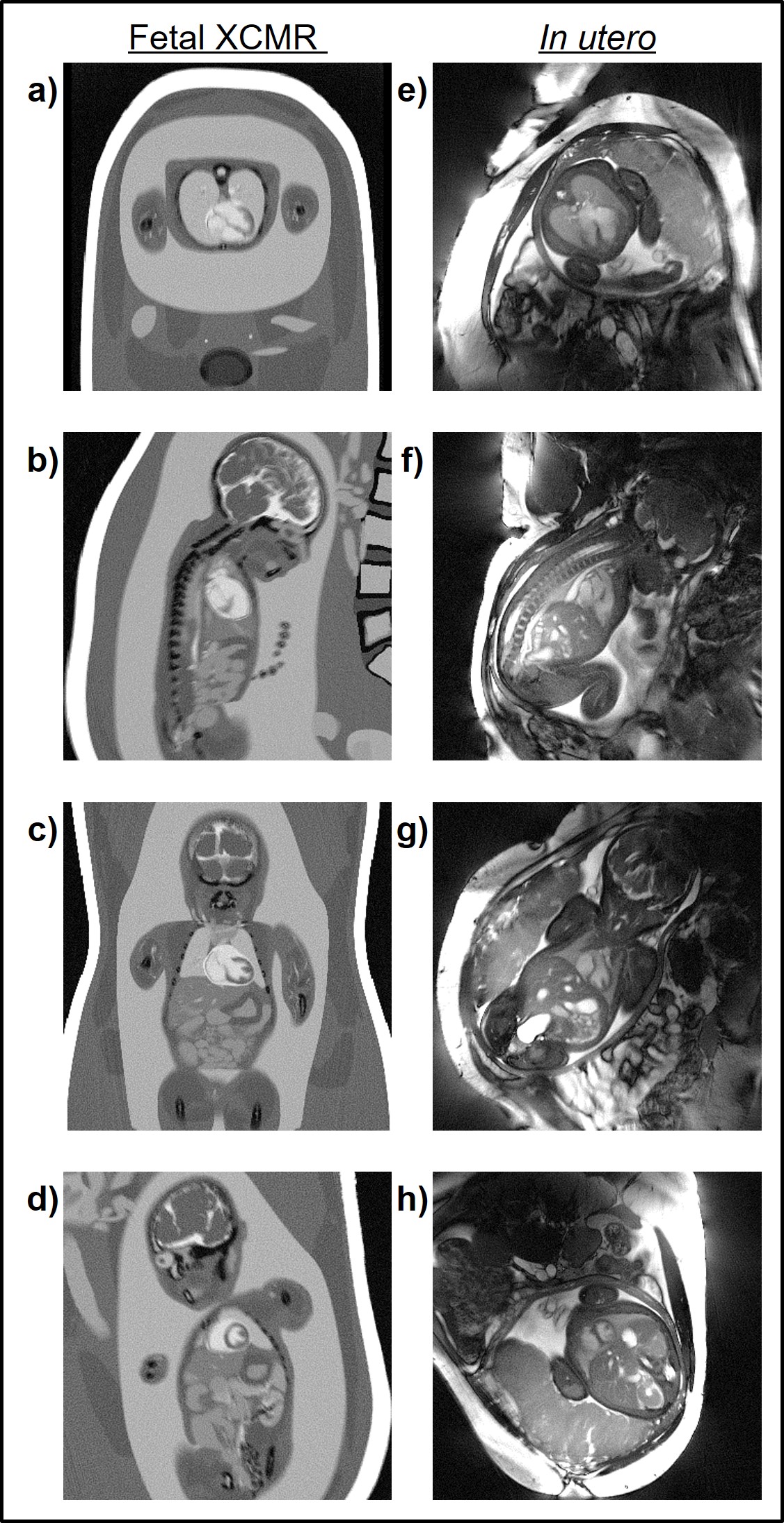
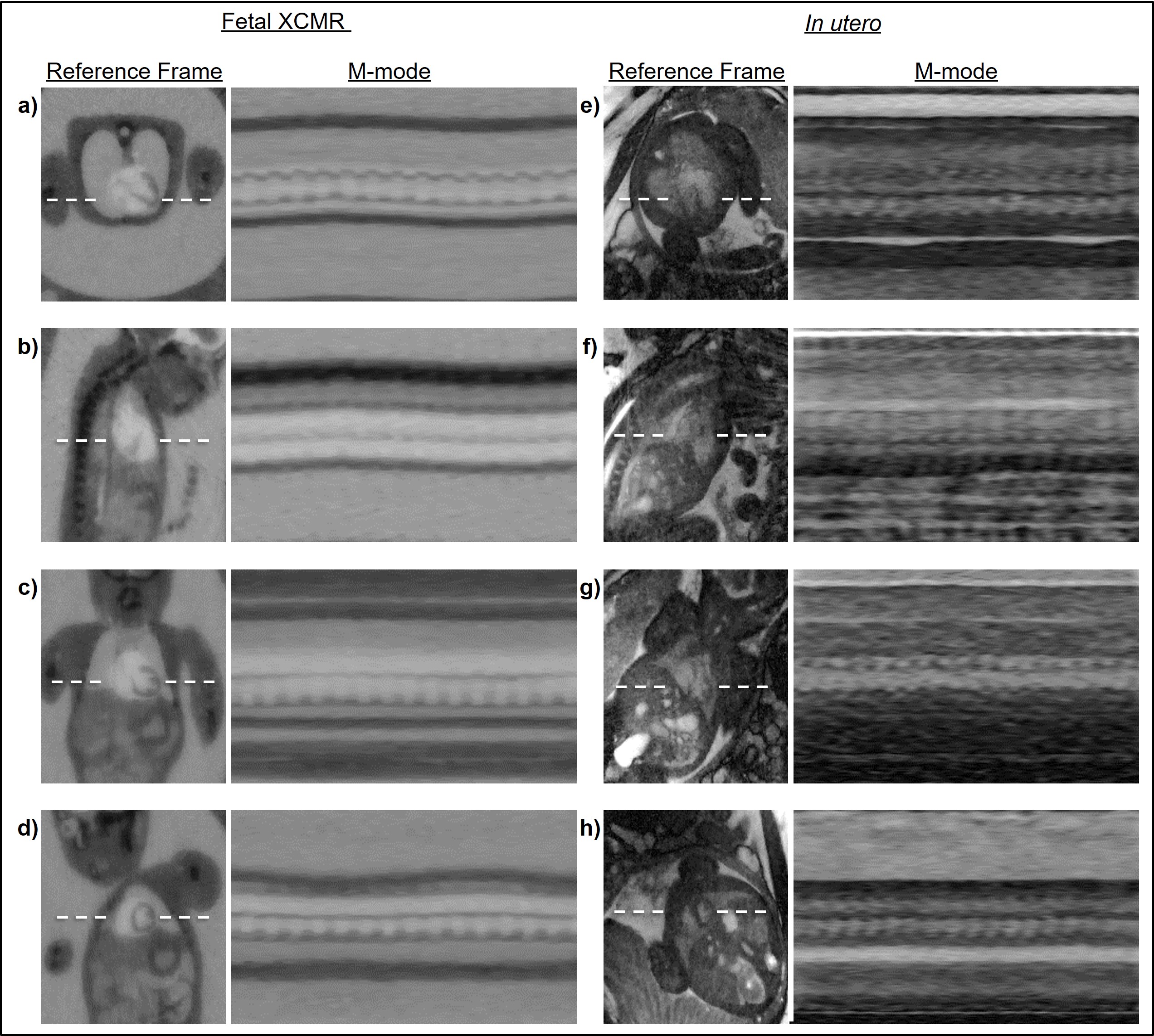
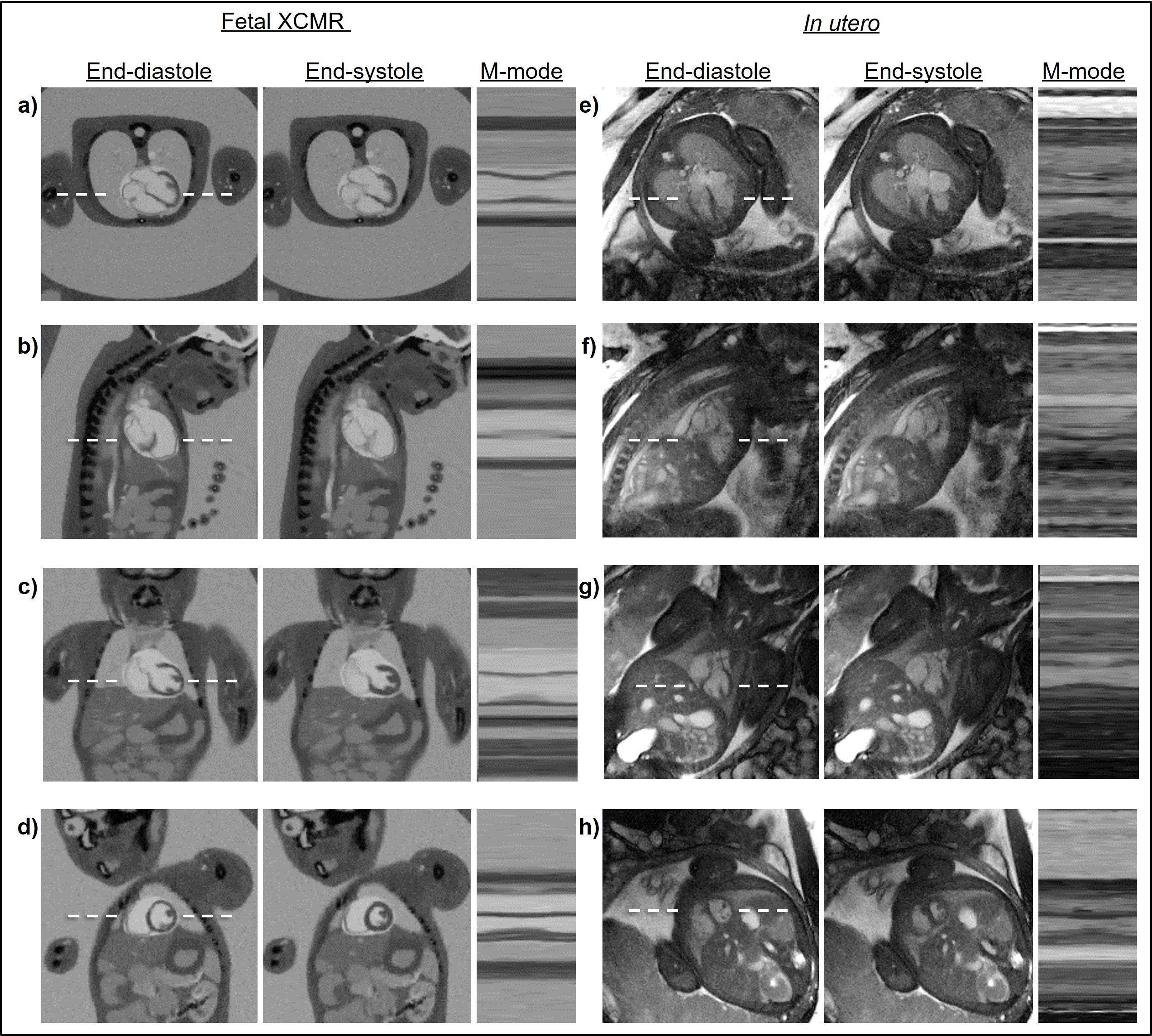
Fig. 2 displays representative static image reconstructions using the total number of acquired spokes from Fetal XCMR phantom and in utero fetal data sets. Overall, MR contrast, morphologies, and relative proportions of the maternal and fetal anatomy are well represented by the Fetal XCMR images in transverse (Fig. 2a), sagittal (Fig. 2b), coronal (Fig. 2c), and short-axis (Fig. 2d) orientations when compared to their in utero fetal image counterparts (Fig. 2e-h). Fig. 3 shows dynamic real-time image reconstructions of the same Fetal XCMR (Fig. 3a-d) and in utero fetal data (Fig. 3e-h) sets from Fig. 2. A still frame from the real-time image series is shown along with an M-mode representation of the temporal dynamics along the dash line. While the image quality is reduced, due to the level of undersampling, compressed sensing reconstruction allows for visualization of maternal respiratory and fetal cardiac motion. Finally, motion and heart rate estimates were derived from the real-time images (Fig. 3) and applied to each of the corresponding data sets to produce motion corrected CINE images of the fetal heart. Fig. 4 shows high quality CINE image reconstructions of Fetal XCMR data sets in transverse (Fig. 4a), sagittal (Fig. 4b), coronal (Fig. 4c), and short-axis (Fig. 4d) orientations with corresponding in utero images shown for comparison (Fig. 4e-h). For each data set, end-diastolic and end-systolic frames are shown along with an M-mode representation. Overall, the CINE images provide excellent delineation of fetal cardiac anatomy and temporal dynamics for both data types.Discussion
In this work, an open-source framework for simulating CMR images of the fetal heart was developed: Fetal XCMR. User-selected parameters control standard MRI acquisition parameters as well as the level of maternal respiratory motion and gross fetal movement. Comparison to in utero acquisitions yielded similar image quality, anatomy, tissue signals and contrast.Conclusions
The Fetal XCMR phantom provides a new method for evaluating fetal CMR acquisition and reconstruction methods by simulating the underlying anatomy and physiology. As the field of fetal CMR continues to grow, new methods will become available and require careful validation. The Fetal XCMR phantom is therefore a powerful and convenient tool in the continued development of fetal cardiac imaging.Acknowledgements
No acknowledgement found.References
1. Roy CW, Seed M, van Amerom JFP, et al. Dynamic imaging of the fetal heart using metric optimized gating. Magn Reson Med. 2013;70(6):1598–1607
2. Roy CW, Seed M, Macgowan CK. Accelerated MRI of the fetal heart using compressed sensing and metric optimized gating. Magn Reson Med. 2016;00:1–11
3. Roy CW, Seed M, Kingdom JC, Macgowan CK. Motion compensated cine CMR of the fetal heart using radial undersampling and compressed sensing. J Cardiovasc Magn Reson. 2017;19(1):29
4. van Amerom JFP, Lloyd DFA, Price AN, et al. Fetal cardiac cine imaging using highly accelerated dynamic MRI with retrospective motion correction and outlier rejection. Magn Reson Med. 2018;79(1):327–338
5. Chaptinel J, Yerly J, Mivelaz Y, et al. Fetal cardiac cine magnetic resonance imaging in utero. Sci Rep. 2017;7(1):15540
6. Haris K, Hedström E, Bidhult S, et al. Self-gated fetal cardiac MRI with tiny golden angle iGRASP: A feasibility study. J Magn Reson Imaging. 2017;1–11
7. Kording F, Yamamura J, de Sousa MT, et al. Dynamic fetal cardiovascular magnetic resonance imaging using Doppler ultrasound gating. J Cardiovasc Magn Reson. 2018;20(1):17
8. Segars WP, Sturgeon G, Mendonca S, Grimes J, Tsui BMW. 4D XCAT phantom for multimodality imaging research. Med Phys. 2010;37(9):4902
9. Wissmann L, Santelli C, Segars WP, Kozerke S. MRXCAT: Realistic numerical phantoms for cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2014;16(1):63
Figures