4816
MRI texture analysis for detection of axillary lymph node metastasis in breast cancer patients1Stony Brook University, Stony Brook, NY, United States
Synopsis
We tested the hypothesis whether texture analysis of axillary lymph node (aLN) MRI can reliably detect cancer metastasis in the aLN. Comparison was made with ground truth based on pathology and clinical reports. The top single-feature predictor yielded an area under the curve (AUC) of 0.91 and the top two-feature combination yielded an AUC of 0.95. These findings showed that texture analysis of aLN MRI can accurately predict disease status in the nodes associated with breast cancer.
Introduction
Axillary lymph nodes (aLNs) are critically important for staging breast cancer, designing treatment, and monitoring treatment response. Ultrasound, sentinel biopsy, and/or dissection to interrogate aLN are current standards of care for breast cancer patients but they have some drawbacks.
MRI detection of metastasis in aLNs is challenging due to the small aLN size, poor sensitivity of standard breast coil to axilla region and are often left out of the field of view. Small and subtle changes may not be clinically appreciable to the human eye. Texture analysis has the potential to detect subtle disease-relevant features in a quantitative manner.
Texture analysis of the lymph nodes in other cancers has been reported previously. In lung cancer, CT texture of mediastinal lymph nodes could detect differences between benign and malignant nodes with 53% sensitivity and 97% specificity [1]. In non-Hodgkin lymphoma, texture analysis of the apparent-diffusion-coefficient maps of lymph node could differentiate between benign and malignant lymph nodes with 79% sensitivity and 86% specificity [2]. Morphological feature (compactness) of aLNs for detection of metastasis has been found to have 83% sensitivity and 81% specificity [3]. However, texture analysis of the axillary lymph nodes in breast cancer has not been adequately studied. The goal of this study was to evaluate whether texture analysis of aLN MRI can reliably detect cancer metastasis in the aLN. Comparison was made with ground truths based on pathology and clinical reports.
Methods
Post contrast-enhanced MRI (1.5T) and PET/CT was used for analysis. Bilateral breast MR image was 3D fat-suppressed T1-weighted sequence with high resolution of 0.7x0.7x2mm acquired 1.5 minutes after contrast injection. Whole body 18F-FDG-PET/CT and their radiology reads were used for qualitative assessment of metabolic activity in each individual node. Disease nodes were those with high/moderate FDG-PET activity as read by radiologists. In total, 179 nodes from 41 patients were used in this analysis. Normal nodes were from contralateral side of unilateral breast cancer patients (122 nodes). aLN on MRI was manually segmented. Texture analysis was performed using LifeX 4.0 with 64 gray levels and image was normalized to ROI minimum and maximum. A linear model of texture features was created to predict whether there was disease in the aLN on the whole dataset, as well as on randomly assigned 80%/20% training/testing split. Post-analysis evaluation found that the training set consisted of 143 nodes (98 normal/45 diseased) and the testing set consisted of 36 nodes (24 normal/12 diseased). Standard receiver operating curve (ROC) analysis was performed to assess predictive performance, which include area under the curve (AUC), sensitivity, specificity, and accuracy.Results
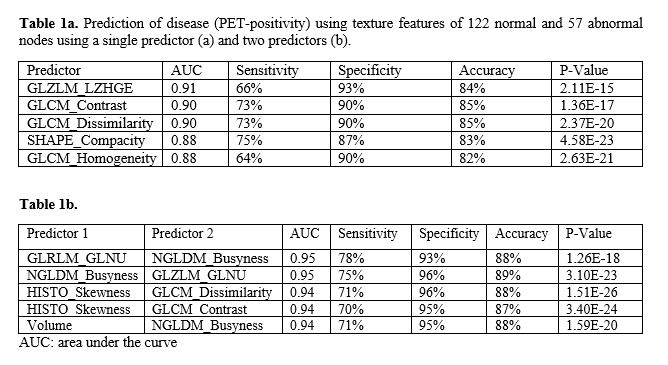
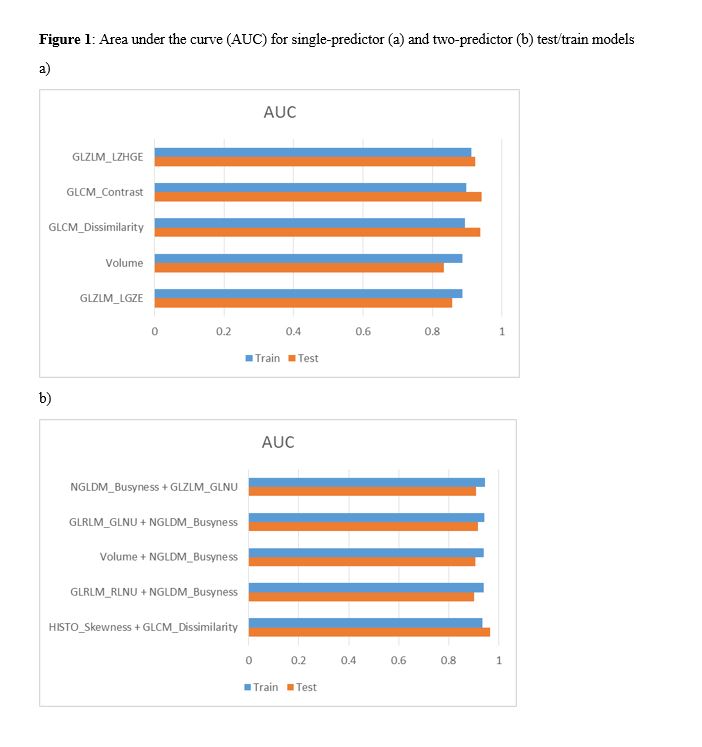
A total of 45 texture features were calculated for each lymph node. Table 1 shows ROC analysis using the entire dataset. The top three single-feature predictors as defined by the highest AUC were GLZLM_LZHGE, GLCM_Contrast, and GLCM_Dissimilarity, yielding an AUC of 0.91, 0.90 and 0.90, respectively. The top two-feature combinations were GLRLM_GLNU+NGLDM_Busyness, and NGLDM_Busyness+GLZLM_GLNU, yielding an AUC of 0.95 and 0.95, respectively. The sensitivity, specificity, accuracy and p values are also show in Table 1; they ranged from 70% to 96%. Specificity was generally higher than sensitivity. Figure 1 shows the results of the 80/20% split for training and testing, respectively. Top single-feature predictor was GLZLM_LZHGE, with an AUC of 0.91 (training) and 0.92 (testing). Top two-feature combination was GLRLM_GLNU+NGLDM_Busyness with an AUC of 0.94 (training) and 0.91 (testing).Discussion
AUCs of single and two-variable predictors were excellent. Specificity was generally higher than sensitivity, suggesting that texture analysis is more successful at predicting true-negatives than true-positives. Sentinel lymph node biopsies have a specificity (true negative) rate of 100% [4]. The specificity resulting from our analysis is ~90%. Development of imaging technology/analysis that can accurately identify absence of disease (high specificity) would be desirable because side effects associated with surgical procedures can be minimized.
A limitation of this study is there was no direct pathological validation of the same aLNs. Direct pathological validation is challenging because aLNs are small and clustered together. We used high FDG activity with reference to radiologist reports as ground truth for diseased nodes.
Conclusion
Texture analysis of aLN MRI can detect cancer metastasis in the aLN with reasonably high accuracy. The top single-feature predictor yielded an AUC of 0.91 and the top two-feature predictor combination yielded an AUC of 0.95. Future studies should improve MR image quality, spatial resolution, additional contrasts (i.e., diffusion-weighted MRI).Acknowledgements
No acknowledgement found.References
[1] Andersen MB et al. CT texture analysis can help differentiate between malignant and benign lymph nodes in the mediastinum in patients suspected for lung cancer. Acta Radiol. 2016 Jun;57(6):669-76. doi: 10.1177/0284185115598808. Epub 2015 Aug 12.
[2] De Paepe KN et al. Improving lymph node characterization in staging malignant lymphoma using first-order ADC texture analysis from whole-body diffusion-weighted MRI. J Magn Reson Imaging. 2018 Oct;48(4):897-906. doi: 10.1002/jmri.26034. Epub 2018 Apr 14.
[3] Fusco R et al. Use of Quantitative Morphological and Functional Features for Assessment of Axillary Lymph Node in Breast Dynamic Contrast-Enhanced Magnetic Resonance Imaging. Biomed Res Int. 2018 May 30;2018:2610801. doi: 10.1155/2018/2610801. eCollection 2018.
[4] Shiller SM et al. The sensitivity and specificity of sentinel lymph node biopsy for breast cancer at Baylor University Medical Center at Dallas: a retrospective review of 488 cases. Proc (Bayl Univ Med Cent). 2011 Apr;24(2):81-5.
Figures