4758
Sliding Window Reduced FOV Reconstruction in EPI for Real-Time Cardiac Imaging1Department of Internal Medicine II, University Ulm Medical Center, Ulm, Germany, 2Core Facility Small Animal Imaging (CF-SANI), Ulm University, Ulm, Germany
Synopsis
In this work we present a reconstruction technique based on $$$k$$$-space subtraction of static image parts to acquire real-time cardiac images. The static part is estimated with a sliding window reconstruction of the region outside of the heart to account for respiratory motion. The reduced field of view, i.e. the region of interest, is then reconstructed using a standard SENSE reconstruction, resulting in a temporal resolution of under 40 ms. The image quality is sufficient to estimate functional values in accordance with the BH-CINE reference standard.
Introduction
The region of interest (ROI) in cardiac imaging is limited to a small extent of the actual field of view (FOV). Simply reducing the FOV to save scan time and increase the temporal resolution is not possible as this would lead to severe image artifacts. While there were ideas to resolve this problem in Cartesian imaging in the 1990s by a subtraction technique1, the focus has recently shifted to saturation pulses2. However, these coincide with increased SAR values and reduce the probability of auxiliary findings. We propose the combination of a sliding window reduced FOV reconstruction (sw-rFOV) technique, EPI and standard Cartesian SENSE with moderate SENSE-factors to achieve real-time (RT) cardiac imaging with temporal resolution of under 40 ms.Methods
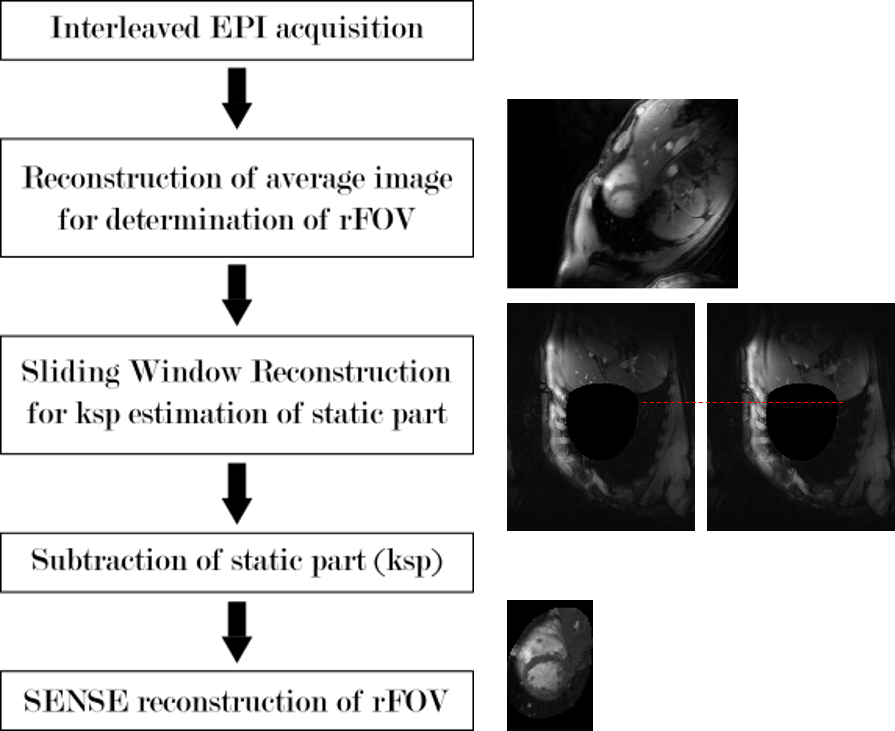
The reconstruction process is illustrated in figure 1 and described in the following. The sliding window width is set to five fully sampled images for the acquisitions, resulting in 720 ms temporal resolution.
The target $$$k$$$-space consists of $$$n$$$ EPI trains (equally spaced), the fully sampled $$$k$$$-space consists of $$$N$$$ trains. The acceleration factor $$$R$$$ is then calculated as
$$R=\frac{N}{n}.$$
The raw (full FOV) data is available in the same dimensions. $$$\textrm{ksp}_i$$$ denotes the full FOV $$$k$$$-space of the $$$i$$$-th frame ($$$i=1 … I$$$). The $$$j$$$-th ($$$j=1 … I/R$$$) fully sampled image is then
$$\textrm{img}_{\textrm{full},j}= \textrm{FT}\left[ \sum_{i=(j-1)R+1}^{jR} \textrm{ksp}_i \right].$$
The $$$k$$$-space of the static part of the image is created with the dynamic region set to 0 in image space:
$$\textrm{ksp}_{\textrm{static},j}=\textrm{FT}^{-1}\left[ \textrm{img}_{\textrm{full},j} (\textrm{dyn. reg.}=0) \right].$$
The sliding window of width $$$w$$$ ($$$w$$$ uneven, WLOG) is then calculated in $$$k$$$-space according to
$$\textrm{ksp}_{\textrm{sw},k}=\frac{1}{w}
\sum_{ind=k-\lfloor\frac{w}{2}\rfloor}^{k+\lfloor\frac{w}{2}\rfloor}
\textrm{ksp}_{\textrm{static},ind}$$
with $$$k=\lceil\frac{w}{2}\rceil ... J-\lfloor\frac{w}{2}\rfloor $$$ .
Finally, the rFOV $$$k$$$-space can be calculated as
$$\textrm{ksp}_{\textrm{dynamic},i} = \textrm{ksp}_i -\textrm{ksp}_{\textrm{sw},k}(\textrm{PE}_{\textrm{ksp}_i})$$
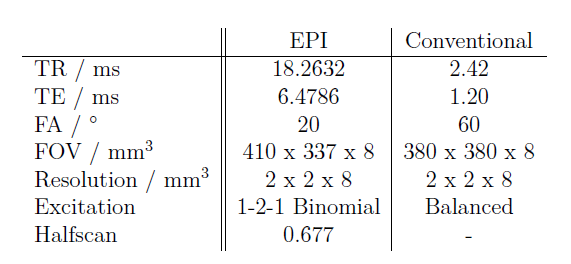
with $$$\textrm{PE}_{\textrm{ksp}_i}$$$ denoting the phase encode steps (non-zero $$$k$$$-space lines) of $$$\textrm{ksp}_i$$$, $$$i=R\lceil\frac{w}{2}\rceil ... I-R\lfloor\frac{w}{2}\rfloor$$$ and $$$k=\lfloor\frac{i}{R}\rfloor$$$. For further acceleration the rFOV reconstruction is based on standard Cartesian SENSE3. To reduce the influence of subcutaneous fat, the sequence was combined with a 1-2-1 binomial fat suppression pulse. The flip angle was chosen to maximize contrast between myocardium and the blood pool. Imaging is performed using an interleaved EPI sequence with the parameters given in table 1. All imaging experiments were performed on a 1.5 T clinical whole-body scanner (Philips Achieva, Best, The Netherlands) with a maximum gradient strength of 21 mT/m per channel and a maximum slew rate of 180 T/m/s. All data were acquired with a 32-element SENSE Cardiovascular array coil. The method was tested in three healthy volunteers, acquiring three short axis slices. Images are compared against standard SENSE reconstructed images from the same dataset and the BH-CINE images. Functional parameters of the left ventricle have been calculated with Segment (Medviso AB, Lund, Sweden).
Results
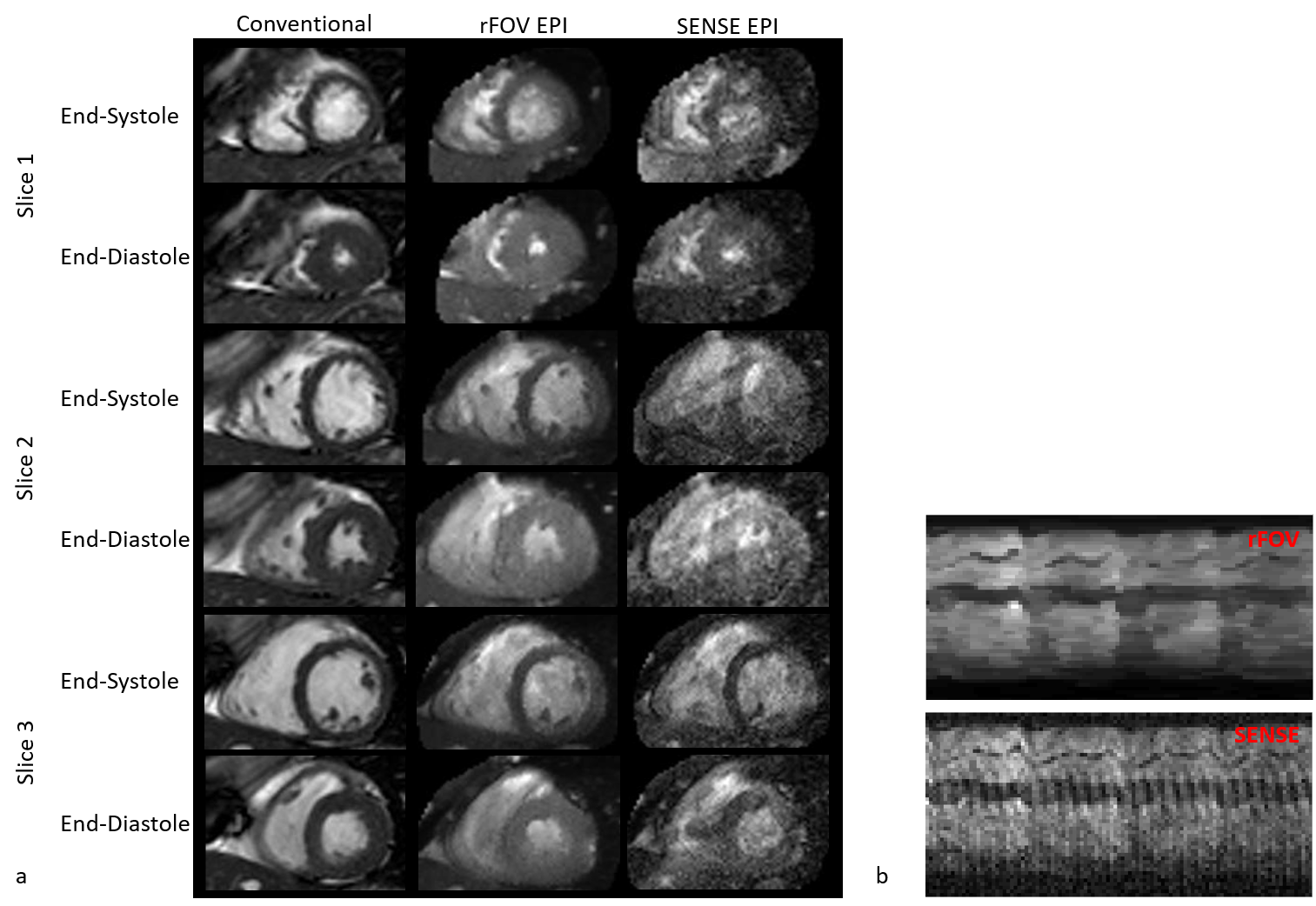
Figure 2 shows sw-rFOV
images, standard SENSE reconstructed images with the same temporal resolution and
the corresponding images from the breath-hold reference standard (a). Additionally,
m-mode images are shown for the non-gated reconstructions (b). Standard SENSE
reconstructed images show strong artifacts and appear not diagnostic. They are not
included in the further analysis.
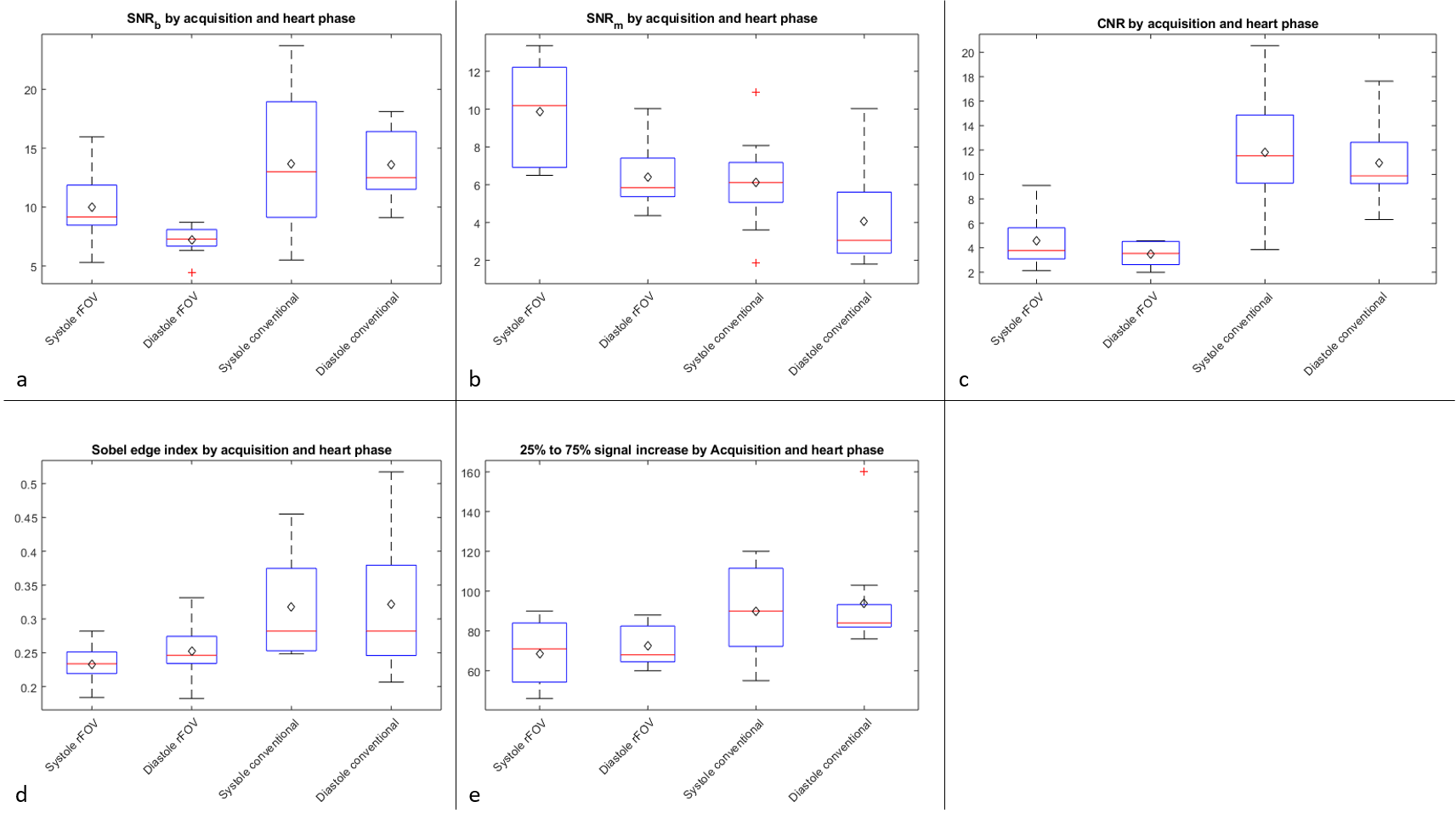
Quantitative image
quality measures and functional parameters are given in figure 3 and table 3,
respectively.Discussion
The ability of the sw-rFOV method to reconstruct RT cardiac images could be shown. Image quality is reduced and the contrast is degraded compared to BH-CINE acquisition. This can be partly explained by the superior b-SSFP contrast generation. However, it could be shown that the rFOV technique allows for higher undersampling factors and therefore higher temporal resolutions than a pure parallel imaging ansatz. Functional parameters are in line with the reference values, a Wilcoxon test showed no significant differences. It should be noted, that differences might be due to minor slice displacement between BH and RT imaging.
Compared to saturation pulse techniques sw-rFOV imaging holds two major advantages: lower SAR values and a higher probability of auxiliary findings. As opposed to other real-time imaging techniques, such as CS or Deep Learning, sw-rFOV relies on simple cartesian reconstruction and does neither need training data nor a carefully chosen regularization parameter and is very resource efficient in terms of reconstruction speed.
Conclusion
The sliding window reduced FOV reconstruction method combined with EPI is able to produce real-time cardiac images with good image quality. The sliding window based subtraction of the static part of the image leads to good results within the resulting reduced FOV. The use of other trajectories with favorable undersampling characteristics or higher sampling efficiency in combination with the sw-rFOV reconstruction techniqueis therefore a future topic of interest.Acknowledgements
The authors thank the Ulm University Centre for Translational Imaging MoMAN for its support.References
(1) Fredrickson, Jill O., and Norbert J. Pelc. "Temporal resolution improvement in dynamic imaging." Magnetic resonance in medicine 35.4 (1996): 621-625.
(2) Weingärtner, Sebastian, and Moeller, Steen and Akcakaya, Mehmet “Feasibility of Ultra-high Simultaneous Multi-slice and In-plane Accelerations for Cardiac MRI Using Outer Volume Suppression and Leakage-Blocking Reconstruction”, ISMRM 2018, 0359
(3) Pruessmann, Klaas P., et al. "SENSE: sensitivity encoding for fast MRI." Magnetic resonance in medicine 42.5 (1999): 952-962
Figures