4751
Cardiac and Respiratory Motion-Resolved 5D Imaging Using a Free-Running Framework: Comparison of Cartesian and Radial Trajectories1Radiology, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 2Center for Biomedical Imaging (CIBM), Lausanne, Switzerland, 3Siemens Healthcare GmbH, Erlangen, Germany, 4Advanced Clinical Imaging Technology (ACIT), Siemens Healthcare AG, Lausanne, Switzerland, 5LTS5, École Polytechnique Fédérale de Lausanne (EPFL), Lausanne, Switzerland
Synopsis
Recent advances have enabled high resolution cardiac imaging using continuous acquisitions that do not require external gating devices and can be reconstructed in arbitrary dimensions. Here, we extend the use of this Free-running framework to a fully self-gated free-breathing 3D Cartesian trajectory with spiral profile ordering for cardiac and respiratory motion resolved 5D imaging. We demonstrate the feasibility of this Cartesian approach by reconstructing and comparing images from both radial and Cartesian sequences with matching scan parameters in healthy volunteers. Overall, Cartesian images demonstrated comparable cardiac and respiratory motion albeit with more residual artifacts present in the Cartesian images.
Introduction
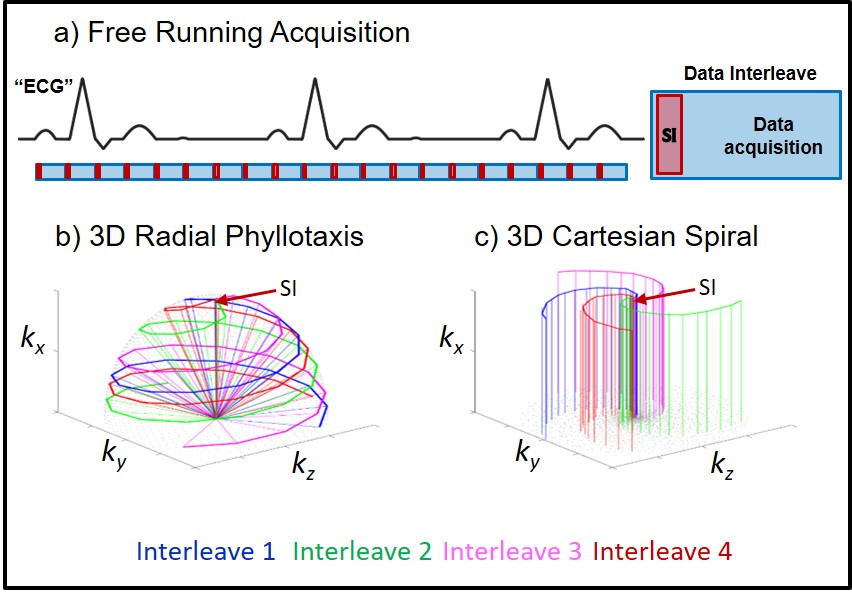
Whole-heart MRI requires acquisitions and reconstructions that are robust to cardiac and respiratory motion. In conventional examinations, a combination of ECG-gating and breath-holding or respiratory navigation is used to freeze physiological motion and produce sharp images. However, external gating devices add to patient setup time, and respiratory control can be difficult in some patients. Recent advances have enabled high-resolution imaging using continuous radial phyllotaxis acquisitions that do not require external devices and can be reconstructed exploiting the intrinsic similarities of arbitrary dimensions (Free-running framework) [1-6]. This is accomplished using a repeated readout along the superior-inferior (SI) direction for retrospective extraction of respiratory and cardiac signals, which informs the compressed sensing reconstruction to suppress undersampling artifact. In this work, we investigate the feasibility of applying the Free-running framework to a Cartesian trajectory with spiral profile reordering for cardiac and respiratory resolved 5D imaging [7-9]. Cartesian sampling is a potentially useful alternative to radial as it is less sensitive to trajectory errors, the imaging volume can more easily be tailored to specific applications allowing for a trade-off between scan time, contrast, and resolution, and the reconstruction can be performed without computationally demanding re-gridding. We demonstrate the feasibility of Free-running Cartesian 5D imaging in healthy volunteers and both qualitatively and quantitatively compare image reconstructions of radial and Cartesian acquisitions.Methods
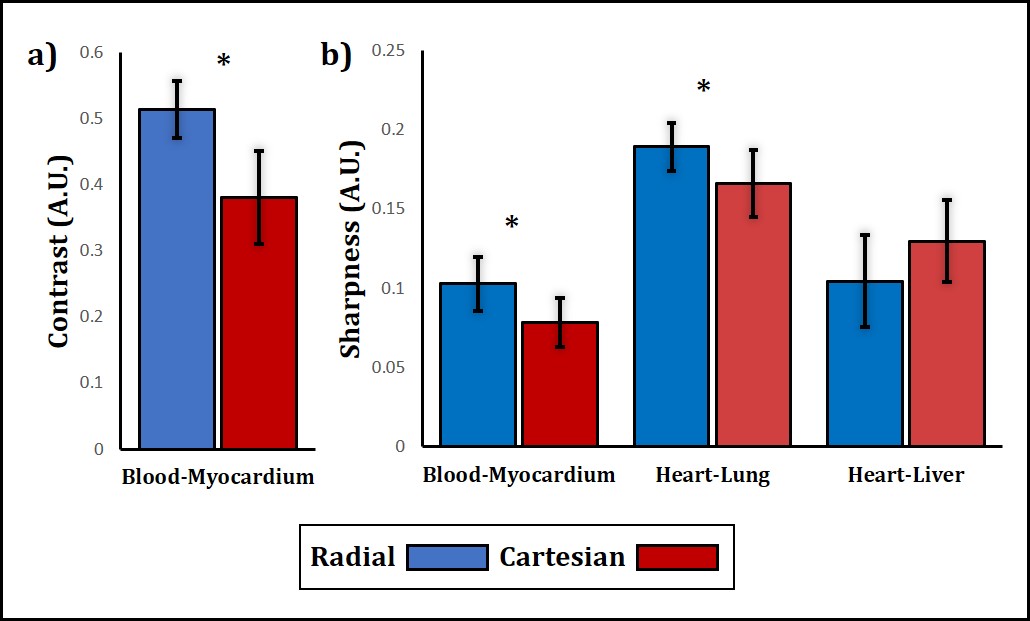
Data were acquired in 8 healthy volunteers (5 male, ages 26-33 years) on a 1.5T clinical MRI scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). Two prototype slab-selective 3D bSSFP sequences with radial (Fig. 1b) and Cartesian (Fib. 1c) sampling were acquired using golden angle phyllotaxis [6] and spiral profile reordering [8], respectively. To match the self-navigation and flexible binning of the radial acquisition, the Cartesian sequence was modified to acquire data independent of the ECG, and one readout oriented along the SI direction was repeated per interleave for subsequent extraction of physiological signals. All imaging parameters, listed in Fig. 1, were consistent between the two sequences except for the field-of-view which was isotropic (220 mm3) for the radial sequence and rectangular for Cartesian (220 x 380 x 165 mm3). Additionally, the RF excitation angle was lowered in some volunteers due to SAR limitations. Data was retrospectively sorted into 16-25 cardiac phases of 50ms window-width and 4 respiratory motion states [3]. The resulting 5D datasets were reconstructed offline using a k-t SPARSE SENSE algorithm with regularization along both temporal dimensions [1, 3]. Qualitative comparison of images was performed by visual inspection across all reconstructed slices and temporal dimensions. Quantitative comparison of contrasts measurements was performed using the ratio of manually selected regions of interest containing the blood pool and myocardium. Measurements of image sharpness were performed using the signal gradient along the blood-myocardium, heart-lung, and heart-liver boundaries [10]. All measurements were taken during end-systole at end-expiration and statistical analysis was performed using paired t-tests.Results
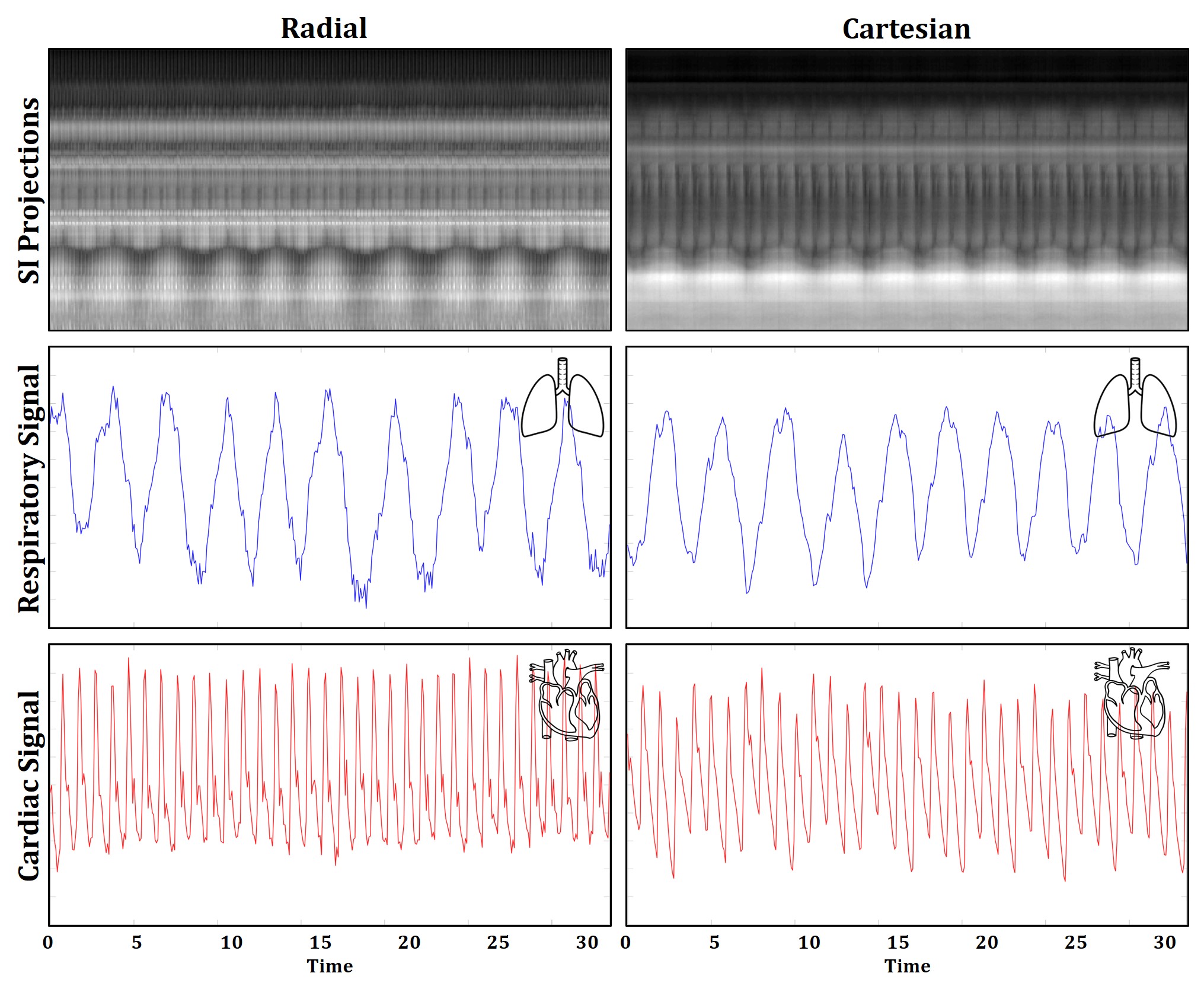
Cardiac and respiratory signals were successfully extracted (Fig. 2) from all 8 volunteers and used for reconstructions of radial and Cartesian acquisitions. In general, Cartesian reconstructions took less time (3-5 hours) using a CPU Fourier transform than their radial counterparts (5-8 hours) which used a GPU non-uniform Fourier Transform. Figs. 3 and 4 show two example reconstructions. Visual comparison of radial and Cartesian images shows that dynamic cardiac and respiratory motion is correctly resolved. However, Cartesian images contain noticeably more residual artifact, leading to an apparent decrease in contrast between the myocardium and blood pool, which was confirmed to be statistically higher (p<0.05) for radial images (Fig. 5a). Quantitative comparison of sharpness also yielded statistically higher (p<0.05) measurements along the blood-myocardium and heart-lung boundaries for radial images, but there was no significant difference in sharpness at the heart-liver boundary.Discussion and Conclusions
5D imaging using a Free-running framework is a promising technique for easily assessing the structure and function of the whole-heart in one single scan. It can be performed without ECG during free-breathing and without extensive image planning relative to the standard clinical 2D CINE approach. Here, we show that Cartesian sampling may be used as an alternative to radial phyllotaxis sampling within the Free-running framework. This study is to our knowledge, the first comparison of 5D imaging between radial and Cartesian acquisitions. To provide a baseline comparison, acquisition and reconstruction parameters were nearly identical. Overall the Cartesian sequence produced similar images to the radial sequence. Still, additional optimization of the Cartesian approach is required to improve image quality. In particular, the use of ESPIRiT for coil sensitivities may help reduce residual fold-over artifacts in the Cartesian 5D images [11].Acknowledgements
No acknowledgement found.References
[1] S. Coppo, D. Piccini, G. Bonanno, J. Chaptinel, G. Vincenti, H. Feliciano, R.B. van Heeswijk, J. Schwitter, M. Stuber. Free-Running 4D Whole-Heart Self-Navigated Golden Angle MRI: Initial Results. Magn. Reson. Med. 2015; 74:1306–1316.
[2] L. Feng, L. Axel, H. Chandarana, K. T. Block, D. K. Sodickson, and R. Otazo, “XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing,” Magn. Reson. Med. 2016; 75:775–788
[3] L. Feng, S. Coppo, D. Piccini, J. Yerly, R.P. Lim, P.G. Masci, M. Stuber, D.K. Sodickson, R. Otazo. 5D whole-heart sparse MRI. Magn. Reson. Med. 2018; 79:826–838
[4] J. Yerly, D. Piccini, L. Di Sopra, J. AM Bastiannsen, S. Coppo, and M. Stuber “Improved Time Efficiency and Workflow for Fully Self-Gated Non-Contrast 5D Imaging of the Heart,” in Proc. Intl. Soc. Mag. Reson. Med. 2017, 2874
[5] L. Di Sopra, D. Piccini, S. Coppo, J. A.M. Bastiaansen, M. Stuber, and J. Yerly, “Motion-resolved 5d imaging of the heart: time to get rid of the ECG?,” in Proc. Intl. Soc. Mag. Reson. Med. 2017, 3148
[6] D. Piccini, A. Littmann, S. Nielles-Vallespin, and M. O. Zenge, “Spiral phyllotaxis: the natural way to construct a 3D radial trajectory in MRI.,” Magn. Reson. Med. 2011; 66: 1049–56
[7] C. Forman, D. Piccini, R. Grimm, J. Hutter, J. Hornegger, and M. O. Zenge, “High-resolution 3D whole-heart coronary MRA: a study on the combination of data acquisition in multiple breath-holds and 1D residual respiratory motion compensation,” Magn. Reson. Mater. Physics, Biol. Med. 2014 27; 435–443
[8] J. Wetzl, F. Lugauer, M. Schmidt, A. Maier, J. Hornegger, and C. Forman, “Free-Breathing, Self-Navigated Isotropic 3-D CINE Imaging of the Whole Heart Using Cartesian Sampling,” Proc. Intl. Soc. Mag. Reson. Med. 2016, 411
[9] T. Correia, G. Ginami, G. Cruz, R. Neji, R. Rashid, R.M. Botnar, C. Prieto. Optimized respiratory-resolved motion-compensated 3D Cartesian coronary MR angiography. Magn Reson Med. 2018;80(6):2618–2629
[10] R. Ahmad, Y. Ding, O.P. Simonetti. Edge sharpness assessment by parametric modeling: Application to magnetic resonance imaging. Concepts in Magnetic Resonance. 2015; 44:138–149.
[11] M. Uecker et al., “ESPIRiT--an eigenvalue approach to autocalibrating parallel MRI: where SENSE meets GRAPPA.,” Magn. Reson. Med. 2014; 71:990–1001
Figures