4750
Rapid, Free-Breathing, Cine MRI for Patients with a Cardiac Implantable Electronic Device: A Preliminary Study1Radiology, Northwestern University Feinberg School of Medicine, Chicago, IL, United States, 2Radiology, Mayo Clinic, Rochester, MN, United States, 3Cardiology, Internal Medicine, Northwestern University Feinberg School of Medicine, Chicago, IL, United States, 4Biomedical Engineering, Northwestern University, Evanston, IL, United States
Synopsis
Standard ECG-gated, breath-held cardiac cine MRI often produces poor image quality in patients with a cardiac implantable electronic device (CIED) due to off-resonance effects, high prevalence of arrhythmia, and/or difficulty in breath-holding. This study seeks to develop a 16-fold accelerated, free-breathing cine MRI pulse sequence using a combination of a gradient echo readout, compressed sensing, and optimal Cartesian k-space sampling. The results from this study shows that an optimal k-space sampling scheme produces superior results compared to random and Poisson disc k-space sampling patterns in imaging phantoms and patients.
Introduction
ECG-gated, breath-held cardiac cine MRI with a balanced steady state free-precession (b-SSFP) readout is considered the reference test for evaluation of cardiac function in non-device patients1,2. In patients with a cardiac implantable electronic device (CIED), however, bSSFP cine often produces non-diagnostic image quality due to severe image artifacts arising from the device, arrhythmia and/or difficulty in breath-holding. One approach to overcome these limitations is to develop a rapid free-breathing cine MRI pulse sequence, but this task is challenging because the presence of a CIED precludes the use of b-SSFP readout and non-Cartesian k-space sampling patterns. In response to this unmet need, we propose to develop a rapid, free-breathing, cine MRI pulse sequence using a combination of gradient echo readout, compressed sensing (CS)3, and optimal 16-fold accelerated Cartesian k-space sampling and evaluate its performance in phantom and patients with and without a CIED.Methods
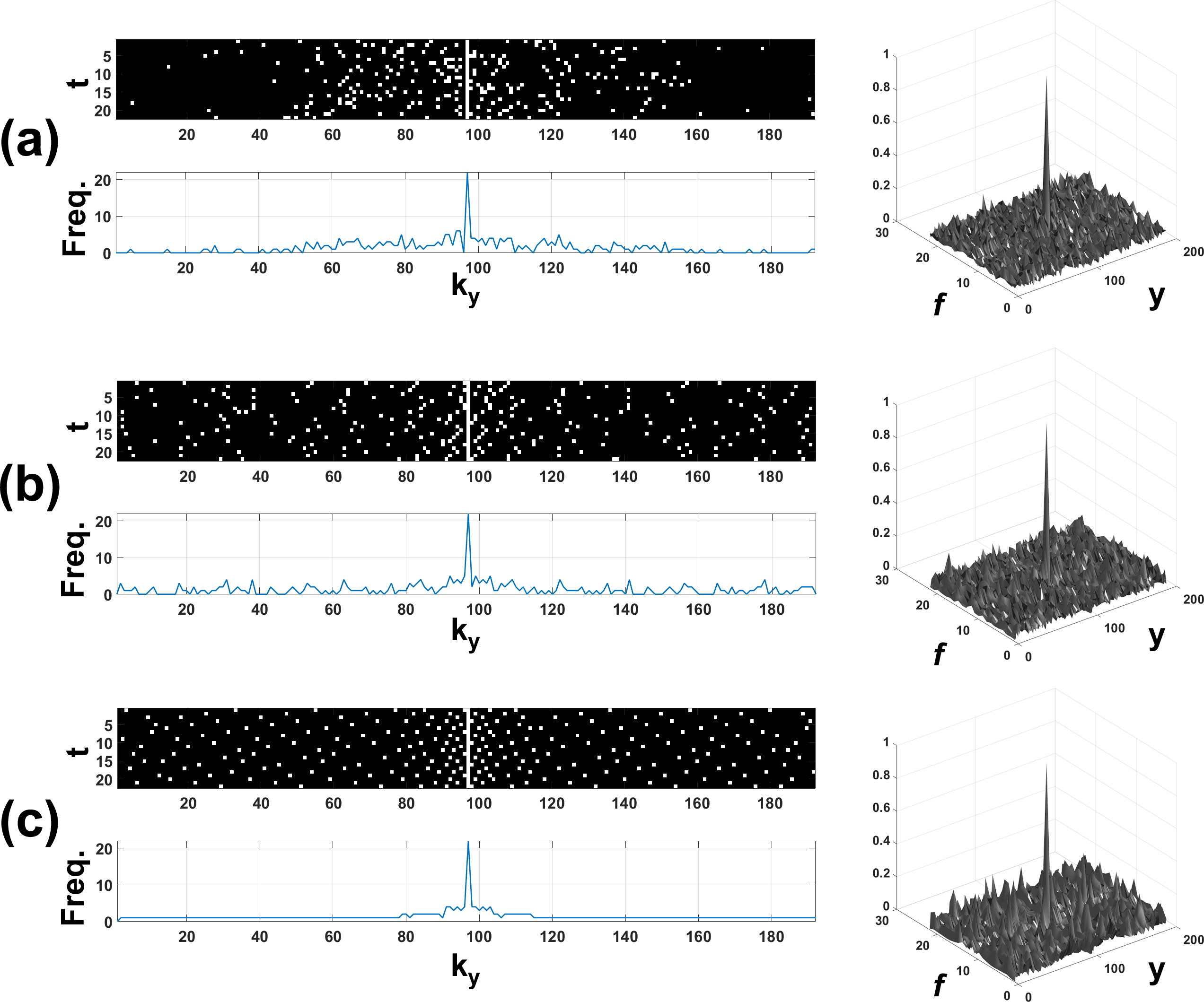
Pulse Sequence: We implemented three different versions of 16-fold accelerated cine MRI pulse sequences which used, except for the undersampling mask, the following identical imaging parameters: FOV = 400 x 400 mm2, slice thickness = 8 mm, matrix size = 192 x 192, TE/TR = 1.8/3.76 msec, flip angle = 20°, receiver bandwidth = 744 Hz/pix, 1 dummy heartbeat to approach steady state, 22 cardiac frames, 12 k-space lines per image/frame, temporal resolution = 45.1 msec, flow compensated gradients along slice and readout directions, asymmetric readout (0.68). ky-t Sampling Patterns: As shown in Figure 1, we tested three undersampled ky-t masks acquiring 12 ky lines (R=16) per frame: random with variable density4, Poisson disc5 with variable density, and lattice-like6 with variable density. For each sampling pattern, the center of k-space was always sampled to ensure the zero-filled data represent a reasonable starting point for CS reconstruction. The proposed lattice-like sampling pattern was designed to ensure that all ky lines are sampled at least once over 22 cardiac frames. For each k-space sampling pattern, we examined its point spread function (PSF) and sparsity in the temporal principal component analysis (PCA) domain. The incoherence of PSF was calculated from three k-space sampling patterns. MRI Experiments: We tested the performance of cine scans on an ACR phantom and two male non-device patients (age = 71 and 65 years) and one female CIED patient (59 years) at 1.5T (AERA and AVANTO, Siemens). Cine scans were performed after administration of clinical dose (0.15 to 0.2 mmol/kg) of gadobutrol (Gadavist, Bayer). All patients provided written informed consent approved by our institutional review board. Image Reconstruction: For each k-space sampling pattern, we performed CS reconstruction using temporal total variation and PCA as two orthogonal sparsifying transforms with identical normalized regularization weights of 0.01 and 50 iterations. The weights were determined empirically based on visual analysis of training data.Results
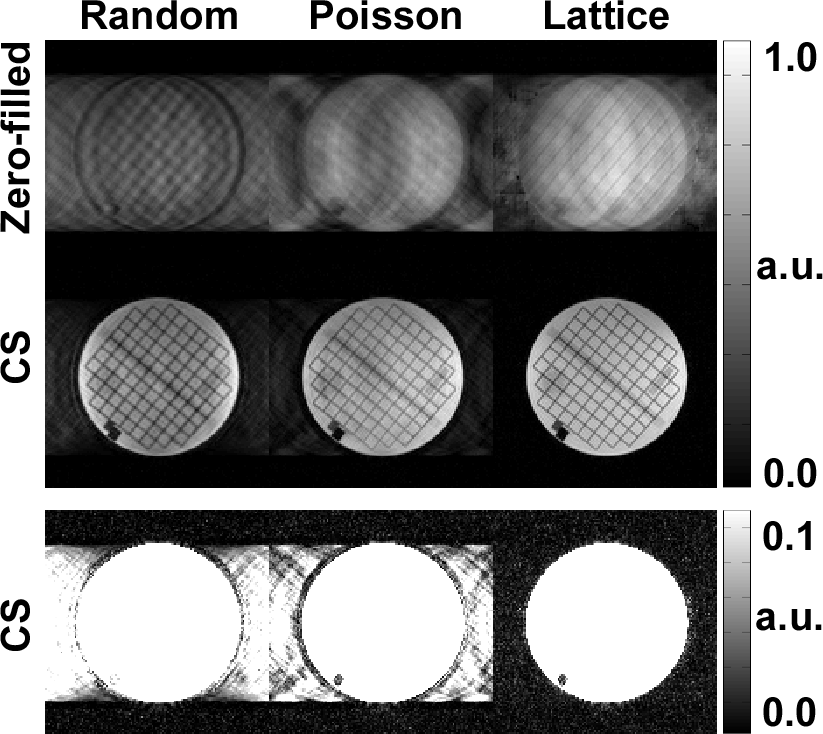
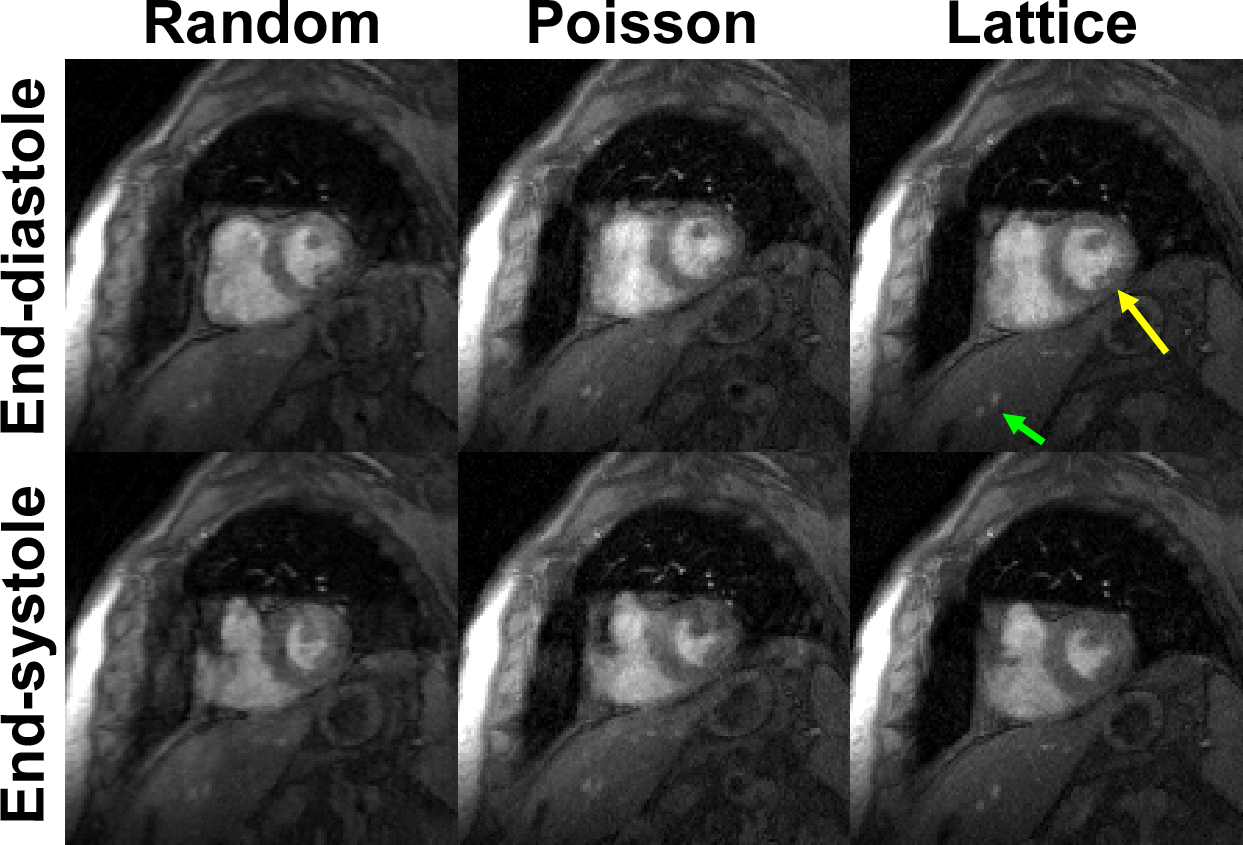
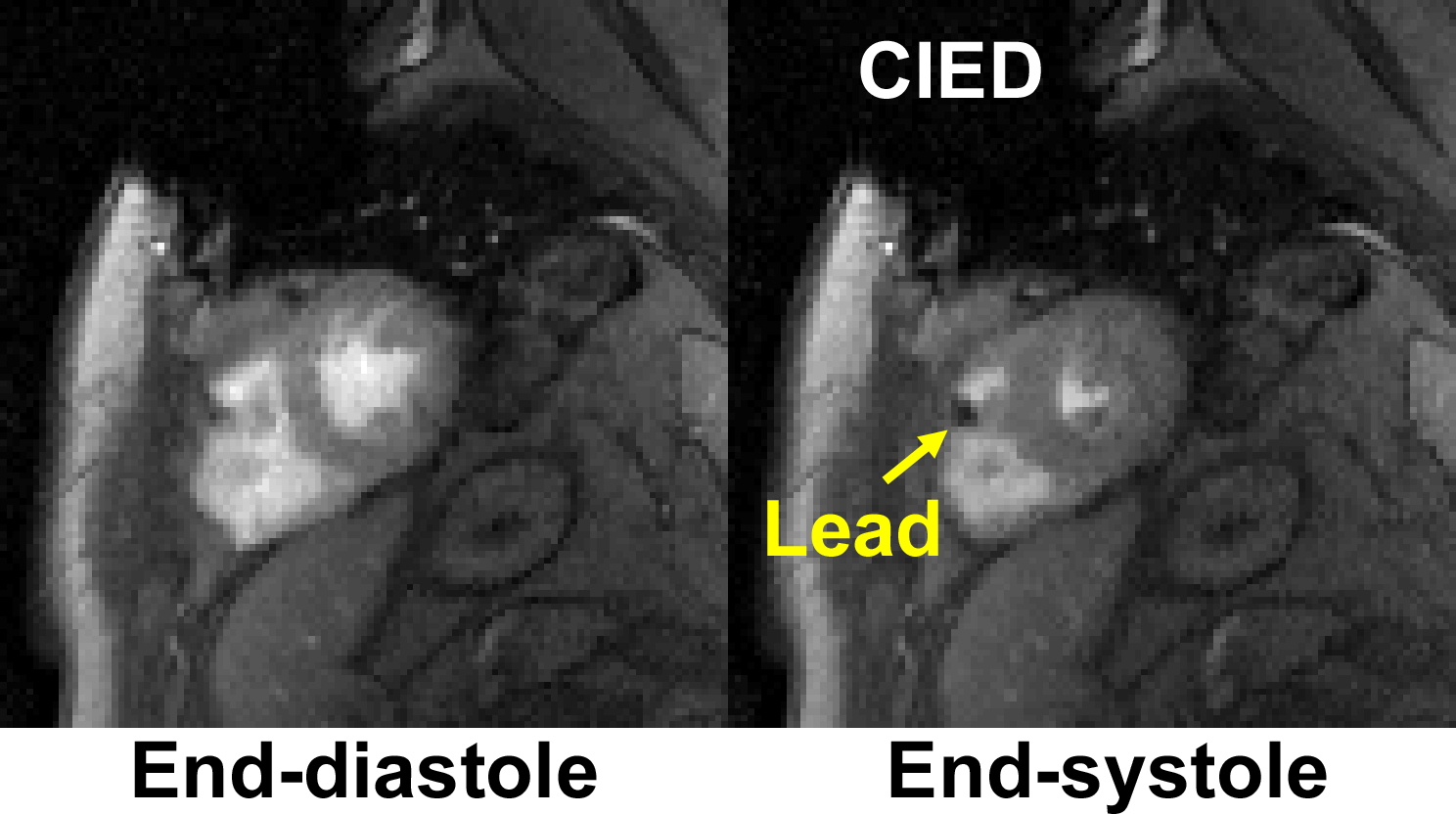
While the incoherence of PSF for lattice (27.3) was lower than that for random (33.1) and Poisson disc (32.1), the lattice produced aliasing artifacts that are more sparse than random and Poisson disc (see Figure 2). Figure 3 compares results between the three k-space sampling patterns, where the lattice pattern produced sharper images (see grid lines on the ACR phantom) with fewer residual artifacts in the background. Figure 4 compares the results in a non-device patient, where the lattice produced shaper images with fewer artifacts than the other two sampling patterns. Figure 5 shows results obtained with a lattice-like pattern in a CIED patient, illustrating good image quality that are consistent with the non-device patient shown in Figure 4.Discussion
This study demonstrates the feasibility of 16-fold accelerated, free-breathing cine MRI for patients with a CIED. Compared with random and Poisson disc sampling patterns, the proposed lattice-like sampling pattern produced sharper images with fewer image artifacts. A future study including a diverse set of CIED patients with different device types is warranted to evaluate the clinical utility of the proposed cine MRI method.Acknowledgements
This work was supported in part by the following grants: NIH R01HL116895, R01HL138578, R21EB024315, R21AG055954References
1. Hundley WG, Bluemke DA, Finn JP, Flamm SD, Fogel MA, Friedrich MG, Ho VB, Jerosch-Herold M, Kramer CM, Manning WJ, Patel M, Pohost GM, Stillman AE, White RD and Woodard PK. ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J Am Coll Cardiol. 2010;55:2614-62.
2. Grothues F, Smith GC, Moon JC, Bellenger NG, Collins P, Klein HU and Pennell DJ. Comparison of interstudy reproducibility of cardiovascular magnetic resonance with two-dimensional echocardiography in normal subjects and in patients with heart failure or left ventricular hypertrophy. Am J Cardiol. 2002;90:29-34.
3. Lustig M, Donoho D and Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn Reson Med. 2007;58:1182-95.
4. Feng L, Srichai MB, Lim RP, Harrison A, King W, Adluru G, Dibella EV, Sodickson DK, Otazo R and Kim D. Highly accelerated real‐time cardiac cine MRI using k–t SPARSE‐SENSE. Magnetic resonance in medicine. 2013;70:64-74.
5. Vasanawala S, Murphy M, Alley M, Lai P, Keutzer K, Pauly J and Lustig M. Practical Parallel Imaging Compressed Sensing Mri: Summary of Two Years of Experience in Accelerating Body Mri of Pediatric Patients. Proc IEEE Int Symp Biomed Imaging. 2011;2011:1039-1043.
6. Tsao J, Boesiger P and Pruessmann KP. k-t BLAST and k-t SENSE: dynamic MRI with high frame rate exploiting spatiotemporal correlations. Magn Reson Med. 2003;50:1031-42.
Figures