4734
3D U-Net for Automated Segmentation of the Thoracic Aorta in 4D-Flow derived 3D PC-MRA1Lurie Childrens Hospital of Chicago, Chicago, IL, United States, 2Northwestern University, Chicago, IL, United States
Synopsis
We developed a 3D convolutional neural network for the automatic segmentation of the thoracic aorta in 4D Flow-derived 3D PC-MRAs. Using 100 testing datasets, we obtained an average dice score of 0.94±0.03 and an average voxel-wise accuracy of 0.99. Additionally, our algorithm is robust enough to accurately segment a wide array of aortic geometries and disease, such as bicuspid aortic value, coarctation, and interrupted aortic arches.
Introduction
Studies have shown the potential of aortic 4D-Flow MRI for the comprehensive characterization and quantification of changes on aortic hemodynamics in common diseases such as aortic valve abnormalities, aneurysm, or dissection. However, 4D-flow data analysis remains time intensive and complex, and despite advances, no automated methods currently exist for advanced processing and quantification across large cohorts. In addition, 4D-flow data analysis is often cumbersome and requires manual interactions. Specifically, 3D segmentation of the aorta, which is often required for subsequent analysis (e.g.3D-WSS), is one of the most time-consuming pre-processing tasks, requiring both anatomic and technical expertise for accurate and reproducible results. As such, a robust, automated segmentation algorithm would accelerate the process of obtaining hemodynamic quantification and improve flow analysis reliability. Previous attempts on automated aortic 3D segmentation have focused on atlas registration and were performed on either short-axis cine MRI or CT images[1-4] from a homogeneous study cohort [5, 6]. However, in a practical clinical or research setting, the automated segmentation algorithm should be 1)based on 4D-flow data alone, and 2)robust across a wide array of aortic geometries and diseases (e.g., BAV, coarctation, interrupted aortic arch). Recent developments in deep learning and convolutional neural networks (CNN) have demonstrated excellent results in the segmentation of MR images in cartilage and musculoskeletal tissue, knee joint tissue, prostrate, and various other anatomical structures[7-9]. In this study, we built on these promising results to develop a 3D CNN for automated 3D segmentation of the thoracic aorta directly from 4D-flow MRI data.Methods
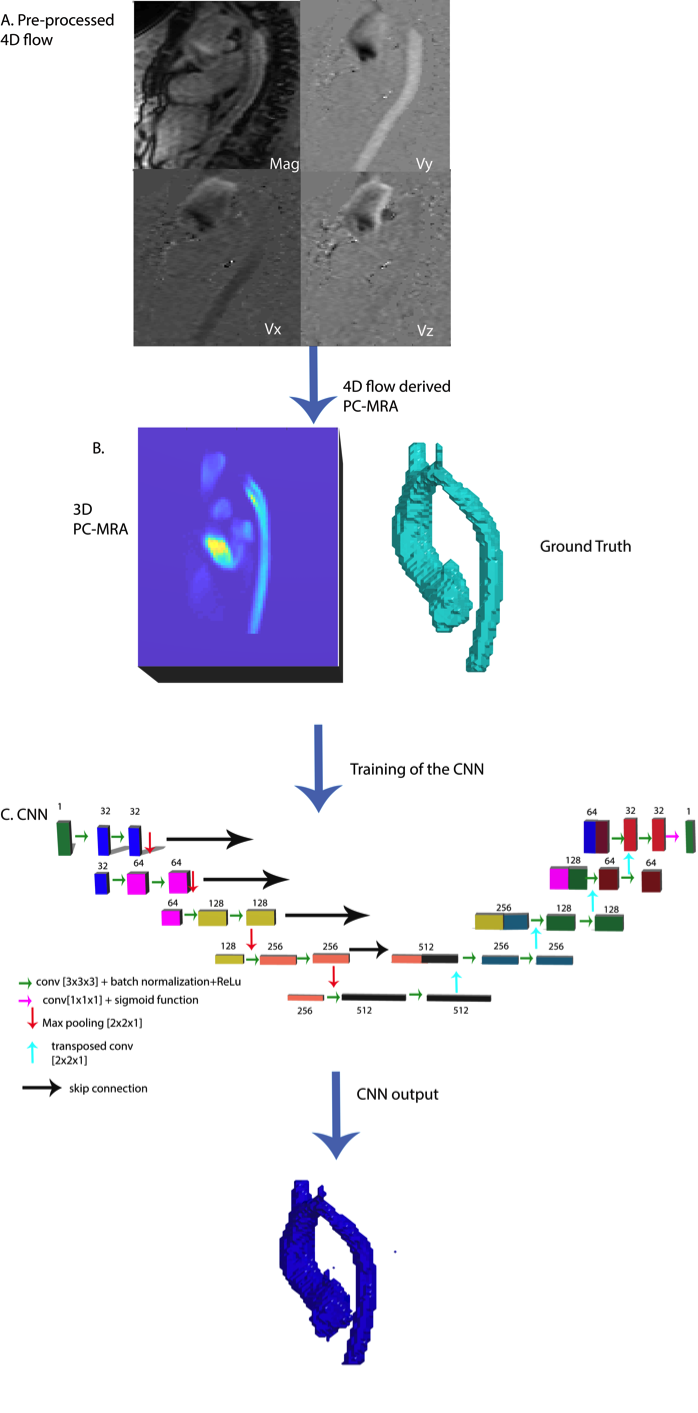
This retrospective study used 210 (100 training, 10 validation, 100 testing) aortic 4D-flow scans (110 male, 13yrs on a 1.5T system (Aera, Siemens, spatial resolution = 1.2-3.5mm3, temporal resolution=37-45ms, venc=120-400cm/s). All 4D-flow datasets were pre-processed for eddy current corrections and noise masking, using a software built in Matlab. 4D-flow derived 3D phase contrast (PC)-MRAs were generated from these data as a basis to conduct a manual 3D segmentation of the thoracic aorta using commercial software (Mimics, Materialise, Belgium). The 3D PC-MRA data were stacked into a 3D array and used as the input for the CNN. The manually obtained 3D segmentations were used as the ground-truth for training. The CNN utilized a 3D Unet architecture, in which there is symmetrical encoder and decoder (Figure 1)[10, 11]. The encoding layers are formed by 2 sets of 3D-convolution, batch normalization, and a linear rectified unit. Max-pooling was applied to half the total number of features across the encoding layer, except in the slice number direction, in order to enable a dynamic input range and promote segmentation consistency across the slices. The decoder layers followed the same structure, except the feature maps were up-sampled to double their dimensions. Additionally, the decoding layer feature maps were concatenated with corresponding encoding layer feature maps in order to retain as much information from the early portions of the network. After the final convolution layer, a sigmoid function was used to generate a probability map across all voxels. A dice loss and a L2 loss function were used to account for the class imbalance in the mask and limited dataset. Additionally, a dropout rate of 0.1 was applied after every convolution layer in order to prevent overfit and obtain more generalizable features across the network. An Adam optimizer was used, and the learning rate was kept constant at 0.0001. Training was performed for 300 epochs.Results
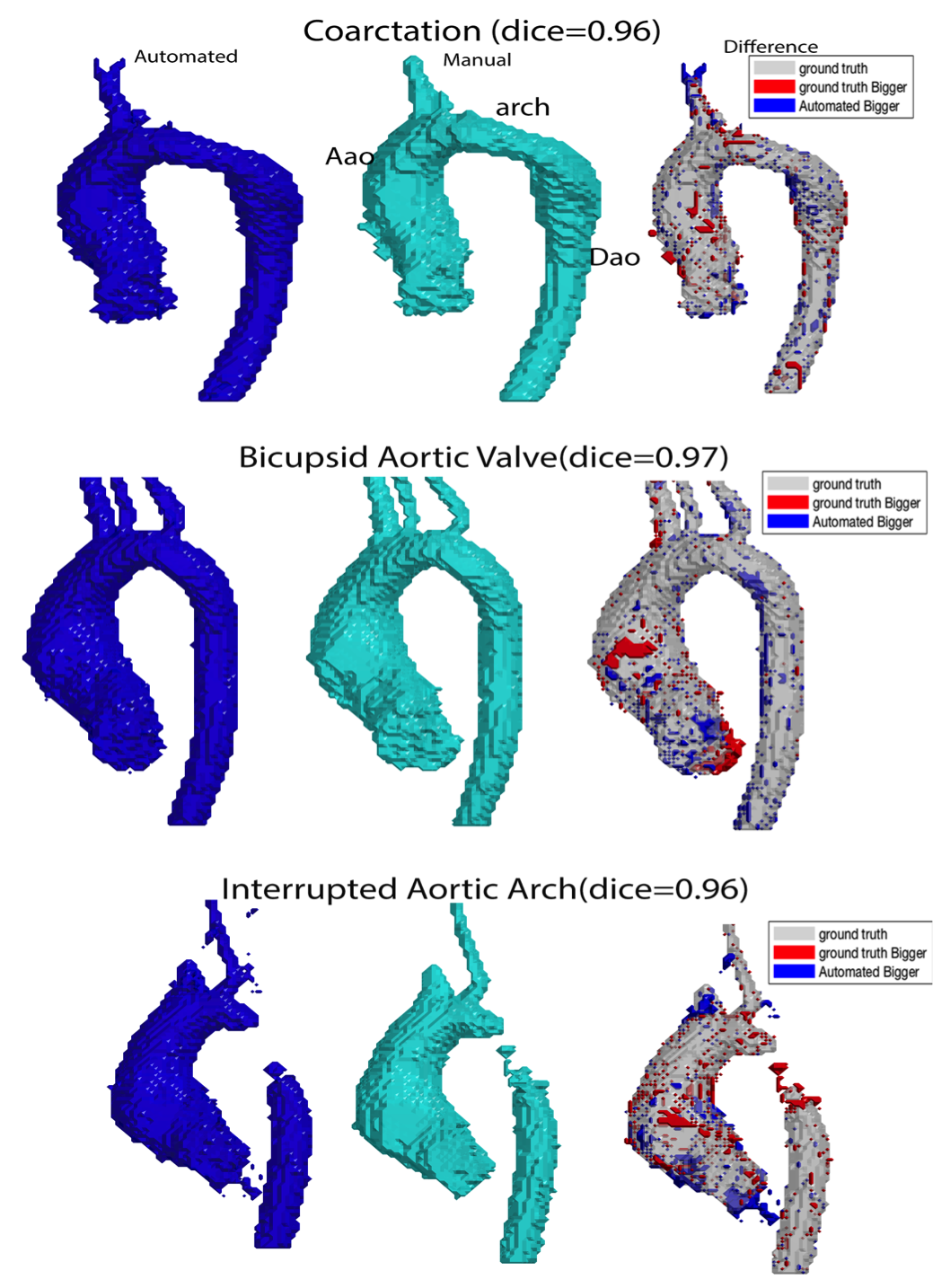
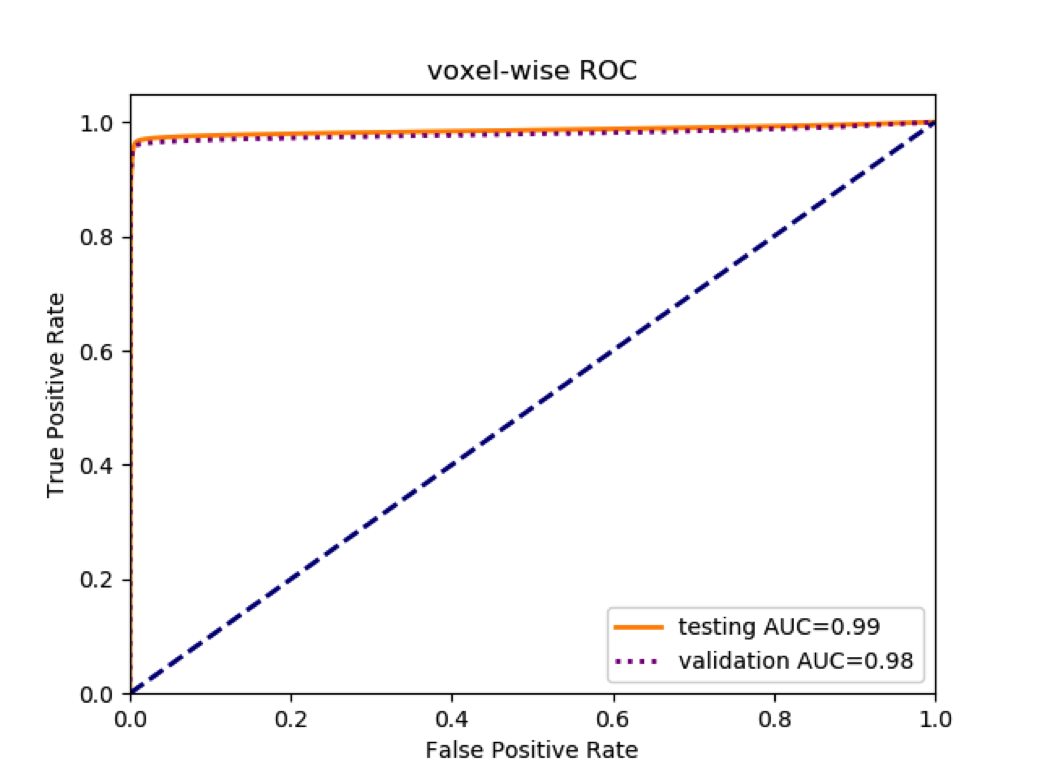
The CNN obtained an average dice score of 0.94±0.03 on the testing dataset and an average dice score of 0.92±0.04 on the validation set. A voxel-wise ROC can be seen in figure 3, with an AUC of 0.99 on the testing dataset. Additionally, the average voxel-wise accuracy, at a decision threshold of 0.5, was 0.99. Figure 2 displays examples of the automated segmentation and the ground-truth for BAV, coarctation, and interrupted aortic arch. The automated segmentation is in very strong agreement with the ground-truth, with the only obvious difference being a patch of the Aao that overlaps with the PA. The total computation on a single dataset was 2 seconds (GPU:GTX 1080-Ti), and the total training time was 150 minutes.Discussion
Our algorithm demonstrated excellent accuracy and robustness, with an average dice score of 0.94 ± 0.03, on par with the highest reported dice score for MR images performed on controls (0.95±0.01) [5]. Future work will progress towards whole heart segmentation and improved discrimination between vasculature, for example our current CNN occasionally includes the SVC as a branch of the aortic, particularly in datasets with more slices.Acknowledgements
No acknowledgement found.References
1. Bustamante, M., et al., Automated multi-atlas segmentation of cardiac 4D flow MRI. Med Image Anal, 2018. 49: p. 128-140.
2. Rohlfing, T., D.B. Russakoff, and C.R. Maurer, Jr., Performance-based classifier combination in atlas-based image segmentation using expectation-maximization parameter estimation. IEEE Trans Med Imaging, 2004. 23(8): p. 983-94.
3. Gibson, E., et al., Automatic Multi-Organ Segmentation on Abdominal CT With Dense V-Networks. IEEE Trans Med Imaging, 2018. 37(8): p. 1822-1834.
4. Odille, F., et al., Automatic segmentation propagation of the aorta in real-time phase contrast MRI using nonrigid registration. J Magn Reson Imaging, 2011. 33(1): p. 232-8.
5. Herment, A., et al., Automated segmentation of the aorta from phase contrast MR images: validation against expert tracing in healthy volunteers and in patients with a dilated aorta. J Magn Reson Imaging, 2010. 31(4): p. 881-8.
6. Duquette, A.A., et al., 3D segmentation of abdominal aorta from CT-scan and MR images. Comput Med Imaging Graph, 2012. 36(4): p. 294-303.
7. Norman, B., V. Pedoia, and S. Majumdar, Use of 2D U-Net Convolutional Neural Networks for Automated Cartilage and Meniscus Segmentation of Knee MR Imaging Data to Determine Relaxometry and Morphometry. Radiology, 2018. 288(1): p. 177-185.
8. Liu, F., et al., Deep Learning Approach for Evaluating Knee MR Images: Achieving High Diagnostic Performance for Cartilage Lesion Detection. Radiology, 2018. 289(1): p. 160-169.
9. Zhu, Y., et al., Fully automatic segmentation on prostate MR images based on cascaded fully convolution network. J Magn Reson Imaging, 2018.
10. Olaf Ronneberger, P.F., Thomas Brox, U-Net: Convolutional Networks for Biomedical Image Segmentation. arXiv, 2015. 1505.
11. Özgün Çiçek, A.A., Soeren S. Lienkamp, Thomas Brox, Olaf Ronneberger, 3D U-Net: Learning Dense Volumetric Segmentation from Sparse Annotation. arXiv, 2016. 1606.
Figures